
Abstract
Emergent modification of a patient's body temperature is crucial in certain disease or injury states. Advanced targeted temperature management techniques such as central venous catheter devices are not universally available, however, virtually all medical centers have access to intravenous fluids. This study approximates the change in body temperature for a given volume of room temperature, chilled, or heated isotonic crystalloid bolus. Using thermodynamic principles, a mathematical model was created to approximate change in body core temperature in response to a given volume and temperature of intravenous fluid. The model assumes rapid fluid infusion and the previously published specific heat capacity of the human body of 3.47 J/kg · °C. Values were calculated under conditions of varying body temperatures from profound hypothermia to hyperthermia (18°C–45°C). Various crystalloid temperatures representing iced, room temperature, and warmed (4°C, 20°C, 42°C) were used in the calculations. Each 30 mL/kg dose of 20°C crystalloid is expected to cool a hyperthermic (38°C–45°C) patient by 0.6°C–0.9°C. Each 30 mL/kg dose of 4°C crystalloid is expected to cool a hyperthermic (38°C–45°C) patient by 1.2°C–1.4°C. Each dose of 42°C crystalloid is expected to warm a hypothermic patient by 0.2°C–0.8°C. Using the results in this study, clinicians may roughly estimate the effect of temperature management with varying doses of intravenous fluids and thus assess the benefits of this technique. Risk should be evaluated based on inevitable coadministered volume and electrolytes. Individuals with volume-sensitive conditions such as heart, liver, or kidney failure deserve particular attention. Based on a mathematical model, typical expected core temperature change is about 0.2°C–1.4°C per 30 mL/kg crystalloid bolus, depending on patient and fluid temperature.
Introduction
Emergent modification of a patient's body temperature is crucial in certain disease and injury states to ensure survival or decrease morbidity. Conditions such as heat stroke, sympathomimetic toxicity, and malignant hyperthermia can kill within minutes without rapid cooling. Similarly, patients suffering from environmental hypothermia, myxedema coma, or sepsis may require fast heating to restore hemodynamics and improve prognosis. In addition, evidence suggests the benefits of inducing abnormal temperature in cases such as postcardiac arrest care (Lascarrou et al., 2019). Drug-induced changes in sensorium may inhibit self-protective behavior from environmental dangers, and toxicological fatalities are strongly correlated with ambient temperature (Marzuk et al., 1998; Bohnert et al., 2010).
A patient's body core temperature is controlled by the hypothalamus with a normal set point of 37°C ± 0.5°C. Counterregulatory responses to elevated temperature include sweating, peripheral vasodilation, and muscle relaxation (Osilla et al., 2019). Counterregulatory responses to depressed temperature include shivering and peripheral vasoconstriction (Osilla et al., 2019). Hyperthermic and hypothermic syndromes overwhelm or inhibit the body's thermoregulatory mechanisms leading to enzyme dysfunction, loss of thermoregulatory function, hemodynamic collapse, and death (Truhlář et al., 2015).
Hypothermia is generally categorized into five stages: mild (32°C–35°C), moderate (28°C–32°C), severe (24°C–28°C), profound (<24°C), and irreversible (dead) (Truhlář et al., 2015). Any elevation of core temperature above 37.5°C is hyperthermic, however, temperatures in excess of 40.5°C should be considered immediately life-threatening in the setting of altered mental status or organ dysfunction (Epstein and Yanovich, 2019).
Multiple methods for body temperature modification exist such as ice packs, central venous countercurrent devices, forced-air warming blankets, evaporative cooling, cold water immersion, peritoneal lavage, and extracorporeal membrane oxygenation (Hilmo et al., 2014; Kempainen and Brunette, 2004; Truhlář et al., 2015; Dow et al., 2019; Epstein and Yanovich, 2019). A temperature modification technique available at nearly all emergency and inpatient settings is intravenous fluid bolus of lactated Ringers solution or physiological saline. Guidelines for resuscitating hypothermic or hyperthermic patients include heated or cooled intravenous fluids, and warmed (40°C–42°C) intravenous fluids are an evidence grade 1B recommendation for hypothermic resuscitation (Truhlář et al., 2015; Dow et al., 2019). This study seeks to approximate the change in body temperature for a given volume of chilled or heated isotonic crystalloid bolus; utilizing this information, clinicians may estimate the dose–response of fluids for treatment of abnormal body temperature.
The thermodynamic principle of enthalpy explains heat transfer between substances, such as a crystalloid infusion and the human body. Temperature change is based on the mass, temperature difference, and specific heats of both body and fluid. Specific heat is defined as the quantity of energy required to raise the temperature of the unit mass of a given substance by a given amount. For example, when equal volumes of boiling water are poured into otherwise identical iron and clay pots, the iron pot will develop a higher maximum temperature.
Methods
Non-human trial; no IRB approval was needed. Using thermodynamic principles, the author created a mathematical model to approximate change in body temperature in response to a given volume and temperature of crystalloid infusion. Manipulation of the formulae yielded functions that solve for temperature change per liter bolus, and temperature change per 30 mL/kg bolus. The two formulae are given below (see Fig. 1 for derivation):
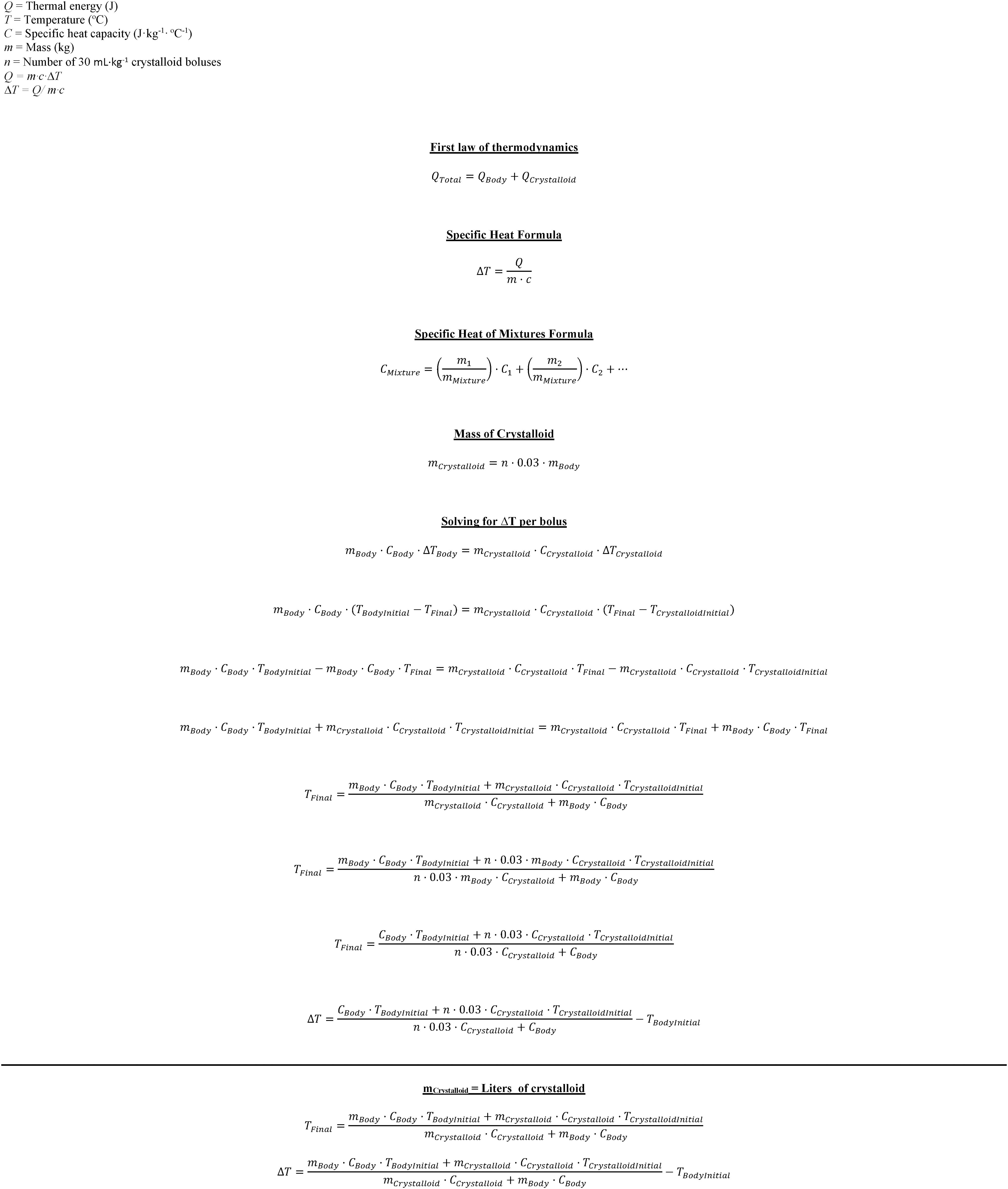
Derivation of formulae used in a heat exchange model.
Change in temperature (ΔT) per mL/kg bolus (n)
Change in temperature (ΔT) per 1 L bolus
Where m is mass, C is specific heat, T is temperature, and n is number of 30 mL/kg crystalloid boluses. Patient mass is measured weight, crystalloid mass is approximated as one kilogram per liter due to near-identical specific gravity to water, and crystalloid specific heat is approximated as that of water. Temperature is measured core patient temperature, and temperature of crystalloid is selected. The previously published specific heat capacity of the human body of 3.47 J/kg · °C was used for calculations (Kakitsuba and Mekjavic, 1987). This value is within 6% of the specific heats of tissues most relevant to temperature-related mortality, that is, heart (3.686 J/kg · °C) and brain (3.630 J/kg · °C) (Hasgall et al., 2018). The previously published value is within 4% of an estimate by a weighted average of the specific heat of component tissues (3.35 J/kg · °C) as delineated in version 4.0 of the IT'IS Database for thermal parameters of biological tissues (Hasgall et al., 2018). The calculated specific heat is based on a human body composed by mass of 63% water, 15% fat, 4% cortical bone, 1% cancellous bone, and 17% protein (Report of the Task Force, 1979; Jacobshagen et al., 2009; National Academies Press, 2015; Lacroix, 2019).
Values were calculated under conditions of varying patient body temperatures ranging from profound hypothermia to hyperthermia (18°C–45°C) using Microsoft Excel (2019). Various crystalloid temperatures representing iced, room temperature, and warmed (4°C, 20°C, 42°C), and various crystalloid volumes (number of liters, number of 30 mL/kg boluses) were used in the calculations. Fluid temperatures were based on those that are readily achievable as well as published guidelines (Jacobshagen et al., 2009; Truhlář et al., 2015). The formulae were also used to estimate dosing requirements for various patient-based scenarios. Induced hypothermia was simulated by calculating fluid dose required to lower core temperature from 37°C to 33°C. Morbid obesity was simulated by estimating the specific heat (3.054 J/kg · °C) of a 150 kg patient who is 40% body fat. Profound malnutrition was simulated by estimating the heat capacity (3.466 J/kg · °C) of a patient who is 5% body fat, which is within 1% of the previously published value (Hasgall et al., 2018). Profound peripheral vasoconstriction was simulated by subtracting the published estimated percentage weight of arms (5.37%) and legs (17.56%) from the body mass (Plagenhoef et al., 1983). Unintentional iatrogenic hypothermia was simulated by providing a large volume crystalloid and blood resuscitation to a normothermic patient. Massive blood transfusion (10 U or 5 L) was modeled using specific heat of blood of 3.617 J/kg · °C (Hasgall et al., 2018).
Results
Calculations were performed using the maximum number of significant digits available for each value. Uncertainty is expressed by presenting results using two significant digits.
Table 1 represents varying temperature crystalloid infusions based on a 30 mL/kg crystalloid dosing strategy. Each cell denotes the change in temperature from a single 30 mL/kg dose. Each 30 mL/kg dose of 20°C crystalloid is expected to cool a hyperthermic (38°C–45°C) patient by 0.6°C–0.9°C. Each 30 mL/kg dose of 4°C crystalloid is expected to cool a hyperthermic (38°C–45°C) patient by 1.2°C–1.4°C. Each dose of 42°C crystalloid is expected to warm a mildly hypothermic (32°C–35°C) patient by 0.2°C–0.3°C, a moderately hypothermic (28°C–32°C) patient by 0.3°C–0.5°C, a severely hypothermic (24°C–28°C) patient by 0.5°C–0.6°C, and a profoundly hypothermic (18°C–24°C) patient by 0.6°C–0.8°C.
Expected Temperature Change Per 30 mL/kg Crystalloid Bolus
Tables 2–4 represent varying temperature crystalloid infusions in a 70 kg patient based on the number of liters given. Each cell denotes the final temperature after a single 1 L dose. Each liter of room temperature (20°C) crystalloid would be expected to reduce a hyperthermic patient's temperature by 0.4°C–0.7°C. Each liter dose of iced (4°C) crystalloid would be expected to reduce a hyperthermic patient's temperature by 0.4°C–0.7°C. Each liter dose of 42°C crystalloid is expected to warm a mildly hypothermic (32°C–35°C) patient by 0.1°C–0.2°C, a moderately hypothermic (28°C–32°C) patient by 0.2°C, a severely hypothermic (24°C–28°C) patient by 0.2°C–0.3°C, and a profoundly hypothermic (18°C–24°C) patient by 0.3°C–0.4°C.
Expected Final Temperature Per 4°C Liter in a Seventy Kilogram Patient
Expected Final Temperature Per 20°C Liter in a Seventy Kilogram Patient
Expected Final Temperature Per 42°C Liter in a Seventy Kilogram Patient
Expected temperature change was modeled in various patient scenarios.
Therapeutic hypothermia
To lower the temperature from 37°C to 33°C, a patient would require 3.8 iced (4°C) 30 mL/kg crystalloid boluses, which translates to 8 L in a 70 kg patient. Using room-temperature (20°C) crystalloid, this would require 18 L in a 70 kg patient.
Morbid obesity (150 kg)
Each liter dose of room temperature (20°C) crystalloid would decrease a hyperthermic patient's temperature by 0.1°C–0.2°C. Each liter dose of iced (4°C) crystalloid would decrease a hyperthermic patient's temperature by 0.2°C–0.3°C. Each liter dose of 42°C crystalloid is expected to warm a patient by ≤0.1°C through all stages of hypothermia.
Malnutrition
Results from Table 1 are applicable to malnutrition.
Profound peripheral vasoconstriction
In a 70 kg patient, each liter of room temperature (20°C) crystalloid would be expected to reduce a hyperthermic patient's temperature by 0.3°C–0.5°C. Each liter dose of iced (4°C) crystalloid would be expected to reduce a hyperthermic patient's temperature by 0.6°C–0.9°C. Each liter dose of 42°C crystalloid is expected to warm a mildly hypothermic (32°C–35°C) patient by 0.1°C–0.2°C, a moderately hypothermic (28°C–32°C) patient by 0.2°C–0.3°C, a severely hypothermic (24°C–28°C) patient by 0.3°C–0.4°C, and a profoundly hypothermic (18°C–24°C) patient by 0.3°C–0.5°C.
Unintentional iatrogenic hypothermia from room temperature crystalloid infusion
In a 70 kg patient, each liter is expected to lower the temperature by 0.2°C–0.3°C. A 6 L bolus is expected to decrease body temperature from 37°C to 35.4°C.
Unintentional iatrogenic hypothermia from blood transfusion
In a 70 kg patient, each respective unit of refrigerated (4°C) and room temperature (20°C) unit of blood is expected to lower the temperature by 0.2°C and 0.1°C. A respective 4°C and 20°C rapid 10 U (5 L) blood transfusion is expected to decrease body temperature from 37°C to 34.7°C and 35.8°C.
Discussion
This article seeks to provide dosing information for temperature management across a range of intravenous fluid doses and temperatures using thermodynamic equations. A controlled human trial assessing these results is unlikely because inducing dangerous temperature change in healthy subjects is unethical, and prospectively gathering patient data is subject to confounding by other temperature modifying therapies. Limited clinical studies have examined the effect of cold fluid infusion to lower core temperature. A retrospective study of 52 cardiac arrest survivors found that infusion of 3800 ± 275 mL iced saline over about 4 hours brought core temperature from 35.3 ± 0.2 to 33°C, however, weights were not recorded (Jacobshagen et al., 2009). A study examining fever control via cold saline infusion in 12 patients with acute brain injury found the mean fluid volume needed to reduce core temperature by 1°C at near-physiological temperature was 18.7 mL/kg (Willms et al., 2019). A study of nine volunteers under general anesthesia found that a 30-minute 40 mL/kg infusion of 4°C saline cooled the subjects by 2.5 ± 0.4°C (Rajek et al., 2000). Another study examined eight healthy male volunteers and found that it required about 23 mL/kg of 4°C saline to lower core temperature by 1°C (Rittenberger et al., 2019). A retrospective study of 18 pediatric intensive care unit patients found that 4°C saline decreased temperature from 38.2°C ± 1.6°C to 37.0°C ± 1.7°C per 18.2 ± 10.1 mL/kg infusion (Fink et al., 2012). Although these studies only examined patients with initial temperatures ranging from normal to 39.5°C, the formula-predicted temperature reduction at 39°C is similar at 1.2°C per 30 mL/kg bolus of 4°C saline. All of these studies examined patients or research subjects with normal or near-normal initial and final core temperatures. The clinical studies were confounded by antipyretics, sedatives, paralytics, and other temperature management strategies, as well as being retrospectively designed. The volunteer studies examined physiological rather than disease states, were limited by narrow temperature modification range, and were confounded by anesthetics. Ultimately, a controlled clinical trial would be needed to validate the mathematical model's expected effect from temperature-modified intravenous fluids.
Ideally, heat administration is titrated with continuous core temperature measurement via an esophageal thermometer, however, this method may be unavailable or contraindicated. Using the results in this study, clinicians may roughly estimate the effect of temperature management with varying doses of intravenous fluids and thus assess the benefits of this technique. Risk should be evaluated based on inevitable coadministered volume and electrolytes. Individuals with volume-sensitive conditions such as heart, liver, or kidney failure deserve particular attention.
The dose–response relationship described herein may imply situations where warmed or cooled fluids offer insubstantial therapeutic effect. For example, potentially dangerous volumes of warm fluid are required to make a clinically significant temperature difference in mildly or moderately hypothermic patients, or as solitary therapy for induced hypothermia. In other cases, hypothermic patients may require large fluid volumes due to cold diuresis, and so, the coadministration of intravenous heat and volume may be beneficial. The temperature change from warm intravenous fluids on morbidly obese patients appears minimal. During profound hypothermia, shock states, and vasopressor infusion, there may be relative vasoconstriction of the extremities, which was modeled in this study (Dow et al., 2019). Although large-volume iced fluid infusions have been reported without adverse effects, extreme caution should be maintained since sudden cardiac temperature change may result in dysrhythmia (Jacobshagen et al., 2009).
Patients who require large-volume resuscitations such as in the setting of exsanguinating hemorrhage, pancreatitis, and diabetic ketoacidosis may develop unintended hypothermia due to infusion of cool fluids. Typically, blood products are refrigerated and crystalloids stored at room temperature. Fluid warming should be considered if the patient is unlikely to tolerate the expected temperature change.
Limitations
This study has several limitations. All estimates of change in body temperature are based on mathematical models rather than clinical evidence. A randomized-controlled trial would be a more definitive method of approximating heat dose from intravenous fluids. The model does not perfectly account for differentially perfused core and periphery, mismatch between body heat generation and dissipation, heat exchange between fluid and environment during infusion, variations in average specific heat between patients, shivering and sweating, variation in organ perfusion, or change in body heat generation over the course of a resuscitation. The model does not account for preferential heat exchange with a single extremity via peripheral intravenous catheter versus central venous catheter. This study assumes core temperature measured via an esophageal probe adjacent to the heart's left atrium, however, temperature may be measured elsewhere in practice; also, core temperature may not reflect brain temperature. The model assumes rapid fluid administration such as with a pressure infuser. In practice, the effect of temperature-controlled intravenous fluids may be confounded by additional simultaneous measures to correct body temperature such as external or invasive warming or cooling.
Conclusion
Clinicians should consider the relationship between intravenous fluid dose and temperature change on the human body. Based on a mathematical model, typical expected core temperature change is about 0.3°C–1.4°C per 30 mL/kg crystalloid bolus, depending on patient and fluid temperature. A risk–benefit assessment should be made across dose ranges for intravenous fluids to reflect the continuum of expected clinical effects, and account for other methods of temperature management.
Author Contributions
Dr. A.B. is the sole author and conceptualized, researched, wrote, and edited the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.