
Abstract
Targeted temperature management (TTM) is a recognized treatment to decrease mortality and improve neurological function in hypoxic ischemic encephalopathy. An esophageal cooling device (ECD) has been studied in animal models, but human data are limited. An ECD appears to offer similar benefits to intravascular cooling catheters, with potentially less risk to the patient. We studied whether the ECD could act as a substitute for intravascular cooling catheters in delivering adequate TTM after cardiac arrest. Nine patients admitted to the intensive care unit after cardiac arrest who required TTM were enrolled prospectively. The primary outcome measures were timeliness of insertion, ease of insertion, user Likert ratings, time to achieve a target temperature of 36°C, and time during which target temperature was maintained within 1°C of the 36°C goal for 24 hours by using an ECD. Time to reach target temperature was 0 to 540 minutes (mean: 113.33 minutes, median: 0 minute, standard deviation [SD]: 179.22). Maintenance of a target temperature of 36°C over 24 hours had a range of 58.33% to 100% (mean: 91.67%, median: 95.83%, SD: 13.34). Ease of insertion related to Likert ratings with a range of 1–9 (mean: 5.38, median: 5.5, SD: 3.43) and a simplicity of ECD uses a range of 4–10 (mean: 7.63, median: 8.0, SD: 1.65). Overall, there was preference for the ECD over intravascular cooling methods (mean: 6.71, mean: 6, SD: 3.01) and external cooling methods (mean: 8.0, median: 9.0, SD: 2.33). For patients requiring TTM, use of an ECD adequately allowed for TTM goals to be achieved and maintained. Overall, user evaluation was positive.
Introduction
Controlling a patient's temperature after cardiac arrest results in improved odds of favorable outcomes (Bernard et al., 2002; HACA, 2002). Therapeutic hypothermia or targeted temperature management (TTM) has demonstrated a reduction in mortality and improvements in neurological recovery after the return of spontaneous circulation. More recent studies have demonstrated that patients who actively cooled were more likely to reach a favorable neurological outcome than those who did not undergo cooling (risk ratio 1.94, 95% confidence interval [CI] 1.18–3.21) (Arrich et al., 2016). Further, a survival benefit was identified in the group undergoing therapeutic hypothermia as compared with the group without cooling (risk ratio 1.32, 95% CI 1.10–1.65) (Andresen et al., 2015; Vargas et al., 2015; Arrich et al., 2016). Though the original studies evaluated TTM at 32–34°C, several studies have shown no difference in mortality or neurological outcomes at 33°C versus 36°C (Nielsen et al., 2013; Cronberg et al., 2015; Zhang et al., 2015). More recent evidence suggests that a higher temperature target may result in lower compliance to the target and trends toward poorer outcomes (Bray et al., 2017; Salter et al., 2018; Lascarrou et al., 2019; Johnson et al., 2020).
Currently, surface cooling and endovascular cooling are accepted methods for induction of therapeutic hypothermia. Surface cooling can be accomplished with cooling fans, cooling blankets, or ice packs (de Bourmont et al., 2014). Intravascular cooling is an invasive method requiring insertion of a large bore venous catheter with cold saline cycling through a closed circuit. Both methods are effective and have demonstrated effects on mortality or neurological recovery (Deye et al., 2015; Oh et al., 2015). Although no outcome difference was demonstrated, the intravascular method is superior at initiation and stability of the temperature goal (de Waard et al., 2015; Deye et al., 2015). Shivering rates are more likely to reflect the temperature achieved than a particular technique. However, thromboembolic disease rates are increased with intravascular catheters, with rates reported as high as 50% in traumatic brain injury (Simosa et al., 2007).
Esophageal cooling devices (ECDs) have demonstrated effectiveness in temperature management in swine models (Kulstad et al., 2013). An orogastric catheter is inserted and cold saline is circulated through a close circuit to achieve sustained and rapid central temperature reduction. This relatively new method has demonstrated effective temperature control, decreased adverse events, and ease of use (Markota et al., 2016; Naiman et al., 2016; Goury et al., 2017; Hegazy et al., 2017).
Within our institution intensive care units (ICUs), it is current practice to treat patients who present after cardiac arrest with TTM to achieve mild hypothermia (targeted temperature 36°C; goal range 35–36°C) for 24 hours to align with recent TTM publications (Nielsen et al., 2013; Cronberg et al., 2015; Zhang et al., 2015). The American Heart Association, the European Resuscitation Council, the Canadian Critical Care Society, the Canadian Neurocritical Care Society, and the Canadian Critical Care Trials Group recommend TTM with a specific goal temperature set by protocol within a range of 32–36°C (Donnino et al., 2015; Howes et al., 2016). A variety of interventions and devices are currently being used for TTM, with no consensus on the preferred method. External cooling is less invasive, but it is associated with longer cooling times and more temperature variability. Cooling with intravascular cooling catheters provides more rapid cooling with less variation in temperature, but it carries the inherent risks of central venous cannulation, deep venous thrombosis (Maze et al., 2014), and catheter-related thrombosis in non-heparinized patients. Esophageal cooling probes appear to offer similar benefits to intravascular cooling catheters, with potentially less risk to the patient; however, experience using this device is limited.
We aimed at measuring the ease of use, reliability, and effectiveness of esophageal cooling for TTM in a cohort of consecutive patients at our institution. We hoped to determine whether this method could substitute invasive cooling catheters and standardize cooling protocols for TTM in our ICUs and potentially reduce risks for patients.
Methods
This study was approved by the local Review board. This is an observational, feasibility study of consecutive patients admitted to the ICUs at two urban hospitals after cardiac arrest who met indications for TTM. The Rockyview General Hospital and South Health Campus are academic urban hospitals located in Calgary, Alberta, Canada. Twenty critical care and nine coronary care unit beds provide care to patients with out-of-hospital cardiac arrest (OHCA). One to four patients are admitted with OHCA each month at each site. Consecutive patients over the study period were approached. Consent was obtained in ∼10% of eligible patients. Adult patients were included if persistently comatose (Glasgow Coma Scale [GCS] <8) after any cardiac arrest (out or in hospital) and irrespective of cardiac rhythm (whether shocked or not). A patient was eligible if the treating team considered TTM indicated. A protocol for TTM in post-cardiac arrest patients is used across the ICUs in our city. Shivering is controlled with sedation, analgesia, or neuromuscular blockade at the intensivist's discretion. External cooling with ice packs or cooling blankets are variably used in the emergency department at the emergency room physicians' discretion.
The following patients were excluded: pediatric patients (<18 years), intracranial hemorrhage, trauma patients, septic shock, uncontrolled coagulopathy, prior known limitations in goals of care, history of esophageal stricture or diverticulum, known or suspected varices, recent oral or esophageal surgery, weight <40 kg, toxic ingestion of acid or alkali, basal skull fracture, and/or initial temperature <35.5°C.
TTM protocol
Patients admitted to the ICU and for whom the intensivist prescribed TTM (goal of <36°C for 24 hours) underwent placement of the ECD (the Esophageal Cooling Device, Advanced Cooling Therapy, Chicago, IL) in lieu of an oral gastric (OG) tube. The tube was precooled for ease of insertion by connecting it to the standard cooling unit currently employed for cooling blankets and cooling intravascular catheters. The bedside nurse, physician, or nurse practitioner performed tube insertion in a similar fashion to passage of an OG tube. The length of insertion was determined by measuring distance from the earlobe to lips to just below the xiphoid. A jaw thrust was performed if required to position the catheter in the posterior oropharynx. Placement of the esophageal catheter was confirmed by using the standard air insufflation–auscultation technique and a post-insertion chest radiograph. Core temperature monitoring was done by using a Foley thermometer as a primary measurement and rectal temperature as a secondary measurement. The endotracheal tube and esophageal catheter were secured in a standard manner by an endotracheal tube fastener. The esophageal catheter was connected to low-wall intermittent suction. The protocol for an esophageal probe leak, as evidenced by the suction suddenly draining water, was to remove the device from the patient. The cooling unit was set to a target temperature of 36°C. After 24 hours of TTM, rewarming was performed as per usual practice at a rate not exceeding 0.2°C/hour.
Primary outcome measures were time to achieve a target temperature of 36°C after admission to the ICU, percentage of time that target temperature was maintained within 1°C of the 36°C goal for 24 hours, user Likert ratings for ease of insertion, use of the ECD, and preference to intravascular or external cooling (Appendix A).
Additional baseline data included patient demographics, diagnosis, and comorbidities. The presenting vital signs, including GCS, in addition to details of events precipitating the cardiac arrest (initial ECG rhythm), were collected. This study was approved by the Research Ethics Board and Department of Critical Care Medicine at the University of Calgary.
Results
Between October 2017 and April 2019, 10 patients were enrolled and had an ECD inserted for TTM. One patient had early removal of the ECD due to a human error, outside of protocol and data are not included on this patient. Patient characteristics are described in Table 1.
General Patient Demographics on Admission
ICU, intensive care unit.
Primary outcomes
ICU admission to ECD insertion was variable, with a range of 35 to 865 minutes. The mean insertion time was 277.67 minutes, with a median of 207 minutes. The standard deviation (SD) was 255.28 minutes (Fig. 1). The time to temperature goal of 36°C was variable, with a range of 0 to 540 minutes (mean: 113.33 minutes, median: 0 minute, SD: 179.22 minutes) (Fig. 1). Five patients were admitted with a temperature within the goal range. Three patients reached TTM within 200 minutes. Maintenance of a target temperature of 36°C ± 1°C over 24 hours had a range of 58.33% to 100% (mean: 91.67%, median: 95.83%, SD: 13.34) (Fig. 2).
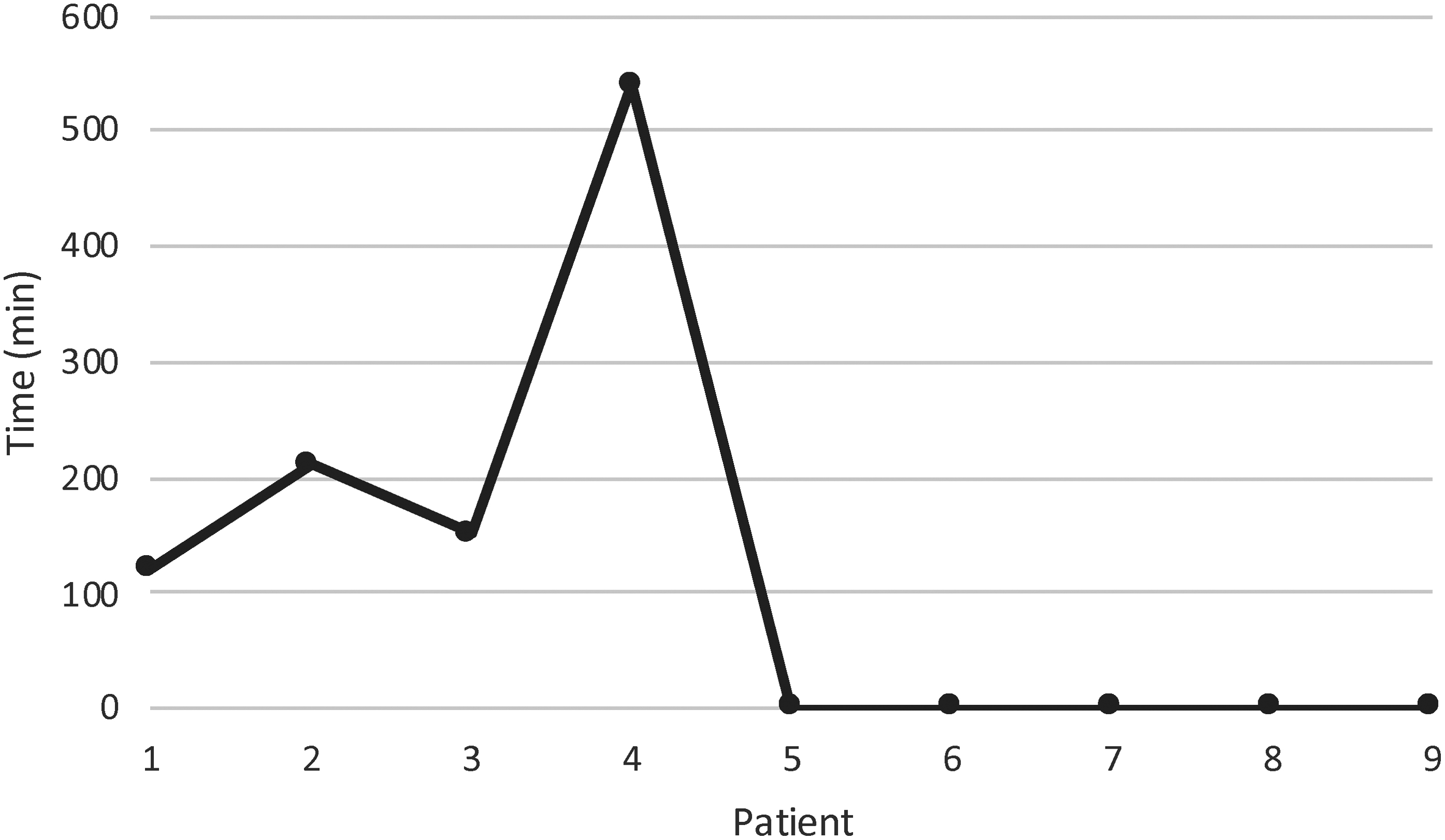
Time to reach TTM of 36°C. TTM, targeted temperature management.
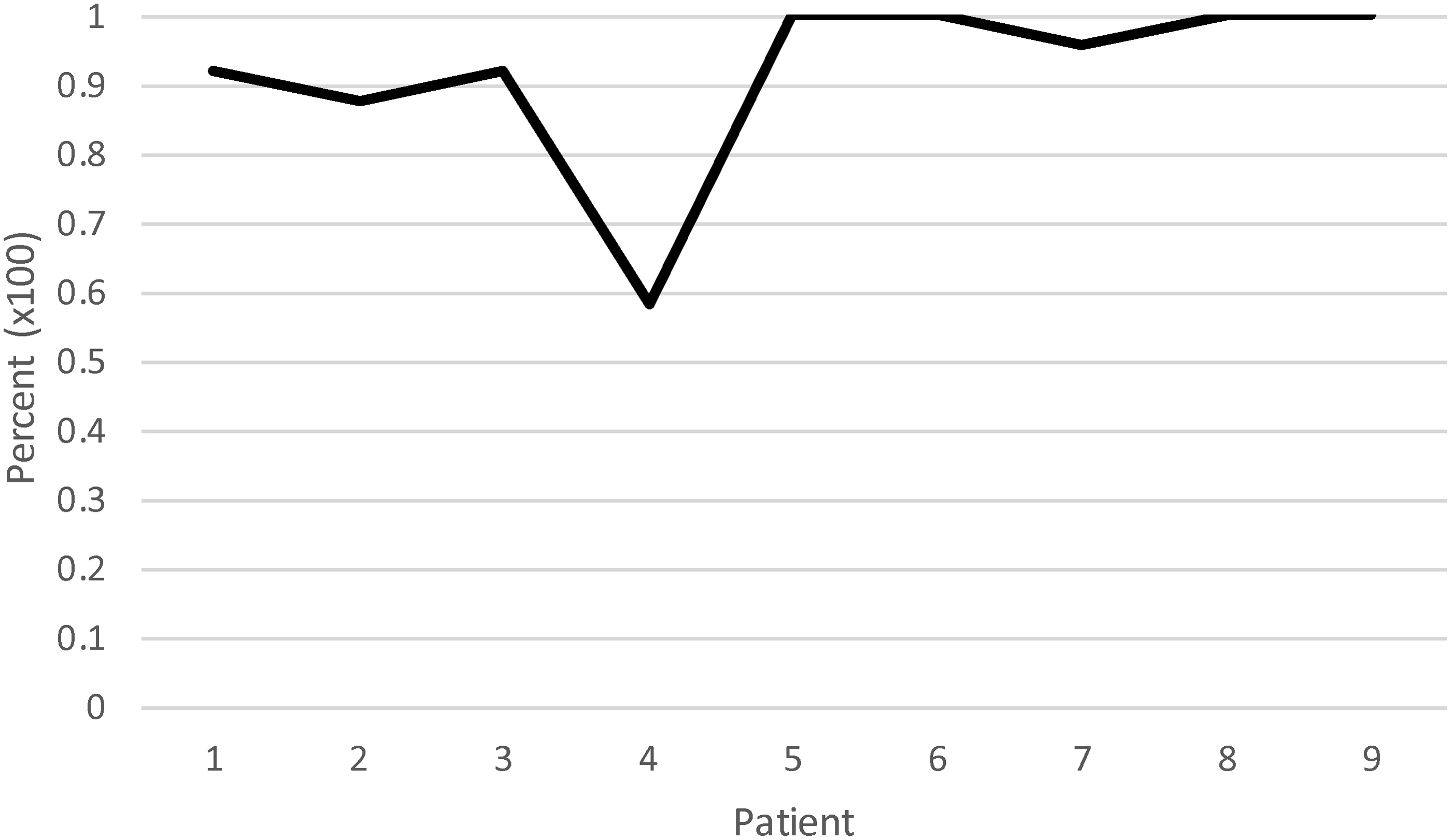
Percentage of time TTM was maintained within 1°C of the 36°C target temperature of a 24-hour period.
Ease of insertion related to Likert ratings produced a range of 1–9 (mean: 5.38, median: 5.5, SD: 3.43), and a simplicity of ECD used a range of 4–10 (mean: 7.63, median: 8.0, SD: 1.65) (Fig. 3). Overall, there was preference for the ECD over intravascular cooling methods (mean: 6.71, mean: 6, SD: 3.01) and external cooling methods (mean: 8.0, median: 9.0, SD: 2.33) (Fig. 3).
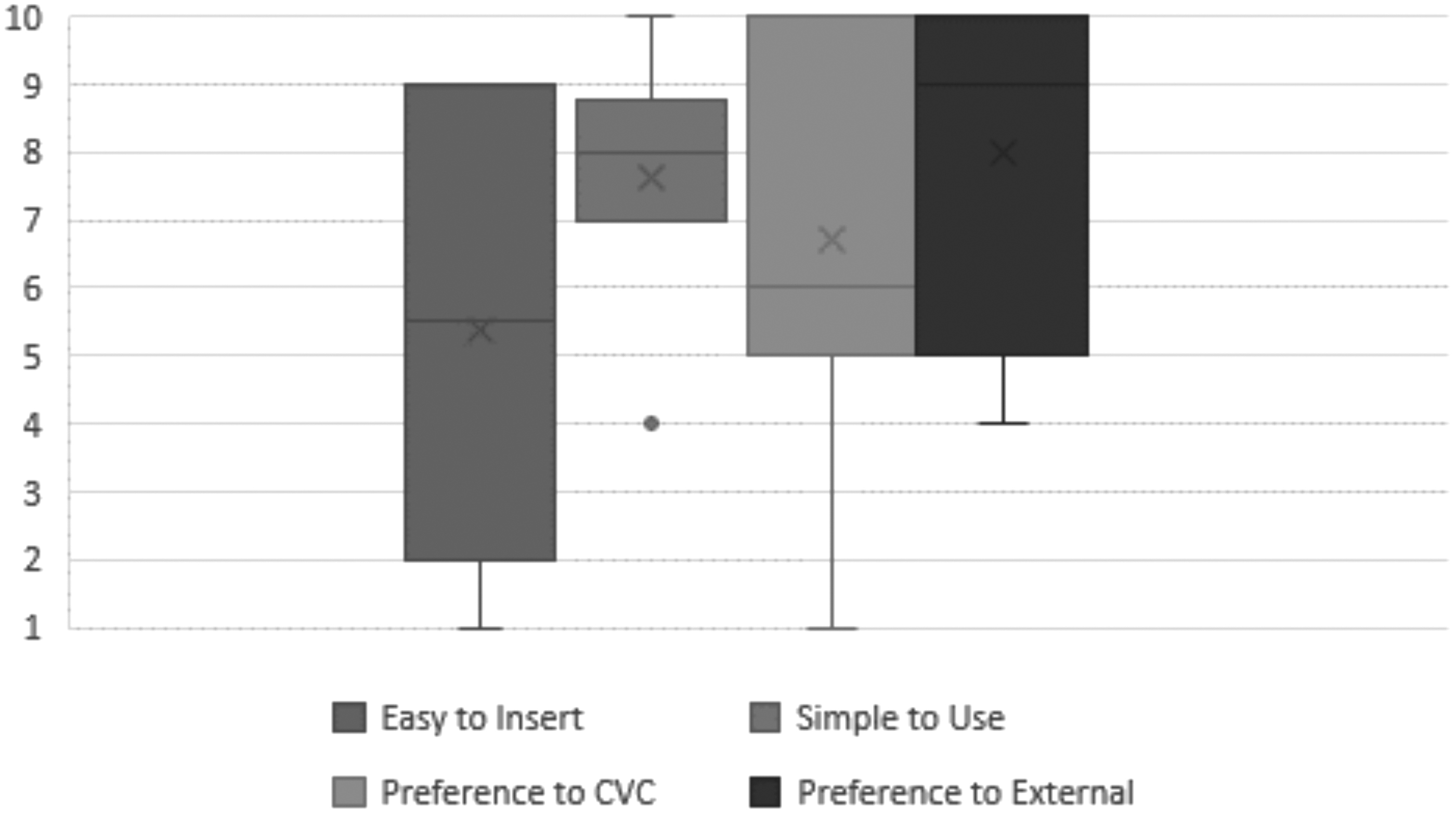
User Likert ratings, scaled 1–10.
Discussion
This prospective feasibility human study describes the successful use of an ECD for TTM after cardiac arrest. The device achieved and maintained a goal temperature of 36°C in most patients. One patient (patient number 4) was as an outlier who had difficult temperature management throughout their post-arrest care. Additional cooling methods in this patient were required; however, the goal temperature was still not achieved for another 300 minutes after this addition. The remainder of the enrolled patients did not require additional cooling methods, nor was any leak reported for the ECDs.
Marked variability was found between admission to the ICU and ECD insertion (<2 to 15 hours). The majority were inserted less than 6 hours after ICU admission. Although ECD insertion was not difficult, TTM initiation via internal cooling was delayed in this cohort in certain patients. These delays may be explained in part by variability in ICU bed availability, need for computed tomography scans before admission, and lack of familiarity with the research protocol. They represent an opportunity for process improvement and will be reviewed by our department's quality improvement committee.
Despite this limitation, ECDs were effective in temperature regulation (cooling rate of 1.12°C/hour, warming rate of 0.22°C/hour), reduced the volume of cooled intravenous fluid administration, and found no adverse effects (Oh et al., 2015). These observations are aligned with other reports (Simosa et al., 2007; de Waard et al., 2015) and support the hypothesis that temperature management can be effectively achieved with the ECD.
Overall, ECDs were easy to insert and use in most patients. One staff member found the ECD to be too flexible and difficult to insert. This was due to a technical error. Instead of pre-cooling the catheter to 4°C before insertion, the temperature was pre-set on the unit at 32°C, effectively warming the catheter and rendering it very flexible. Sharing this information with the ICU team resulted in an improved ease of insertion and overall staff satisfaction with remaining interventions. Another user indicated that the catheter required excess lubrication, and one user found the oropharynx to be crowded. The ECDs are slightly larger than conventional orogastric tubes and it may explain this observation. The use of lubricant is a known required step in the insertion of the ECD. One evaluator did not record Likert scores, but reported overall positive comments with regard to the insertion and use of the ECD. This study aligns with a previous report suggesting that this tool is user-friendly (Goury et al., 2017).
Our study has limitations commensurate to its design. As a feasibility study, the limited sample size is adequate, although it does not permit conclusions about patient outcomes. The study highlights a wide variability in the initiation of internal cooling in this cohort, although external cooling was used before ECD insertion. This observation does not impact our conclusion. This study does not allow us to comment on relative morbidity of intravascular cooling versus esophageal cooling. Each patient is this study had a temperature target of 36°. A lower target would have likely resulted in a longer duration to achieve target temperature.
Conclusions
For patients prescribed TTM, the use of an ECD allowed for targeted temperature goals to be achieved and maintained. The ECDs are easy to insert and use most of the time. We conclude that the ECD is a feasible method of achieving TTM in two urban critical care sites. It appears to be a reasonable option for post-cardiac arrest care. This study provides support for a comparative study of various cooling methods. There has yet to be a study comparing favorable outcomes between other cooling methods, whether invasive or not, and the novel ECD. If achieving a temperature target early is touted to be of most impact to patients, then having access to multiple methods may allow flexibility in treating more patients with success.
Footnotes
Acknowledgments
The authors would like to acknowledge the participation of the families of critically ill patients in Calgary and the support of the nurses in the Department of Critical Care Medicine.
Authors' Contributions
P.M. designed, conducted the study and reviewed the article. T.S. participated in data gathering, study design and wrote the article. P.C. participated in study design and revised the article. P.H. helped with study design and provided support for nurses in use of the catheter. J.K. designed and conducted the study, edited the article, and provided mentorship.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.