
Abstract
Gout arthritis commonly affects joint regions by deposition of crystals, promoting functional damage mainly during periods of exacerbation. Cryotherapy is a commonly used resource to contain inflammatory processes, however, its use during a gout crisis is not yet well understood. Therefore, the objective was to evaluate the parameters of Wistar rats submitted to an experimental gout model and treated with dual cryotherapy protocol. Twenty-one male Wistar rats were used, separated into three groups: control group (CG), lesion group (LG), and lesion + cryotherapy group (LCG). Gout model induction was through intra-articular injection, with urate crystal solution, in the right knee and cryoimmersion treatment was performed for 20 minutes at a temperature of 5° ± 2°C. Seven evaluations and two treatment moments were performed, and the following parameters were analyzed: joint edema, grip strength, joint disability, motor function, and leukocyte migration through synovial lavage. In the statistical analysis we used SPSS 20.0 with Generalized Linear Models, with least significant difference posttest, always with 5% significance level. The treatment reduced edema, promoted strength recovery, and was effective in reducing total leukocytes in the synovial fluid. No difference was observed between the injured groups for joint disability and motor function. Cryotherapy promoted edema reduction and increased pelvic limb grip strength in Wistar rats during the acute period.
Introduction
Gouty arthritis is characterized by the deposition of monosodium urate crystals that occurs due to increased physiological levels of uric acid, also known as hyperuricemia (Keenan, 2017). The characteristic crystallization of gout occurs in soft tissues and peripheral joints, which in turn generates an inflammatory response of periods of high and low intensity (Perez-Ruiz et al., 2014). The supersaturation of urate in the body depends on a relationship of ingestion, synthesis, and excretion, with gout being the final result of untreated systemic hyperuricemia (Nasser-Ghodsi and Harrold, 2015). Besides the concentration of uric acid, other factors can predispose the development of the disease, such as hypertension, obesity, alcohol consumption, diabetes mellitus, and renal alterations (Roddy and Choi, 2014).
The knee and ankle joints are characteristic sites of installation of crystals and commonly manifests in the first metatarsophalangeal joint, called podagra (Bardin and Richette, 2014). Another feature of the chronic joint gout is the presence of macroscopic collections of uric acid in the subcutaneous tissue (Colberg and Henderson, 2017). The acute gout crisis is described as one of the most painful inflammatory joint processes (Rees et al., 2014) that begins from a cascade of macrophage-mediated events that phagocyte crystals present in the joint and release inflammatory mediators that promote neutrophil chemotaxis (Cronstein and Sunkureddi, 2013; Azevedo et al., 2017). Chronicity promotes deformities, changes in joint motion, edema, and has repercussions on radiological findings, such as Martel's sign (Perez-Ruiz et al., 2015).
The literature presents evidence that the chronic use of drugs to control joint inflammation is related to the risk of cardiovascular and cerebrovascular accidents (Barthélémy et al., 2013). Therefore, nonpharmacological treatments are of outstanding importance for the management of clinical signs, being cryotherapy a low-cost resource, easy access to the patient, and with minimized side effects (Crystal et al., 2013; Watkins et al., 2014).
Among the cooling forms, cryoimmersion is efficient for the treatment of joint and soft tissue injuries, since it optimizes the contact area with the target region (Douglas et al., 2013). The reduction of temperature, with consequent metabolic decrease, promotes slowness of nerve conduction, helping in the modulation of symptoms and recovery after intense activities (Murgier and Cassard, 2014). Local ice therapy has been proven to be more efficient in the treatment of individuals with gout than in other types of joint arthritis (Suresh and Das, 2012). There is a hypothesis that the inflammation caused by crystals responds better to the treatment of tissue temperature reduction and that this can also be a method of gout diagnosis. Even so, data are still scarce to support these theories (Guillot et al., 2019).
Although cryotherapy is widely applied in acute lesions, its effects on symptomatology, repercussions on functional capacity, mode of application, cooling time, and temperature have low scientific evidence regarding its use in gouty arthritis. Hence, the need for studies to shed light on the use of ice safely to the patient with gout is founded. Therefore, the aim of this study was to evaluate functional parameters and leukocyte migration in Wistar rats submitted to an experimental model of gout and treated with cryotherapy during the acute period.
Materials and Methods
Animals
We used 21 male Wistar rats, 8 weeks old and weighing ∼250 g, obtained from the Central Bioterium of the Universidade Estadual do Oeste do Paraná (UNIOESTE). During the experiment, the animals were kept in a light/dark period of 12 hours, temperature of 23 ± 1°C, with water and feed ad libitum. Later on, 1 week of adaptation, the animals were randomly distributed among three groups:
CG (control group; n = 7): did not get any type of intervention. LG (lesion group; n = 7): gout induction in the tibiofemoral joint of the right pelvic limb (RPL). LCG (lesion + cryotherapy group n = 7): Drop induction in the tibiofemoral joint of MPD and treatment with immersion cryotherapy.
This experimental, nonblind, randomized trial was conducted after approval of the research protocol by the Ethics Committee on Animal Use (CEUA) of UNIOESTE.
Gout induction injury protocol
The injury induction model was based on the protocol proposed by Coderre and Wall (1987). To prepare the monosodium urate solution (MSU), 4 g of uric acid were dissolved in 800 mL of water, adjusted to pH 8.9 with sodium chloride (NaCl) at 60°C. Subsequently, the solution was cooled in an oven to obtain the needle crystals, which in turn were suspended in phosphate-buffered solution (PBS). For application, the animals were controlled with the help of a flannel and placed in a dorsal decubitus position with manual containment of the RPL. After trichotomy and asepsis with iodinated alcohol (1%), they were administered with the aid of a syringe (1 mL) and needle (13 × 4.5 mm), 50 μL of MSU in the tibiofemoral joint through intra-articular injection only in LG and LCG. For CG, 50 μL of PBS was administered (Fig. 1).
Gout induction in the tibiofemoral joint.
Cryotherapy treatment protocol
To perform the treatment, the animals were manually contained allowing the RPL to be immersed in a container of 1440 cm3 (20 × 12 × 6 cm), containing ice and water, at a temperature of 5° ± 2°C controlled by thermometer (Incoterm), for 20 minutes (Karvat et al., 2018). Two treatments were performed, the first intervention at peak pain (6 hours after injury) and the second 2 hours after the first treatment (Fig. 2).

Time scheme of the moments of evaluation (EV), induction of the gout model, and treatment with cryotherapy.
Functional evaluations
Before the experiment began, all animals were trained and adapted to the equipment used in the evaluations for 3 days, with three repetitions for each type of evaluation. Seven data were collected and obtained: basal evaluation (EV0), before intra-articular injection; EV1, 6 hours after the injury; EV2, immediately afterward the first treatment with cryotherapy; EV3, 1 hour after the first treatment; EV4, 2 hours after the first treatment and 8 hours after the injury; EV5, immediately afterward the second treatment; and EV6, 1 hour after the second treatment. The evaluators were always the same for each type of evaluation and were blinded with respect to the groups.
Articular edema evaluation
To quantify the edema, the animal was immobilized in a flannel and later, three measurements were performed with a nondigital caliper positioned in the region of the knee joint interline, mean laterally in the MPD. The mean of the values obtained was considered.
Evaluation of muscle strength
For evaluation of the RPL muscle strength, a grip strength equipment (Insight®) was used. After manual containment of the animal, the evaluated limb held the transducer in grid format. Thence, three measurements were obtained after the evaluator promoted a traction in the back of the animal, with increasing force, until the animal lost the grip. At the final stage, the average of the values was considered.
Joint disability evaluation
The functional incapacity test was done using a 30-cm-diameter metal cylinder coated with stainless steel-braided mesh (2 mm), which performed three revolutions per minute. Metallic shoes were adapted in both plantar regions of the pelvic limbs, and the right shoe was connected to a signal capture equipment. Thus, during 1 minute of walking the animal, the paw elevation time (PET) of the RPL was recorded. The values were obtained using the Rise-Step software (Insight).
Motor function evaluation
This evaluation aimed to verify the animal's ability to maintain itself at different angles according to its articular proprioception and motor activation. An inclined plane equipment (Insight) composed of an acrylic ramp with a manual mechanism of angular variation (0–90°) and nonslip surface was used. The animal was laid in two directions at the crest of the ramp: the first with the cephalic region upward (vertical) and the second with the cephalic region to the side (transverse), with the pelvic limb under evaluation positioned at the lowest tip of the incline. The evaluation started from 45° and in case the animal won the angulation for 5 seconds, the ramp was elevated another 5° until the manifestation of a minimum reaction of instability or imbalance. Three measurements of maximum angle were performed for each position and considered the mean of the values.
Evaluation of leukocyte migration
After 9 hours of experimentation, all groups were anesthetized through intraperitoneal injection of ketamine hydrochloride (95 mg/kg) and xylazine (12 mg/kg). After noting the absence of motor response to tail clamping and digital folds, the animals were submitted to synovial fluid collection. For this, 5 μL of synovial fluid from the RPL was collected to make a smear slide, which was subsequently stained with May–Grunwald and Giemsa to obtain the percentage of mononuclear and polymorphonuclear leukocytes with the help of a 100 × objective light microscope.
For the total leukocyte count, the articular cavity was washed using 100 μL of 0.9% saline solution and 4 μL of EDTA 5%, collecting 20 μL of the fluid washed with a micropipette, from this, it was diluted in Turck liquid (glacial acetic acid 2 mL, methylene blue 1%, and distilled water 98 mL) with dilution factor varying between 80 and 380 μL depending on the concentration of cells in the synovial fluid. The cells were counted using a Neubauer chamber (cells/mm3), in a 40 × objective light microscope. Four quadrants were adopted to measure the amount of leukocytes. Later, they were submitted to euthanasia for anesthetic overdose.
Statistical analysis
The SPSS 20.0 program was used for data analysis. For the functional analysis comparisons, Generalized Mixed Linear Models were used, and for the leukocyte comparisons, Generalized Linear Models were used; in both cases it was used as least significant difference posttest, always with 5% significance level.
Results
In the joint edema evaluation, there was a significant difference between groups [F(2;120) = 241.2, p < 0.001], between evaluations [F(6;120) = 23.9, p < 0.001], and interaction [F(12;120) = 7.97, p < 0001].
In the EV0 analysis between the groups, there was no significant statistical difference. From EV1 to EV6, the injury groups showed a difference (p < 0.001) with higher values when compared with CG. However, LCG showed reduction of edema compared with LG from EV1 to EV5. Regarding the intragroup evaluations, the CG showed no statistical difference. Both LG and LCG showed a significant statistical increase from the EV1 to EV6 (p < 0.001). Nevertheless, the group treated with cryotherapy showed reduction of values starting from EV2 (Fig. 3).

Joint edema evaluation in centimeters, with medium–lateral diameter measurements. The graphic presents the data according to the moment of evaluation (EV), for the different groups (CG; LG; and LCG). Data expressed as mean and standard deviation. Equal capital letters denote similarities between the groups and lower case letters between the intragroup evaluations. CG, control group; LG, lesion group; LCG, lesion cryotherapy group.
In pelvic limb strength evaluation, there was significant difference between groups [F(2;120) = 163.4, p < 0.001], between evaluations [F(6;120) = 50.5, p < 0.001], and interaction between groups and evaluations [F(12;120) = 18.1, p < 0001].
In the baseline evaluation (EV0) between the groups, the injury groups presented higher values compared with the CG. In EV1, LG and LCG showed statistical differences (p < 0.001) compared with CG, but with a reduction of means. The group treated with cryotherapy showed increased strength from EV2 with a statistical difference compared with LG. In the intragroup analysis, there was no statistical difference for the CG. On the other hand, the injured groups presented a difference from EV1 to EV6, and the treated group started to recover the mean in EV2, showing an increasing increase until EV6 (Fig. 4).
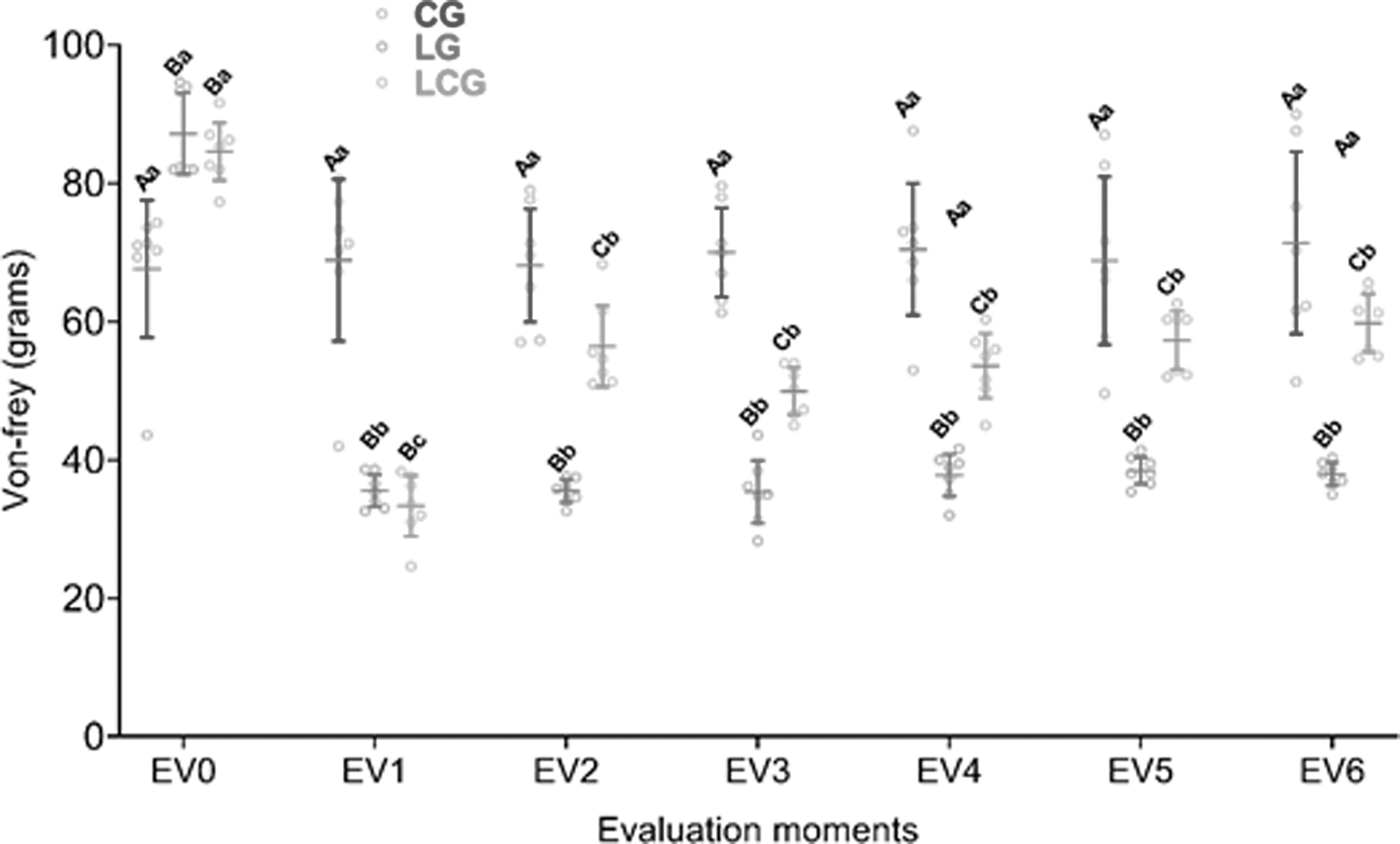
Grip evaluation in grams of the pelvic limb with the injury. The graphic presents the data according to the moment of evaluation (EV), for the different groups (CG; LG; and LCG). Data expressed as mean and standard deviation. Equal capital letters denote similarities between the groups and lower case letters between the intragroup evaluations.
In the PET evaluation, there was a significant difference between groups [F(2;120) = 229.0, p < 0.001], between evaluations [F(6;120) = 26.5, p < 0.001] and interaction [F(12;120) = 10.5, p < 0001].
In the baseline evaluation, there was no difference between the groups. In EV1, LG and LCG obtained statistical difference (p < 0.001) compared with CG. This increase was observed up to EV6, with no difference between the injured groups and reduction of PET. In the intragroup analysis, there was no statistical difference in the CG evaluations. On the other hand, the injured groups presented a difference from EV1 with a decrease from EV2 to EV6. The LCG showed statistical similarity to Basal in EV4 and EV5 (Fig. 5).
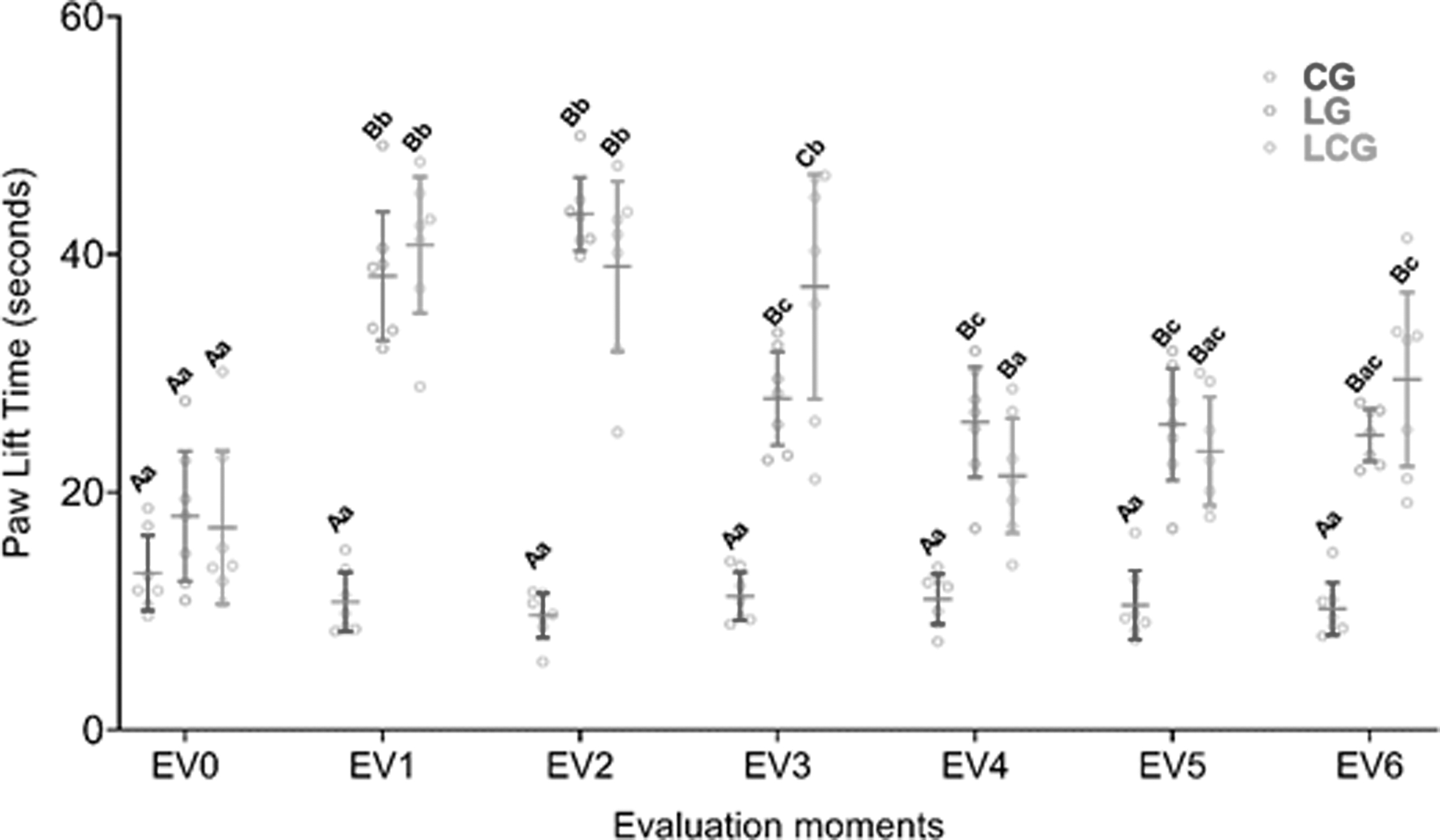
PET evaluation in seconds of the pelvic limb with the injury. The graphic presents the data according to the moment of evaluation (EV), for the different groups (CG; LG; and LCG). Data expressed as mean and standard deviation. Equal capital letters denote similarities between the groups and lower case letters between the intragroup evaluations. PET, paw elevation time.
In the inclined plane evaluation, there was significant difference in the two animal positions between groups [F(2;126) = 4.72, p < 0.001] and [F(2;120) = 22.68, p < 0.001], between evaluations [F(6;126) = 7.46, p < 0.001] and [F(6;120) = 7.35, p < 0.001]; besides interaction between groups and evaluations [F(12;126) = 4.46, p < 0001] and [F(12;120) = 4.37, p < 0001], respectively, in the up position and between groups [F(2;120) = 22.68, p < 0.001], between evaluations [F(6;120) = 7.35, p < 0.001], and interaction between groups and evaluations [F(12;120) = 4.37, p < 0001] in the cross position.
With the animal positioned vertically, there was no difference between the groups in the EV0, EV1, EV5, and EV6. The LG showed statistical differences (p < 0.001) compared with CG only in EV3 and EV4 and LCG in EV2, EV3, and EV4 compared with CG. This increase was observed up to EV6, with no difference between the injured groups. In EV4 and EV5 the group treated with cryotherapy showed higher values compared with LG. In the intragroup analysis, there was no statistical difference in the CG evaluations. On the other hand, the LG and LCG presented difference (p < 0.001) from EV2 with reduction of the mean along the evaluations. However, both groups were similar to the values of the EV0.
With the animal positioned across the board, there was no statistical difference in the EV0 between the groups. The LG showed difference (p < 0.001) in the EV1, EV3, EV4, and EV5 resembling the CG in EV2 and EV6. The LCG, on the other hand, was different from EV1 to EV5, being similar to the CG in EV6. In the analysis between the evaluations, there were no statistical differences for the CG. There were differences between the EV0 and the other evaluations for both injured groups. The LG and LCG showed a recovery of the mean after EV3 showing no difference between the treated and untreated groups (Fig. 6).
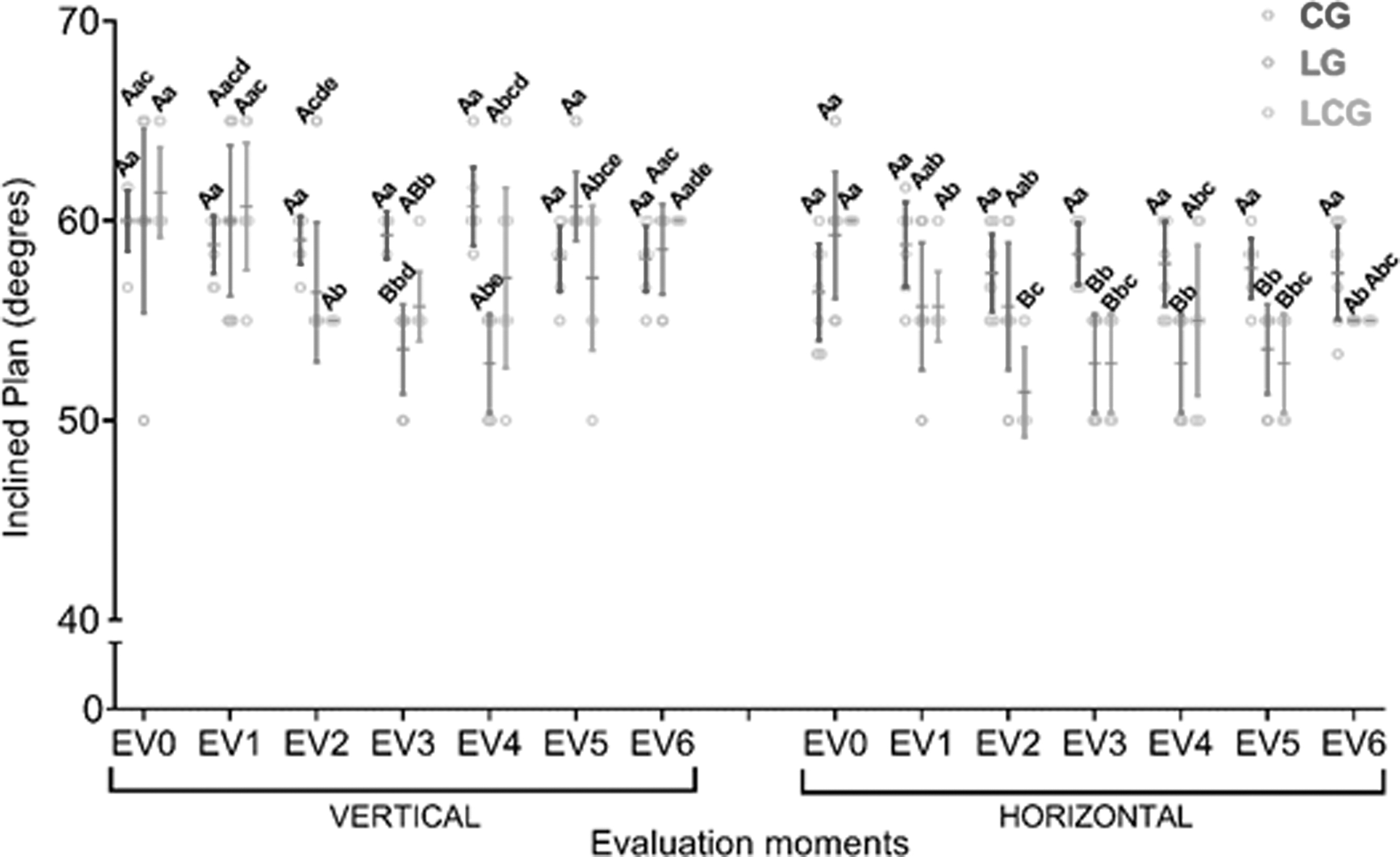
Inclined plan evaluation in degrees according to the position of the animal (vertical or transversal). The graphic presents the data according to the EV, for the different groups (CG; LG; and LCG). Data expressed as mean and standard deviation. Equal capital letters denote similarities between the groups and lower case letters between the intragroup evaluations.
For synovial lavage analysis, there was statistical difference in the three estimates performed between the groups (p < 0.001). For the number of mononuclear leukocytes [Wald(2) = 38.98, p < 0.001; MDD = 46.25] and polymorphonuclear leukocytes [Wald(2) = 73.98, p < 0.001; MDD = 45.95], LG and LCG showed statistical difference when compared with CG. There was no difference between the injured groups. For the total of leukocytes [Wald(2) = 88, 19, p < 0.001; MDD = 552.84], the LG and LCG showed statistical differences (p < 0.001) in relation to the CG (p < 0.001), and were also statistically different among themselves (Fig. 7).
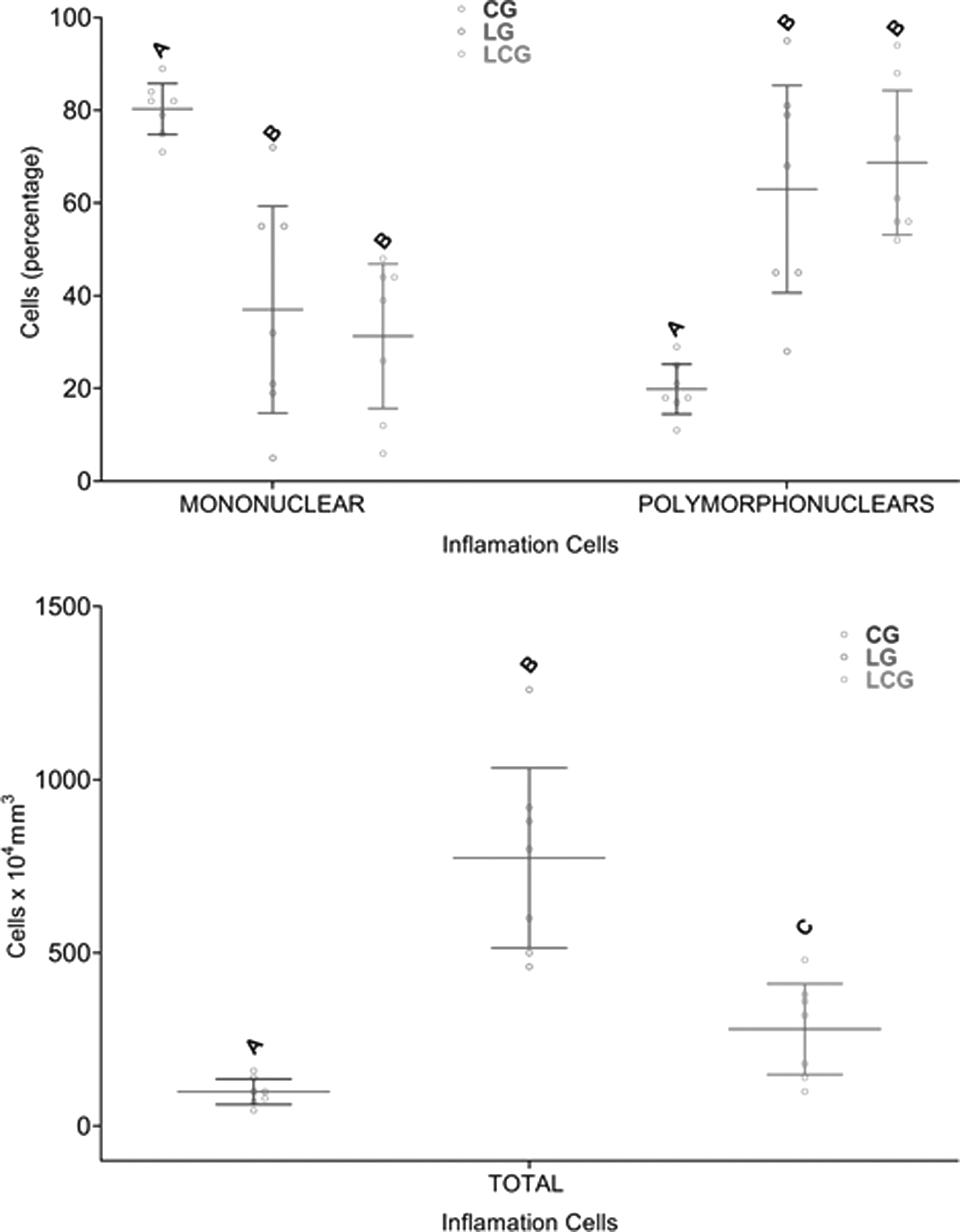
Analysis of the leukocyte count of the joint with the lesion. The graphic presents the data according to the cell type, for the different groups (CG; LG; and LCG). Data expressed as mean and standard deviation. Equal capital letters denote similarities between the groups.
Discussion
According to the results obtained, it can be observed that the experimental model of gouty arthritis induced by urate crystals reproduced symptoms similar to those visualized in an acute attack of the disease, which in turn were quantified by means of functional evaluations and synovial fluid analysis.
Both injured groups showed increased joint diameter 6 hours after the lesion. However, immediately after the first treatment, the LCG obtained a reduction of the mean while the untreated group showed an increasing. Cryoimmersion may have been effective in reducing the presence of exudate in the joint through capillary contraction, making it difficult to release inflammatory factors, such as P, bradykinin and histamine. Therefore, inflammatory suppression is positive because it protects the joint synovial tissue from harmful processes (Miao et al., 2013; Zhang et al., 2018).
In the Miao et al. (2013) study, about the repercussions of hypothermia on gouty arthritis induced by urate crystals on the ankle, adenosine 5′ monophosphate was used to reduce the central temperature of Wistar rats by 16–18°C for ∼10 hours. As a consequence, they demonstrated that hypothermia reduced joint edema and leukocyte infiltration of the treated group. Although the method of temperature reduction differs, both studies had a positive impact on the reduction of edema, although in this research, the temperature was maintained around 5°C.
Cryoimmersion is an advantageous method because it is a noninvasive, low-cost resource and, among the forms of application, allows a large joint area to be cooled. In addition, assisting in this process, there is also the presence of compressive forces of water, also known as hydrostatic pressure, which hinders the edema formation (White and Wells, 2013). The use of cryotherapy with a 2-hour interval is considered a common form in therapeutic settings, as well as used in research (Bleakley et al., 2006).
Regarding the repercussions on grip strength, LG and LCG showed a reduction in values at the time of peak pain, and after the first treatment, LCG obtained an increase in average strength that remained 1 hour after cryoimmersion. The same happened after the second treatment denoting that the ice helped to regain the strength of the treated group. It is common that joint inflammatory diseases manifest reduction of range of motion and muscle strength (Luc-Harkey et al., 2018; Ellegaard et al., 2019).
Despite limited evidence, it is speculated that cryotherapy may, due to phenomena such as vasoconstriction and increased tissue viscosity, hinder the interaction between myofibril cross bridges, which would generate muscle torque deficit (Kalli and Fousekis, 2020), which differs from the results obtained in the present study, in which it is believed that the decrease in nerve conduction, with a consequent increase in the nociceptive threshold (Gutiérrez Espinoza et al., 2010), may have allowed greater muscle torque.
On PET for the injured groups, there was an increase in the mean after the injury, which was expected with the increase of nociception (Tonussi and Ferreira, 1992). Nevertheless, after the treatments, both groups presented a reduction of values showing similar behavior, with no difference regarding the nociception. These results differ from those found by Moreira et al. (2011), in an experimental model of right knee synovitis, in which the animals were treated with cryoimmersion in acute phase, at 5°C, for 20 minutes, resulting in improved joint disability and pain of the group treated with ice. It is known that gouty arthritis presents particularities in relation to other arthritic diseases and that the influence of cryotherapy on this disease needs further investigation, since the induction of joint injury in the experimental model provides changes in physiological patterns (Zhang et al., 2018), which may have influenced the nonrelevant recovery of the treated animals, that is, the sensitivity of the test may not be at a sufficient level for analysis in this injury/treatment model.
Regarding the evaluation of motor function in the inclined plane, it was observed that, in both positions (vertical and transversal), the animals of LG and LCG showed a decrease in tolerance to inclination. Both showed recovery of values throughout the evaluations, and in the transverse position, after the first treatment, the LCG performed worse than the LG. However, at the end of the evaluation, the injured groups showed statistical similarity. Despite recovery throughout evaluations, in this study, it was possible to observe the presence of motor deficit 6 hours after the lesion of LG and LCG corroborating with the findings related to gouty arthritis that the disease is associated with a functional impairment, which leads to reduced productivity and increased vascular morbidities due to their clinical periods of exacerbation (Harrold et al., 2017).
Adie et al. (2012) have shown that cooling may assist in the return of knee function in an acute inflammatory condition, but that this hypothesis is still inconclusive. The effect of angular tolerance reduction after the first LCG treatment, may be ascribed to the fact that cold has the capacity to interfere with sensory/motor uptake, joint positioning, and modulation of nervous signals (Oliveira et al., 2010; Costello et al., 2012). This can occur by reducing the temperature of the painful area and consequent nerve conduction of A and C fibers, reducing the sensation of pain as well as stimuli responsible for stabilization and motor control (Attia and Hassan, 2017). However, during the evaluations, the injured groups do not present differences, demonstrating that the ice did not remain as a harmful agent for the motor control of LCG. One study showed that cooling of the quadriceps muscle and knee does not alter joint proprioception of healthy individuals (Furmanek et al., 2018). The evidence regarding joint repercussions is still contradictory, for individuals with and without associated comorbidities (Costello and Donnelly, 2010).
In the analysis of synovial lavage, a reduction in the number of mononuclear and an increase in the number of polymorphonuclear leukocytes in the LG and LCG was observed. The same behavior occurred in the total leukocyte count, however, LCG obtained a significant reduction compared with LG. The infiltrating monocytes and resident macrophages are the main responsible for initiating the acute attack of the drop, which is followed by an intense invasion of polymorphonuclear leukocytes in the synovial membrane (Pineda et al., 2015). In the study of Scanu et al. (2012), the synovial fluid of 38 patients with gouty arthritis was evaluated, and during acute phases of the disease, they observed an increase of polymorphonuclear cells and also a higher concentration of leukocytes in the first 48 hours. These findings are similar to those of the present study showing changes in synovial fluid composition.
In the Guillot et al. (2019) study, the objective was to evaluate the anti-inflammatory effects of cryotherapy on different types of knee arthritis in humans, performing two applications with local ice, 30 minutes, with an 8-hour interval, and there was a reduction in the levels of interleukin (IL)-6, IL-1-beta, and vascular endothelial growth factor for individuals with microcrystal-induced arthritis.
Although the present research did not perform a specific assessment of cytokines, it is potential to correlate the findings based on the reduction of inflammatory cells, demonstrating that local cryotherapy was effective in reducing leukocyte migration. Therefore, this research was able to demonstrate that cryoimmersion treatment promotes positive effects during gout attack and that it is in need of further scientific investigation to shed light in all appropriate parameters to safely perform on the patient.
Conclusion
It can be concluded that the use of cryotherapy during the exacerbation period of the experimental gout model, reduced joint edema, promoted increased limb grip strength, and decreased the total number of leukocytes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.