
Abstract
We aimed to verify whether slow heart rate (HR) is associated with neurologic outcome and the factors that can contribute to the development of bradycardia in out-of-hospital cardiac arrest (OHCA) survivors who underwent targeted temperature management (TTM). We extracted the data of comatose adult OHCA survivors who underwent TTM between October 2015 and December 2018 from the prospective multicenter registry. Data on HR recorded every 6 hours within 72 hours after return of spontaneous circulation and calculated minimal, mean, and maximal HR and time to the lowest HR were obtained. HR <50 bpm was defined as bradycardia. The primary outcome was a 6-month neurologic outcome based on Pittsburgh-Glasgow Cerebral Performance Category Scale. Of the 814 included patients, 508 (62.4%) had poor neurologic outcome and 197 (24.2%) had bradycardia. Bradycardia (odds ratio [OR], 0.574; 95% confidence interval [CI], 0.362–0.192), minimal HR (OR, 1.023; 95% CI, 1.008–1.037), and mean HR (OR, 1.016; 95% CI, 1.002–1.030) were independently associated with poor neurologic outcome, but not maximal HR and time to the lowest HR. Preexisting arrhythmia (OR, 2.067; 95% CI, 1.037–4.118), renal disease (OR, 2.028; 95% CI, 1.153–3.567), cardiac etiology (OR, 1.526; 95% CI, 1.045–2.228), downtime (OR, 0.985; 95% CI, 0.974–0.996), and serum lactate levels (OR, 0.936; 95% CI, 0.900–0.974) were independently associated with bradycardia. Bradycardia and decreased mean and minimal HR were independently associated with good neurologic outcomes. Bradycardia was associated with preexisting arrhythmia, renal disease, cardiac etiology, shorter downtime, and lower serum lactate level.
Introduction
Targeted temperature management (TTM) is a proven standard treatment that can improve the neurologic outcome of comatose out-of-hospital cardiac arrest (OHCA) survivors (Bernard et al., 2002; Hypothermia after Cardiac Arrest Study Group, 2002; Nielsen et al., 2013). Although the target temperatures of 33°C and 36°C for OHCA patients with presumed cardiac etiology have similar neurologic outcomes (Nielsen et al., 2013), a recent research revealed that a target temperature of 33°C is a more effective measure than normothermia to improve the neurologic outcome of cardiac arrest patients with nonshockable rhythm who are generally expected to have a worse neurologic prognosis (Lascarrou et al., 2019). This finding suggests that a target temperature of 33°C has more potent neuroprotective effect in comatose OHCA survivors. However, moderate therapeutic hypothermia (TH) has more profound physiological effects on core temperature than mild hypothermia. Bradycardia is a noteworthy change as the body temperature decreases during TH (Polderman and Herold, 2009).
Bradycardia (<50 bpm) was observed in 30–50% of OHCA patients during TH (Thomsen et al., 2015, 2016), while 10–13% of OHCA patients developed severe bradycardia (<40 bpm) (Nielsen et al., 2009; Kim et al., 2015). Previous studies showed that bradycardia during TH is associated with good neurologic outcome or survival (Staer-Jensen et al., 2014; Thomsen et al., 2015, 2016). Although bradycardia presenting during TH can be an early prognostic marker of OHCA, previous studies obtained the data on heart rate (HR) at limited time points, had small sample size, or had no findings on the association between HR and blood pressure (Staer-Jensen et al., 2014; Thomsen et al., 2015, 2016; Oksanen et al., 2018). The factors associated with the development of bradycardia during TTM and the association between HR and outcome based on the etiology of cardiac arrest remain unknown.
To address these points, we hypothesized that bradycardia as a binary value and HR as a continuous value are associated with the neurologic outcomes. Hence, we aimed to verify the association between HR and neurologic outcome in a prospective, large multicenter cohort of comatose OHCA survivors who underwent TTM. We also aimed to assess the factors contributing to the development of bradycardia during TTM and the association between bradycardia and blood pressure change over time.
Methods
Study design and population
This is a prospective, multicenter, observational cohort study. Korean Hypothermia Network prospective registry (KORHN-PRO; NCT02827422) has been collecting the data on adult (≥18 years) comatose (who do not follow verbal commands) OHCA survivors who underwent TTM from 20 participating hospitals in South Korea in accordance with the Utstein-style guidelines between October 2015 and December 2018 (Perkins et al., 2015). Institutional review board of all participating hospitals approved this study. A written informed consent was obtained from all patients in accordance with national requirements and the principle of the Declaration of Helsinki.
The participating hospitals provided postcardiac arrest care according to the standard TTM protocol at each hospital. KORHN-PRO excluded patients with suspected or confirmed acute ischemic or hemorrhagic stroke, poor prearrest neurologic status with Cerebral Performance Category (CPC) scale of 3 or 4, known limitations in therapy and on do-not-resuscitate status, a disease that made 180 days survival unlikely, a body temperature of <30°C, and refusal to provide informed consent. An independent commission assessed the neurologic outcomes 6 months after return of spontaneous circulation (ROSC) through telephone interview using the Pittsburgh Glasgow CPC scale (Booth et al., 2004).
We included adult comatose OHCA survivors who underwent TTM with a target temperature of 33°C and excluded patients who were supported with extracorporeal membrane oxygenation (ECMO), had a target temperature more than 33°C or a prolonged TTM (>24 hours), died within 72 hours after ROSC, had a pacemaker insertion within 72 hours after ROSC, with missing data on HR within 72 hours, and with missing data on neurologic outcome 6 months after ROSC.
Targeted temperature management
Comatose OHCA patients were cooled with target temperature of 32–36°C as early as possible. Various feedback cooling devices available in each hospital were used for TTM. Patients received analgosedatives and neuromuscular blocker as needed according to local protocols of each hospital. Patients were rewarmed at the rate of 0.2–0.5°C/h after maintenance phase. Body temperature was monitored to avoid the development of fever at least 72 hours after completion of TTM.
Data collection
We extracted the following data from KORHN-PRO: age, sex, preexisting illness, witness, bystander cardiopulmonary resuscitation, the first monitored rhythm (shockable or nonshockable), cardiac arrest etiology (cardiac or noncardiac), downtime (time from collapse to ROSC), lactate levels after ROSC, QTc interval on electrocardiogram, use of inotrope or vasopressor (epinephrine, norepinephrine, dopamine, dobutamine, and vasopressin) during TTM, preinduction duration (time from ROSC to initiation of TTM), induction duration (time from initiation of TTM to achievement of target temperature), HR and mean arterial blood pressure (MBP) every 6 hours within 72 hours after ROSC, and neurologic outcomes within 6 months after ROSC.
We defined bradycardia as a HR of <50 bpm and calculated the mean HR, minimal HR, maximal HR, time to the lowest HR after ROSC, and average MBP. The primary outcome was neurologic outcomes 6 months after ROSC; it was dichotomized into good (CPC 1 or 2) or poor (CPC 3–5) neurologic outcomes.
Statistical analysis
We used descriptive statistics to summarize the data. We report counts with percentages for categorical variables and median with interquartile range for continuous variables since all continuous variables had non-normal distribution. We used the chi-square test with continuity correction or Fisher's exact test for categorical variables and Mann–Whitney U test for continuous variables. We used the multivariate logistic regression analysis to identify variables associated with bradycardia and to determine whether bradycardia or HR was independently associated with neurologic outcome. We selected the variables with p < 0.20 in univariate analyses as covariates for multivariate analysis. We used a backward stepwise approach to build the final regression model and evaluated the goodness of fit using the Hosmer–Lemeshow test. The final model included age, hypertension, witness, first monitored rhythm, cardiac arrest etiology, downtime, lactate, norepinephrine, and vasopressin to investigate the association between HR variables and outcome. We report logistic regression analysis results as odds ratio (OR) with 95% confidence interval (CI). We used linear mixed analyses to investigate the changes in HR or MBP over time within 72 hours after ROSC in the neurologic outcome groups (good and poor neurologic outcome groups) and bradycardia groups (bradycardia and nonbradycardia groups). We performed post hoc analyses with Mann–Whitney U-test with Bonferroni correction.
To reduce the selection bias on the effect of potential confounding factors, we calculated a propensity score for the development of bradycardia using a multivariate logistic regression model based on variables, with p < 0.2 between the bradycardia and nonbradycardia groups (Table 2). Propensity score matching was performed in a one-to-one manner between the two groups using calipers with a width equal to 0.2 standard deviation of the logit of the propensity score. The significance level was set as p < 0.05. Data were analyzed using the PASW/SPSS™ software, version 18 (IBM, Inc., Chicago, IL).
Baseline Characteristics Stratified by Bradycardia
Included number for analysis.
CPR, cardiopulmonary resuscitation; IQR, interquartile range; PCI, percutaneous coronary intervention.
Results
Study population
During the study period, 1373 of 10,258 comatose OHCA survivors underwent TTM. Of them, 59 patients underwent ECMO, 211 had a target temperature more than 33°C, 21 underwent prolonged TTM, 231 died within 72 hours after ROSC, 5 had a pacemaker insertion within 72 hours after ROSC, 1 had missing data on HR, and 31 had missing data on neurologic outcome within 6 months. A total of 814 patients were included in the final analysis (Fig. 1).
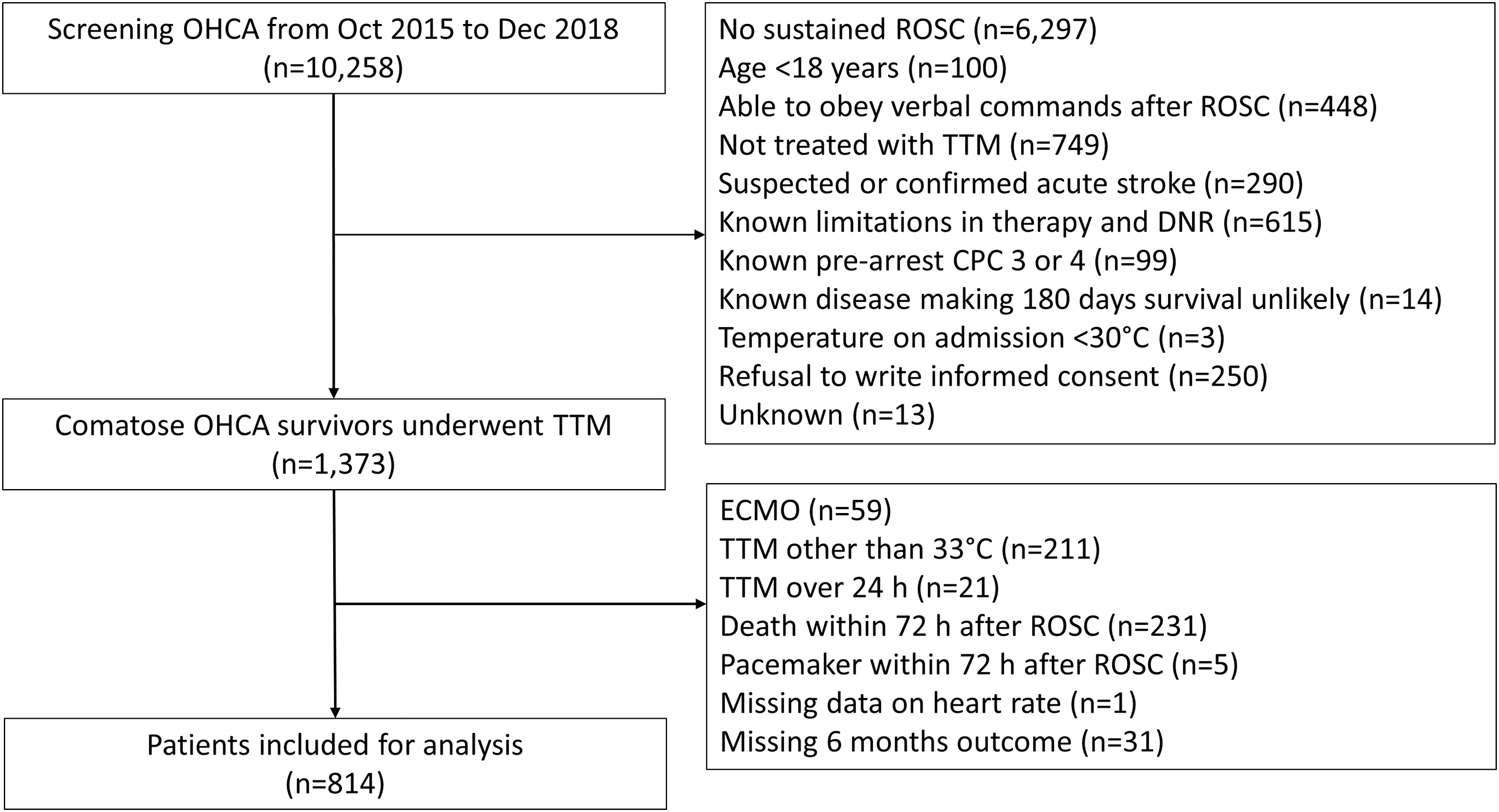
Flow diagram of patient inclusion. CPC, Cerebral Performance Category; DNR, do not resuscitate; ECMO, extracorporeal membrane oxygenation; OHCA, out-of-hospital cardiac arrest; ROSC, return of spontaneous circulation; TTM, targeted temperature management.
Table 1 shows the baseline characteristics of the study population. Poor neurologic outcome at 6 months after ROSC was observed in 508 (62.4%) patients. The poor neurologic outcome group was older and comprised more female patients. The poor neurologic outcome group was more likely to have higher preexisting illness (hypertension, diabetes mellitus, pulmonary disease, and renal disease), less likely to be witnessed, less likely to have a shockable rhythm and cardiac etiology, had a longer downtime, had a higher serum lactate after ROSC, had a longer QTc, and required more epinephrine, norepinephrine, dopamine, and vasopressin. The mean and minimal HRs within 72 hours after ROSC were significantly different between the good neurologic outcome group and poor neurologic outcome group, whereas the maximal HR within 72 hours after ROSC was not different between groups. The lowest HR was observed 24 hours after ROSC, and the good outcome group had a shorter time to the lowest HR.
Baseline Characteristics of the Study Population Stratified by Neurologic Outcome After 6 Months
Included number for analysis.
CPR, cardiopulmonary resuscitation; HR, heart rate; IQR, interquartile range; PCI, percutaneous coronary intervention.
Factors associated with development of bradycardia
Bradycardia developed in 197 (24.2%) patients within 72 hours after ROSC. Severe bradycardia (<40 bpm) developed in 66 (8.1%) patients. Table 2 shows the baseline characteristics between bradycardia and nonbradycardia groups. The bradycardia group was older and was more likely to have preexisting illness (previous acute myocardial infarction, angina, arrhythmia, renal disease, and previous percutaneous coronary intervention), a shockable rhythm, and a cardiac etiology. The bradycardia group had a shorter downtime, a lower serum lactate, and used less dopamine.
Table 3 shows the results of the multivariate regression analysis of factors that can predict the development of bradycardia. Preexisting arrhythmia (OR, 2.067; 95% CI, 1.037–4.118), renal disease (OR, 2.028; 95% CI, 1.153–3.567), cardiac etiology (OR, 1.526; 95% CI, 1.045–2.228), shorter downtime (OR, 0.985; 95% CI, 0.974–0.996), and lower serum lactate (OR, 0.936; 95% CI, 0.900–0.974) are associated with development of bradycardia within 72 hours after ROSC. Use of inotrope or vasopressor was not independently associated with development of bradycardia.
Multivariate Logistic Regression Analysis of Independent Predictors of Bradycardia
aOR, adjusted odds ratio; CI, confidence interval; PCI, percutaneous coronary intervention.
Association of HR variables and bradycardia with neurologic outcome
Table 4 shows the results of the multivariate regression analyses of poor neurologic outcome. Time to the lowest HR was not associated with neurologic outcome. Bradycardia (OR, 0.574; 95% CI, 0.362–0.912), mean HR (OR, 1.016; 95% CI, 1.002–1.030), and minimal HR (OR, 1.023; 95% CI, 1.008–1.037) within 72 hours after ROSC were independently associated with poor neurologic outcome, whereas maximal HR was not associated with neurologic outcome.
Multivariate Logistic Regression Analyses of Bradycardia and Heart Rate Variables Associated with Poor Neurologic Outcome
Adjusted with age, hypertension, witness, shockable rhythm, cardiac etiology, downtime, lactate, norepinephrine, and vasopressin.
aOR, adjusted odds ratio; CI, confidence interval; CPR, cardiopulmonary resuscitation; HR, heart rate; NA, not applicable.
The cardiac etiology group had lower minimal HR and higher incidence of bradycardia than the noncardiac etiology group (Fig. 2). We analyzed the association between HR and outcome apart from the etiology of cardiac arrest. Higher minimal HR (OR, 1.024; 95% CI, 1.006–1.041) was independently associated with poor outcome in the cardiac etiology group, while bradycardia (OR, 0.308; 95% CI, 0.114–0.830) was independently associated with poor neurologic outcome in the noncardiac etiology group (Fig. 2).
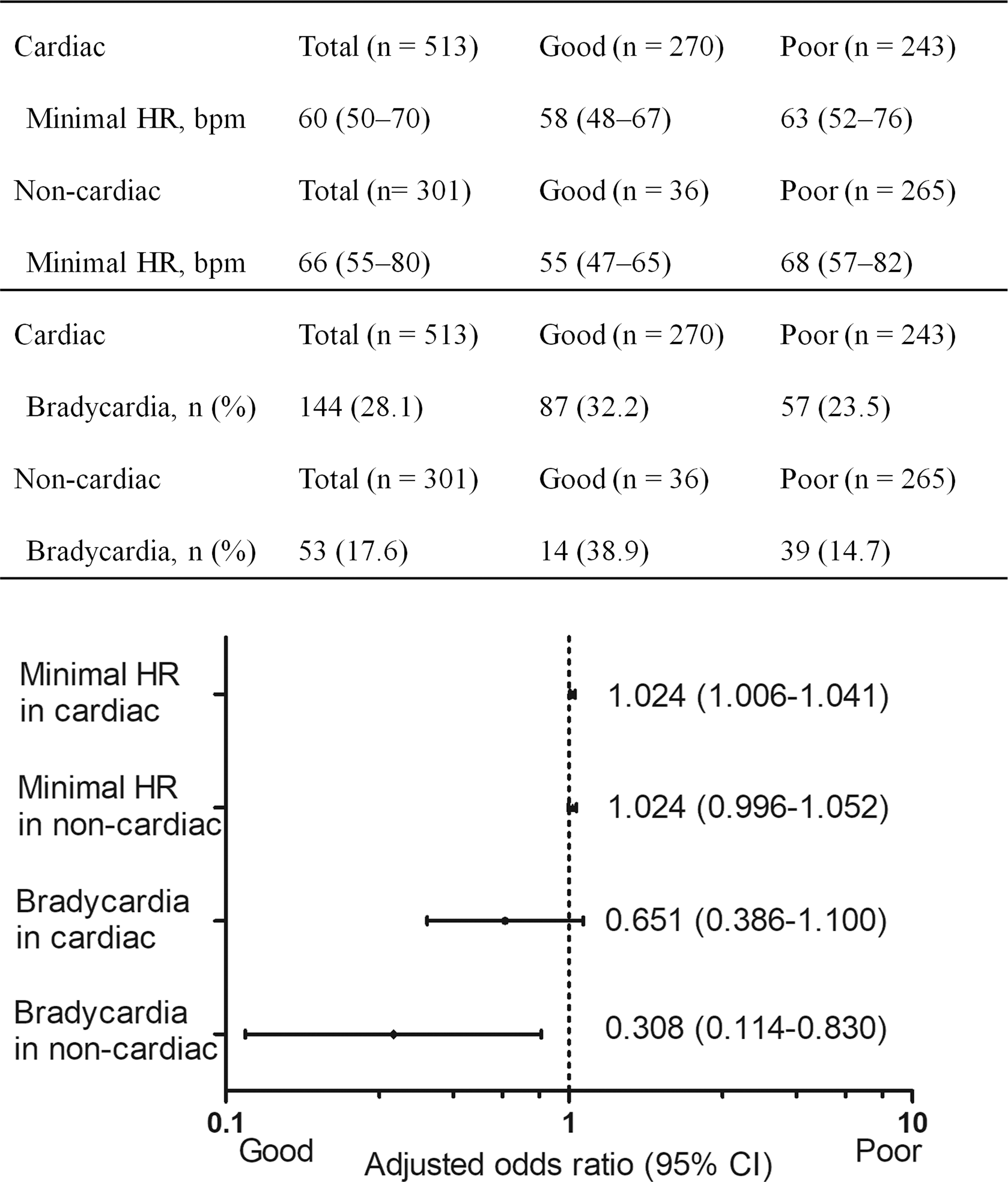
The association of minimal heart rate and bradycardia with neurologic outcome stratified by cardiac etiology and noncardiac etiology groups. The higher minimal heart rate is independently associated with poor neurologic outcome in cardiac etiology group, and bradycardia is independently associated with good neurologic outcome.
Changes in HR and mean blood pressure within 72 hours after ROSC
Figure 3 shows the changes in HR and mean blood pressure stratified by neurologic outcome and bradycardia groups. HR significantly changed over time within 72 hours after ROSC irrespective of neurologic outcome or bradycardia groups, and HR reached the minimal value during TTM. The poor outcome group had significantly higher HR within 48 hours after ROSC; meanwhile, the bradycardia group had significantly lower rates throughout the 72 hours after ROSC (Fig. 3). The mean blood pressure changed over time within 72 hours after ROSC irrespective of neurologic outcome or bradycardia severity. The mean blood pressure was not different between the bradycardia group and nonbradycardia group at any time within 72 hours after ROSC. However, the poor neurologic outcome group had significantly lower MBP within 6 hours after ROSC and 42–72 hours after ROSC.

Changes in the heart rate and mean blood pressure stratified by neurologic outcome and bradycardia.
Analysis of propensity score-matched cohort
Each group included 184 of 368 patients after matching, and the balance between the bradycardia and nonbradycardia groups was improved (Supplementary Table S1). The poor neurologic outcome was 48.4% and 53.8% in the bradycardia and nonbradycardia groups, respectively (p = 0.348).
Discussion
In this observational study, we found that bradycardia <50 bpm and slow HR are independently associated with good neurologic outcome at 6 months after ROSC in OHCA survivors who underwent TTM. Minimal HR in the cardiac etiology group and bradycardia in the noncardiac etiology group were independently associated with neurologic outcome. Preexisting arrhythmia, renal disease, cardiac etiology, shorter downtime, and lower serum lactate contributed to the development of bradycardia. Use of inotrope or vasopressor was not associated with bradycardia. After balancing contributing factors to bradycardia, bradycardia was found to be not associated with the neurologic outcomes. The bradycardia group had an MBP comparable to that of the nonbradycardia group within 72 hours after ROSC.
The independent association of bradycardia or slow HR with good neurologic outcome in the present study is in line with that reported in previous studies (Staer-Jensen et al., 2014; Thomsen et al., 2015, 2016; Oksanen et al., 2018). The slow HR associated with lower body temperature is a physiological reaction, which indicates intact autonomic response (Polderman, 2009). The brain–heart interaction can explain the role of bradycardia as a prognosticator in cardiac arrest survivors. Although brain injury differs depending on the location and type, the catecholamine release pathway has a common central role in the brain–heart interaction (Oppenheimer, 1994; Nguyen and Zaroff, 2009; Krishnamoorthy et al., 2016).
Therefore, patients with global brain injury following a cardiac arrest can present with autonomic dysfunction according to the severity of brain injury. A recent prospective study showed that HR variability related variables, which are known to be markers of autonomic dysfunction, have good prognostic performance in OHCA patients who underwent TTM (Endoh et al., 2019). The autonomic dysfunction of a severely injured brain might mitigate the negative chronotropic action of TTM. The HR between good and poor neurologic outcome groups was not different after the completion of TTM, while the HR was consistently different during TTM and reached the lowest HR in the middle of TTM in the present study. This finding implies that the autonomic responsiveness to temperature management was different between neurologic outcome groups. Therefore, the changes in HR in response to body temperature changes can be used as an early prognostic marker in OHCA patients who underwent TTM.
This finding is consistent with that in the previous study, which validated the independent association of bradycardia during first 24 hours after ROSC and neurologic outcome (Thomsen et al., 2016). Contrastingly, a recent study showed that the bigger difference between post-rewarming and pre-rewarming HRs was associated with good neurologic outcome in OHCA survivors who underwent TH (Inoue et al., 2018). Although the maximal HR was mostly observed during the rewarming phase, the maximal HR had no association with neurologic outcome unlike minimal or mean HRs, because the maximal HR itself does not reflect the changes in HR as rewarming.
Minimal HR is a quantitative value for slow HR, while bradycardia is a qualitative value. Not all of them had a significant association with neurologic outcome in each of the cardiac and noncardiac etiology groups in the present study. The cardiac etiology group had profound bradycardia compared with the noncardiac etiology group, which seemed to contribute to the insignificant association between bradycardia <50 bmp and neurologic outcome in the cardiac etiology group. Although the noncardiac group had a wider difference in minimal HR between neurologic outcome groups than the cardiac etiology group, worse neurologic outcome and the heterogeneity of noncardiac etiology might contribute to the insignificant association between minimal HR and outcome after adjustment. Nevertheless, both sole groups have the same directional association between slow HR and good neurologic outcome.
An observation study on invasive hemodynamic monitoring revealed that MBP decreased while cooling, whereas left ventricular contractility increased in OHCA patients who underwent TTM (Chen et al., 2019). The group with good neurologic outcomes had higher MBP between 42 and 72 hours after ROSC. However, both neurologic outcome groups had stable MBP throughout the TTM; although the bradycardia group might have decreased cardiac output, the bradycardia and nonbradycardia groups had similar stable MBP within 72 hours after ROSC. This finding suggests that stroke volume is increased or at least preserved during cooling, as previous studies revealed that left stroke work index increased with cooling (Chen et al., 2019).
The factors contributing to the development of bradycardia in the present study were as follows: arrhythmia, cardiac etiology, and less ischemic insult (shorter downtime and lower serum lactate). Although previous studies did not describe the factors contributing to the development of bradycardia, the candidates might be inferred from the difference in the baseline characteristics between the bradycardia group and nonbradycardia group (Thomsen et al., 2015, 2016). One previous research showed similarly that the bradycardia group had a shorter downtime and a lower serum lactate, and another previous study showed that the bradycardia group was younger and had more preserved left ventricular systolic function (Thomsen et al., 2015, 2016). Although myocardial dysfunction had no association with outcome (Yao et al., 2018; Grand et al., 2019), a shorter downtime, lower lactate level, and younger age are generally associated with good outcomes in cardiac arrest survivors (Kim et al., 2016; Lee et al., 2017; During et al., 2018). Considering those factors, the association between bradycardia and contributing factors might enhance the early prognostic role of slow HR or bradycardia in cardiac arrest survivors. The disappearance of an association between bradycardia and neurologic outcomes after balancing the contributing factors to bradycardia implies that bradycardia might have a comprehensive role by summarizing the contributing factors.
A previous study showed that the bradycardia group used less epinephrine and norepinephrine within 24 hours after ROSC (Staer-Jensen et al., 2014). However, the vasopressor or inotropes were not associated with bradycardia irrespective of having β adrenergic agonist prophecy in the present study. Although use of norepinephrine or vasopressor was associated with poor neurologic outcome, those had no association with bradycardia in the present study, which might support that bradycardia during TTM is irrelevant to the vasopressor/inotrope use.
This study has several limitations. Although the present study used a prospectively collected large sample from multicenter, we can only provide the association due to the observational nature of the study. The results of the present study are not generalizable to patients with a target temperature other than 33°C because bradycardia is a kind of physiologic response against cooling and the HR depends on the depth of hypothermia. Therefore, we only included patients with a target temperature of 33°C. The registry has no data on the medication that the patients took before the cardiac arrest occurred, which possibly affected the HR. The significant association between bradycardia and the preexisting arrhythmia might come due to the medication, which can be a potential confounder. Sedatives might also affect the development of bradycardia. Not all patients were administered analgosedatives, which might be a confounder. Previous studies used cardiovascular sequential organ failure assessment subscore to adjust the hemodynamic status. Instead, we analyzed the use of inotrope/vasopressor within 24 hours after ROSC to directly examine the association between bradycardia and inotrope/vasopressor during postcardiac arrest care. This study only included the patients who underwent a TTM of 33°C to determine the homogeneity of the target group. However, the TTM trial showed a similar incidence of bradycardia that required pacing between the group with a target temperature of 33°C and that with a target temperature of 36°C (Nielsen et al., 2013). Future research is warranted to investigate the association between HR and outcome in patients with a TTM of more than 33°C. We did not distinguish the types of bradycardia. Instead, we excluded patients who required a pacing therapy. We did not have data on cardiac function after ROSC and HR variability, which is the appropriate parameter to assess autonomic function.
Conclusion
Bradycardia and slow HR within 72 hours after ROSC are independently associated with good neurologic outcome 6 months after ROSC in OHCA survivors who undergo a TTM of 33°C. Bradycardia <50 bpm is associated with preexisting arrhythmia, renal disease, cardiac etiology, shorter downtime, and lower serum lactate level, but not with inotrope/vasopressor use. Individuals with and without bradycardia have similar stable MBP 72 hours after ROSC.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.