
Abstract
Fever may aggravate secondary brain injury after traumatic brain injury (TBI). The aim of this study was to identify episodes of temperature increases through visual plot analysis and algorithm supported detection, and to describe associated patterns of changes in on brain tissue oxygen tension (PbtO2). Data derive from the high-resolution cohort of the multicenter prospective Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI) study. Temperature increases (
Introduction
Severe traumatic brain injury (TBI) is a devastating disease that is still associated with a considerable rate of morbidity and mortality despite tremendous improvements in the critical care management (Steyerberg et al., 2019). Systemic complications, including fever frequently occur in the early phase after trauma and likely exacerbate secondary brain injury (Walter et al., 2016). Up to 50% of patients following acute brain injury develop fever within the hospitalization time (Kilpatrick et al., 2000). While deleterious effects of fever and their association with unfavorable outcomes are well described (Greer et al., 2008), underlying pathophysiologic mechanisms are still not fully elucidated. Fever is associated with multiple systemic and cerebral changes, such as an increased metabolic demand (Busija et al., 1988; Holtzclaw, 1992), increased endogenous stress levels, alterations in blood pressure levels (Walter et al., 2016), increases in cardiac output and heart rate (HR) (Bain et al., 2014), hyperventilation, the synaptic release of excitatory amino acids (Stocchetti et al., 2005), elevated intracerebral pressure (ICP) levels (Rossi et al., 2001; Stocchetti et al., 2005; Nyholm et al., 2017), ischemic cortical depolarizations, and blood–brain barrier breakdown (Wang et al., 2014).
Assessing brain tissue oxygen tension (PbtO2) along with other hemodynamically relevant factors during episodes of temperature increases may provide insight into changes in oxygen supply and consumption (Le Roux et al., 2014). Most data investigating the influence of different temperature levels on cerebral oxygenation are derived from animal studies or from human studies in which mostly patients with hypothermia were studied (Tokutomi et al., 2003; Zhi et al., 2003; Flynn et al., 2015). Some studies in humans (Stocchetti et al., 2005; Spiotta et al., 2008; Nyholm et al., 2017) assessed the association between PbtO2 and fever and report no significant decrease of PbtO2 levels during fever. However, little is known how changes in body temperature (in particular increases) influence brain tissue oxygen tension, irrespective of the absolute temperature.
In this study, we aimed to quantify changes in PbtO2 during temperature increases in severe TBI patients and to explore simultaneous changes of hemodynamic parameters and the cerebral autoregulatory state (cerebral perfusion pressure, CPP; mean arterial pressure, MAP; HR; pressure reactivity index, PRx; oxygen reactivity index, ORx). Moreover, we intended to compare episodes of temperature increases identified through visual plot analysis and by algorithm-supported detection. Our primary hypothesis was that the rise in temperature carries the risk of brain tissue hypoxia, explained by hemodynamic changes.
Methods
Study population
In the intensive care unit (ICU) stratum of the Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI, registered at clinicaltrials.gov NCT02210221) core study, high-resolution data were collected in a subset of 277 patients admitted to 21 European centers. Of these, 102 patients were selected with reliable continuous temperature recordings. Thirty-three patients had additional monitoring of PbtO2 and were included in the final analysis. Patients were recruited from January 2015 until December 2017. These patients were admitted to the ICU following a moderate (initial Glasgow Coma Scale [GCS] 9–12) or severe (GCS ≤8) TBI. Few patients initially suffered from mild-to-moderate TBI but deteriorated early prompting ICU admission. Insertion of ICP probes confirmed to BTF (Brain Trauma Foundation) guidelines in all patients (Carney et al., 2017). Therefore, a multimodal neuromonitoring bundle was only initiated in patients with severe TBI on admission or in those with neurologic deterioration. Data collection in the CENTER-TBI study adhered to ethical standards and the study was approved by the Medical Ethics Committees of all participating centers. Informed consent was obtained in accordance with local regulations (Steyerberg et al., 2019). The Austrian Ethics approval is given as an example (Medical University of Innsbruck, AN2014-0336 343/4.22). The list of ethics committee approvals of participating sites is online. *
Data collection and preprocessing
All demographic variables were prospectively collected and entered in an electronic case report form (Quesgen, Inc., Burlingame, CA) after interpretation by physicians and/or research assistants. Clinical data were collected on a daily basis: at ICU admission, during ICU stay (days 1–7, 10, 14, 21, 28), and at ICU discharge. Demographic variables were derived from the Core Registry (V2.0).
In the high-resolution CENTER-TBI substudy, high-frequency digital signals of vital parameters were recorded during the ICU stay. Arterial blood pressure (ABP) was most often measured through either radial or femoral arterial lines. ICP was obtained using an intraparenchymal probe (Codman ICP MicroSensor; Codman & Shurtleff, Inc., Raynham, MA), parenchymal fiberoptic pressure sensor (Camino ICP Monitor; Integra Life Sciences, Plainsboro, NJ) or, rarely, external ventricular drain. Signal processing was done using the ICM+ software (Cambridge Enterprise Ltd., Cambridge, United Kingdom).
Signal artifacts were removed partially through visual inspection and also using automated algorithmic methods. For ABP (0–300 mmHg) and ICP (0–100 mmHg) a primary filter was used. ABP data were removed if the pulsatility of ABP (ABPmax-ABPmin) within 1.5 seconds was <20 or >200 mmHg. HR was calculated with use of the fundamental frequency function within 10 seconds on the ABP signal (using the Fourier fast transformation) with a lower and upper limit of 40/min and 180/min. PbtO2 levels >60 or <0 mmHg and temperature levels >45
High-frequency data (MAP; HR; fraction of inspired oxygen, FiO2; temperature; ICP; CPP; PbtO2; ORx; PRx) were averaged over 10 minutes.
Brain tissue hypoxia was defined as PbtO2 <20 mmHg, since this is the threshold prompting interventions according to current practices (Le Roux et al., 2014).
Fever definitions
Temperature was either measured intracranially (N = 16, 49%), external-axillary (N = 2, 6%), by a bladder (N = 11, 33%), or tympanic temperature sensor (N = 2, 6%). In two patients (6%), temperature was derived from a mixed source. Fever was defined as temperature levels above 38.3
Data analysis
There was no significant difference in temperature in the subset of patients with PbtO2 probes compared with all patients with temperature data, both following similar distributions. To minimize bias from a few longer monitoring sessions, periods of duration greater than 11 days were cropped at 11 days for the purpose of analysis. A clinically relevant episode of temperature increase (effervescence) was defined as an increase by
The values were automatically processed for sets of given parameters. For imputation, the function “last observation carry forward” was used from the zoo package. This function replaces each missing value with the most recent nonmissing value before it (Zeileis and Grothendieck, 2005). Imputations were made in (1) 9/71 episodes of
Statistics
Statistical analysis of anonymized patient data was performed by L.H. who was not involved in data collection and who was blinded to the clinical course of all patients. For creation of the summary tables of each episode, the summary tools package was used (Dominic Comtois, 2019; summarytools: Tools to Quickly and Neatly Summarize Data, R package version 0.9.4).
PbtO2 changes (ΔPbtO2), as well as changes of other vital and neuromonitoring parameters within temperature increases were tested in univariate analysis using generalized estimated equations with an autoregressive matrix to account for repeated measurements. Vital or neuromonitoring parameters at baseline or highest temperature points were compared across different PbtO2 characteristics using the t-test or Mann–Whitney U Test, as appropriate.
The analysis and visualizations were conducted using R version 3.6.0 (2019-04-26) and SPSS (version 24.0; IBM SPSS Statistics, Armonk, NY). The analysis was conducted under the consolidation of RMarkdown notebooks, which allowed the analysis code and representation in one document. RMarkdown allows a notebook interface to the analysis, which was especially useful with regard to changes of the data, layout refinement, plots, and discussion of the authors. Statistical significance was attributed to a p-value <0.05.
Results
Of 102 patients prospectively included in the high-resolution ICU cohort, 33 patients met the inclusion criteria for the current analysis. Baseline characteristics were not different between the study population and excluded patients (age p = 0.202, sex p = 1.000, GCS at baseline p = 0.114, GCS motor at baseline p = 0.377). Detailed information on baseline characteristics, hospital complications, and outcomes of 33 patients is given in Table 1. In total, 3587 neuromonitoring hours (median per patient 86; interquartile range [IQR] 61–159 hours) with simultaneous PbtO2 and temperature measurements during the first 11 days of ICU stay were analyzed. Episodes of fever within the study time occurred in most patients (26/33, 79%) and were observed during 13% of monitoring time (471 hours). During episodes of fever, brain tissue hypoxia (PbtO2 <20 mmHg) was found in 20% of measurements, which was comparable to the overall incidence of brain tissue hypoxia (25%) over the whole study period. Mean PbtO2 values were significantly higher at higher temperature levels (Kruskal–Wallis: p < 0.001) (Fig. 1). In this line, there was a weak-positive correlation between higher temperature and higher PbtO2 levels (rho = 0.11; p < 0.01).

Mean PbtO2 values were significantly higher at higher temperature levels (p < 0.001). PbtO2, brain tissue oxygen tension.
Demographics of 33 Patients
ASA, American Society of Anesthesiologists; CT, computed tomography; GCS, Glasgow Coma Scale; GOSE, Extended Glasgow Outcome Scale; ICU, intensive care unit; IQR, interquartile range.
Changes in PbtO2 and hemodynamic variables during temperature increases
Two hundred two episodes of clinically significant temperature increases (
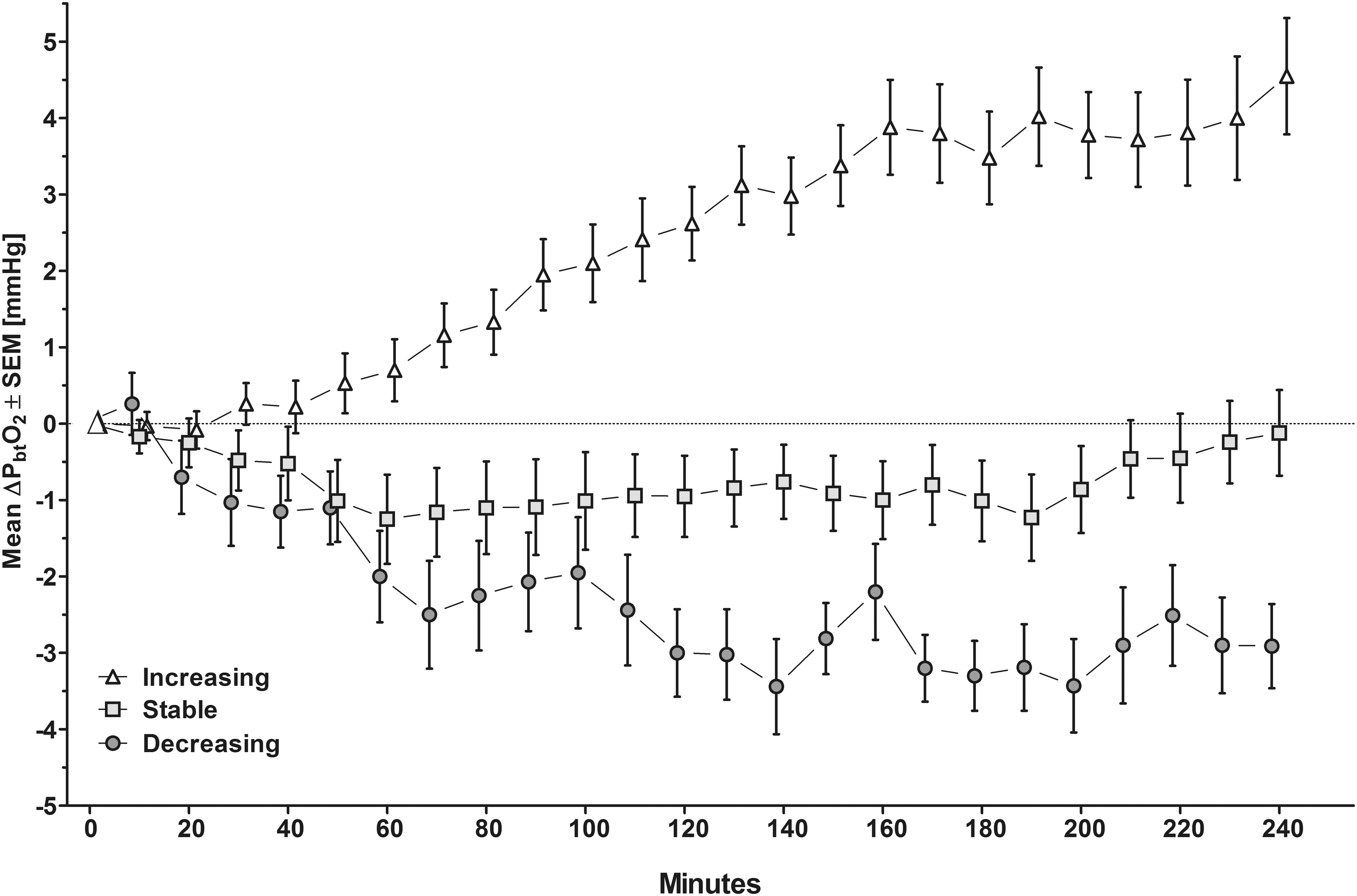
Displays different mean PbtO2 changes during 202 episodes of temperature increases. PbtO2, brain tissue oxygen tension. SEM, standard error of the mean.
Changes in Brain Tissue Oxygen Tension and Hemodynamic Variables During Temperature Increases Splitting at Different Patterns of Brain Tissue Oxygen Tension Changes
Hemodynamic and neuromonitoring parameters are expressed as mean ± standard deviation at baseline and highest temperature within each episode of temperature increase. Using generalized estimating equations, the significance of changes of each variable (Δ) within temperature increases was tested in univariate analysis. Significant changes (p < 0.05) are bold.
bl, baseline; CI, confidence interval; CPP, cerebral perfusion pressure; HR, heart rate; ICP, intracerebral pressure; MAP, mean arterial pressure; OR, odds ratio; ORx, oxygen reactivity index; PbtO2, brain tissue oxygen tension; PRx, pressure reactivity index; T, temperature.
Descriptive analysis of important covariates reflecting the hemodynamic situation and autoregulatory state during temperature increases demonstrated an increase in HR (p < 0.001), irrespective of PbtO2 characteristics. During temperature increases with drops in PbtO2, a decrease in CPP was more pronounced as compared with episodes when PbtO2 increased. During CPP decreases, drops in MAP (p < 0.001), but not increases in ICP (p = 0.565), were observed. Details are given in Table 2.
The autoregulatory status as assessed with the PRx was not different at baseline (p = 0.564) or peak temperature (p = 0.826) comparing episodes when PbtO2 decreased or increased and PRx did not change during effervescences (Table 2). In this line, the percentage of impaired autoregulation (PRx
Brain tissue hypoxia at baseline of effervescence was evident in 19% of episodes (38/202). When analyzing only these episodes, overall PbtO2 improved (ΔPbtO2 +5.0 ± 7.2 mmHg, p < 0.001). PbtO2 increased in 47%, did not change in 45%, and decreased in 8% of these episodes. CPPbaseline (p < 0.001) and CPPpeak (p = 0.001) levels were lower as compared with temperature increases with normal PbtO2 levels at baseline (Table 3).
Changes in Brain Tissue Oxygen Tension and Hemodynamic Variables During Temperature Increases Splitting at Brain Tissue Oxygen Tension <20 mmHg and Brain Tissue Oxygen Tension ≥20 mmHg at Baseline
Hemodynamic and neuromonitoring parameters are expressed as mean ± standard deviation at baseline and highest temperature within each episode of temperature increase. Using generalized estimating equations, the significance of changes of each variables (Δ) within temperature increases was tested in univariate analysis. Significant changes (p < 0.05) are bold.
bl, baseline; CI, confidence interval; CPP, cerebral perfusion pressure; HR, heart rate; ICP, intracerebral pressure; MAP, mean arterial pressure; OR, odds ratio; ORx, oxygen reactivity index; PbtO2, brain tissue oxygen tension; PRx, pressure reactivity index; T, temperature.
Splitting temperature increases by baseline temperature (<37.5
Changes in Brain Tissue Oxygen Tension and Hemodynamic Variables During Temperature Increases Splitting at Temperature <37.5°C and Temperature ≥37.5°C at Baseline
Hemodynamic and neuromonitoring parameters are expressed as mean ± standard deviation at baseline and highest temperature within each episode of temperature increase. Using generalized estimating equations, the significance of changes of each variables (Δ) within temperature increases was tested in univariate analysis. Significant changes (p < 0.05) are bold.
bl, baseline; CI, confidence interval; CPP, cerebral perfusion pressure; HR, heart rate; ICP, intracerebral pressure; MAP, mean arterial pressure; OR, odds ratio; ORx, oxygen reactivity index; PbtO2, brain tissue oxygen tension; PRx, pressure reactivity index; T, temperature.
Manually versus parametric detection of temperature increases
Assisted episode detection of temperature increases revealed (1) 71 (total increase of
Discussion
The main finding of the current study is that variable changes in PbtO2 can be observed when temperature increases in severe TBI patients. PbtO2 increased on average in every third episode and decreased in every sixth episode. Importantly, a drop in PbtO2 occurred simultaneously to a decrease in CPP in the context of a decrease in MAP. Although more episodes of temperature increases were identified by visual curve inspection, algorithm-supported detection was feasible and revealed similar hemodynamic changes.
In the overall cohort, we found a weak-positive correlation between absolute temperature and PbtO2 levels, which is consistent with previous reports (Spiotta et al., 2008; Nyholm et al., 2017). To the best of our knowledge, this is the first study analyzing time-coded dynamic systemic changes and brain oxygenation during episodes of temperature increases at different baseline temperature levels. Our study suggests that alterations of temperature may negatively affect brain hemodynamics only in a minority of analyzed episodes. In a recent prospective observational study in TBI patients, brain temperature variations (>1
In our cohort, the overall impact of temperature changes on brain tissue oxygen tension was minute. During most effervescence episodes, PbtO2 increased or remained stable, which is in line with previous data (Stocchetti et al., 2005). This observation was independent of baseline temperature and baseline PbtO2. It is important to keep in mind that the measured PbtO2 levels reflect the balance between oxygen delivery, consumption, tissue diffusion, and extraction (Rosenthal et al., 2008). Therefore, the shift of the oxygen dissociation curve in hyperthermic conditions with a higher oxygen extraction may serve as one explanation for the observed overall increase of PbtO2 during effervescence (Siggaard-Andersen et al., 1984). Moreover, normal or even increasing PbtO2 levels during temperature increases in our study suggest that the extended metabolic demand was met by upregulated energy supply (Rossi et al., 2001; Stocchetti et al., 2005). This is important and may separate pathophysiological changes observed during effervescences in TBI patients from other stroke patients, where fever exacerbates ischemic injury (Busto et al., 1987). In case of metabolic coupling, regional cerebral blood flow (CBF) increases in parallel to PbtO2 through vasodilation (Jaeger et al., 2005), which bears the risk of raised ICP (Stocchetti et al., 2005). In our patients, ICP was well controlled and changes in ICP (ΔICP 0.6 mmHg) were negligible, irrespective of the baseline autoregulatory status as expressed by PRx (data not shown). Other cardiovascular effects of temperature increases include a higher cardiac output, which may augment oxygen delivery (Bain et al., 2014; Walter et al., 2016). Another explanation, why PbtO2 increased in most of episodes is that cerebral autoregulation was preserved during the majority of episodes.
In a smaller proportion of episodes, we observed drops in PbtO2 levels. This is of interest as previous studies report on the overall effect of temperature increases on PbtO2 and did not include the longitudinal information of PbtO2 patterns (Stocchetti et al., 2005). The most likely explanation for PbtO2 drops is the observed decrease in CPP secondary to a decrease in MAP. It is well known that hypotension may occur during fever as a consequence of vasodilation and redistribution of blood (Bain et al., 2014; Walter et al., 2016). It is important to mention that most of the centers applied a PbtO2-guided treatment concept aiming at the prevention of brain tissue hypoxia. Although, mean baseline PbtO2 was mostly above 20 mmHg, new brain tissue hypoxia was commonly observed during episodes when PbtO2 decreased (30%). In the overall cohort, brain tissue hypoxia developed on average in every sixth episode and persisted in every tenth episode reflecting a considerable risk of secondary brain injury during effervescences. We may have underestimated the incidence of brain tissue hypoxia in our cohort, based on the assumption that low PbtO2 was treated in most centers. In the current understanding, continuous monitoring of PbtO2, CPP, and blood pressure may help to minimize the risk of brain tissue hypoxia. Although a hyperventilatory response to pyrexia is common and may lead to a reduction in CBF and PbtO2 by respiratory alkalosis (Bain et al., 2014), this well-established effect may be negligible in this patient population, where a controlled mechanical ventilation was applied.
Notably, different patterns of PbtO2 changes were observed in the same patient, suggesting that the association between temperature increases and PbtO2 may depend on many factors, including the phase of disease, baseline vasopressor need, and the status of cerebral autoregulation.
In the current study, we aimed to identify increases in temperature by manual and algorithm-supported detection. Interestingly, we could identify more episodes through visual plot analysis because of the basic and strict regulations of the parametric method. To align the method to the “softer” human detection, a better preprocessing and methods with a less rigid rule set may help in the identification. Still, a software-based detection of effervescence is feasible, and the results of associated brain and systemic hemodynamic changes were similar. Moreover, advanced multivariable time-series methods could allow better identification of episodes. Future studies are needed to investigate whether a software-based method could be used at the patients' bedside to alarm the clinician even before a substantial temperature increase is reached. Such predictive models were feasible for predicting changes in ICP and PbtO2 (Myers et al., 2016).
Limitations
Several limitations deserve consideration. We did not assess CBF and brain metabolic changes associated with effervescence, which leaves some interpretation of our results speculative. Second, time-coded vasopressor use was not recorded in our patients, which may have influenced the observed hemodynamic changes. Third, a PbtO2-guided therapy targeting at normal PbtO2 levels was applied in several centers, which makes our results not transferrable to centers without oxygen monitoring and without a comparable treatment approach. Still, the risk of brain tissue hypoxia may be likely higher without monitoring. Fourth, to avoid a bias of hemodynamic side effects of pharmacologic fever treatment, we did not include episodes of temperature decreases in our study. Moreover, fever management varies between European centers (Picetti et al., 2019) and may have made the interpretation of decreases in temperature challenging. Fifth, probe location of PbtO2 catheters was not integrated in the current analysis. Since we investigated relative changes, probe location might not be of high importance. Moreover, the observation that different PbtO2 patterns during temperature increase occurred within the same patients might further justify our approach. Sixth, the site to measure temperature differed among patients. It is well known that intracranial temperature may exceed body temperature by several degree Celsius in acute brain injury highlighting the difficulty of fever definition (McIlvoy, 2004). Since our analysis focused on temperature increases irrespective of fever, this definition was of minor importance. Next, a considerable number of patients with neuromonitoring had no simultaneous recordings of temperature and PbtO2 and had to be excluded, which constitutes the risk of a selection bias. However, baseline characteristics and temperature levels did not differ among the groups. Last, following the Gay-Lussac's Law, the pressure of oxygen rises in parallel with the temperature increases. This phenomenon could have influenced our results, as we are not aware in which patients combined PbtO2/temperature probes with automatic correction of PbtO2 for patients' temperatures were used or whether temperature levels were manually entered in the remaining patients.
Conclusion
In summary, our study indicates that adequate brain tissue oxygen tension was preserved during most episodes of effervescences in patients with severe TBI. However, there was a considerable risk of brain tissue hypoxia during effervescences. On average in every sixth episode a decrease of brain tissue oxygen tension was observed simultaneous to a decrease in CPP, which supports the idea of continuous (neuro)monitoring in severe TBI patients.
Animal or Human Experimentation
The CENTER-TBI study (EC grant 602150) has been conducted in accordance with all relevant laws of the EU if directly applicable or of direct effect and all relevant laws of the country, where the recruiting sites were located, including but not limited to, the relevant privacy and data protection laws and regulations (the “Privacy Law”), the relevant laws and regulations on the use of human materials, and all relevant guidance relating to clinical studies from time to time in force including, but not limited to, the ICH Harmonized Tripartite Guideline for Good Clinical Practice (CPMP/ICH/135/95; “ICH GCP”) and the World Medical Association Declaration of Helsinki entitled “Ethical Principles for Medical Research Involving Human Subjects.” Informed Consent by the patients and/or the legal representative/next of kin was obtained, accordingly to the local legislations, for all patients recruited in the Core Dataset of CENTER-TBI and documented in the e-CRF. Ethics approval was obtained for each recruiting site. The list of sites, Ethics Committees, approval numbers, and approval dates can be found on the website.
Footnotes
Acknowledgments
CENTER-TBI High-Resolution Substudy Participants and Investigators: Audny Anke: Department of Physical Medicine and Rehabilitation, University Hospital Northern Norway, Tromsø, Norway; Bo-Michael Bellander: Department of Neurosurgery & Anesthesia & intensive care medicine, Karolinska University Hospital, Stockholm, Sweden; Erta Beqiri: NeuroIntensive Care, Niguarda Hospital, Milan, Italy; Andras Buki: Department of Neurosurgery, Medical School, University of Pécs, Hungary and Neurotrauma Research Group, János Szentágothai Research Center, University of Pécs, Hungary; Manuel Cabeleira: Brain Physics Laboratory, Division of Neurosurgery, Department of Clinical Neurosciences, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Marco Carbonara: Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Arturo Chieregato: NeuroIntensive Care, Niguarda Hospital, Milan, Italy; Giuseppe Citerio: NeuroIntensive Care Unit, Department of Anesthesia & Intensive Care, ASST di Monza, Monza, Italy; School of Medicine and Surgery, Università Milano Bicocca, Milano, Italy; Hans Clusmann: Department of Neurosurgery, Medical Faculty RWTH Aachen University, Aachen, Germany; Endre Czeiter: Department of Neurosurgery, University of Pecs and MTA-PTE Clinical Neuroscience MR Research Group and Janos Szentagothai Research Center, University of Pecs, Hungarian Brain Research Program (Grant No. KTIA 13 NAP-A-II/8), Pecs, Hungary; Marek Czosnyka: Brain Physics Laboratory, Division of Neurosurgery, Department of Clinical Neurosciences, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Bart Depreitere: Department of Neurosurgery, University Hospitals Leuven, Leuven, Belgium; Ari Ercole: Division of Anesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Shirin Frisvold: Department of Anesthesiology and Intensive Care, University Hospital Northern Norway, Tromso, Norway; Stefan Jankowski: Neurointensive Care, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom; Danile Kondziella: Departments of Neurology, Clinical Neurophysiology and Neuroanesthesiology, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark; Lars-Owe Koskinen: Department of Clinical Neuroscience, Neurosurgery, Umeå University, Umeå, Sweden; Ana Kowark: Department of Anesthesiology, University Hospital of Aachen, Aachen, Germany; David K. Menon: Division of Anesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Geert Meyfroidt: Intensive Care Medicine, University Hospitals Leuven, Leuven, Belgium; Kirsten Moeller: Department Neuroanesthesiology, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark; David Nelson: Department of Neurosurgery & Anesthesia & Intensive Care Medicine, Karolinska University Hospital, Stockholm, Sweden; Anna Piippo-Karjalainen: Helsinki University Central Hospital, Helsinki, Finland; Andreea Radoi: Department of Neurosurgery, Vall d'Hebron University Hospital, Barcelona, Spain; Arminas Ragauskas: Department of Neurosurgery, Kaunas University of Technology and Vilnius University, Vilnius, Lithuania; Rahul Raj: Helsinki University Central Hospital, Helsinki, Finland; Jonathan Rhodes: Department of Anesthesia, Critical Care & Pain Medicine NHS Lothian & University of Edinburg, Edinburgh, United Kingdom; Saulius Rocka: Department of Neurosurgery, Kaunas University of Technology and Vilnius University, Vilnius, Lithuania; Rolf Rossaint: Department of Anesthesiology, University Hospital of Aachen, Aachen, Germany; Juan Sahuquillo: Department of Neurosurgery, Vall d'Hebron University Hospital, Barcelona, Spain; Oliver Sakowitz: Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany; Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany; Nina Sundström: Department of Radiation Sciences, Biomedical Engineering, Umea University, Umea, Sweden; Riikka Takala: Perioperative Services, Intensive Care Medicine, and Pain Management, Turku University Central Hospital and University of Turku, Turku, Finland; Tomas Tamosuitis: Neurointensive Care Unit, Kaunas University of Health Sciences, Kaunas, Lithuania; Olli Tenovuo: Rehabilitation and Brain Trauma, Turku University Central Hospital and University of Turku, Turku, Finland; Peter Vajkoczy: Neurologie, Neurochirurgie und Psychiatrie, Charité—Universitätsmedizin Berlin, Berlin, Germany; Alessia Vargiolu: Neurointensive Care Unit, Department of Anesthesia & Intensive Care, ASST di Monza, Monza, Italy; Rimantas Vilcinis: Department of Neurosurgery, Kaunas University of Health Sciences, Kaunas, Lithuania; Stefan Wolf: Department of Neurosurgery, Charité—Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany; Alexander Younsi: Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany; Frederick A. Zeiler: Division of Anesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Section of Neurosurgery, Department of Surgery, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, Canada.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Data used in preparation of this article were obtained in the context of CENTER-TBI, a large collaborative project with the support of the European Union 7th Framework program (EC grant 602150). Additional funding was obtained from the Hannelore Kohl Stiftung (Germany), from OneMind (United States), and from Integra LifeSciences Corporation (United States).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.