
Abstract
Measuring cardiac output is used to guide treatment during postresuscitation care. The aim of this study was to compare Doppler echocardiography (Doppler-CO) with thermodilution using pulmonary artery catheters (PAC-CO) for cardiac output estimation in a large cohort of comatose out-of-hospital cardiac arrest (OHCA) patients undergoing targeted temperature management (TTM). Single-center substudy of 141 patients included in the TTM trial randomly assigned to 33 or 36°C for 24 hours after OHCA. Per protocol, PAC-CO and Doppler-CO were measured simultaneously shortly after admission and again at 24 and 48 hours. Linear correlation was assessed between methods and positive predictive value (PPV) and negative predictive value (NPV) of Doppler to estimate low cardiac output (<3.5 L/min) was calculated. A total of 301 paired cardiac output measurements were available. Average cardiac output was 5.28 ± 1.94 L/min measured by thermodilution and 4.06 ± 1.49 L/min measured by Doppler with a mean bias of 1.22 L/min (limits of agreements −1.92 to 4.36 L/min). Correlation between methods was moderate (R2 = 0.36). Using PAC-CO as the gold standard, PPV of a low cardiac output measurement (<3.5 L/min) by Doppler was 33%. However, the NPV was 92%. Hypothermia at 33°C did not negatively affect the correlations of CO methods. In the lowest quartile of Doppler, 13% had elevated lactate (>2 mmol/L). In the lowest quartile of thermodilution, 36% had elevated lactate (>2 mmol/L). In ventilated OHCA patients, the two methods for estimating cardiac output correlated moderately and there was a consistent underestimation of Doppler-CO. Absolute cardiac output values from Doppler-CO should be interpreted with caution. However, Doppler can be used to exclude low cardiac output with high accuracy. TTM at 33°C did not negatively affect the correlation or bias of cardiac output measurements. ClinicalTrials.gov ID: NCT01020916.
Introduction
After out-of-hospital cardiac arrest (OHCA), anoxic brain injury is the primary cause of death in patients admitted comatose to hospital (Laver et al., 2004; Witten et al., 2019). Hemodynamic instability with myocardial dysfunction and high vasopressor requirements may contribute to neurological injury (Bro-Jeppesen et al., 2014, 2015; Bhate et al., 2015; Sekhon et al., 2017; Grand et al., 2019a–c), whereas also a significant part of patients die from cardiovascular collapse (Laver et al., 2004; Witten et al., 2019). Hemodynamic instability is most frequent encountered in the early post-OHCA period during targeted temperature management (TTM) (Laurent et al., 2002; Nielsen et al., 2013; Jentzer et al., 2018). Cardiac output has been shown to be low especially for patients undergoing TTM at 33°C (Bro-Jeppesen et al., 2014; Grand et al., 2019b). Inotropes and vasoactive drugs are titrated to increase blood pressure and cardiac output to achieve satisfactory organ perfusion (Cecconi et al., 2014). Several modalities for estimating cardiac output are available, each with different advantages and pitfalls (Chatterjee, 2009). Often thermodilution is used by infusing cold fluid through a pulmonary artery catheter (PAC-CO) (Ganz et al., 1971). This method is costly and carries a risk of complications (Harvey et al., 2005). A noninvasive, alternative approach is the transthoracic Doppler echocardiography (Doppler-CO), which is fast in the hands of skilled users and without any apparent risk for the patient (Huntsman et al., 1983). A previous study has indicated that accurately calculated cardiac output can be measured with noninvasive ultrasound in patients in the intensive care unit (ICU) (Huntsman et al., 1983). However, this approach remains to be established in a large cohort of comatose OHCA patients treated with TTM and thus sedated and receiving mechanical ventilation. Furthermore, because thermodilution uses a temperature gradient, low body temperature could possibly interfere with the validity of the measurements. The purpose of this study was to compare transthoracic Doppler-CO with PAC-CO for cardiac output estimation during TTM after OHCA.
Materials and Methods
Study design and patients
This was a retrospective study on prospectively collected data from the TTM trial (Nielsen et al., 2013) at Copenhagen University Hospital, Rigshospitalet. Patients underwent a TTM protocol of either 33 or 36°C for 24 hours before rewarming. We consecutively enrolled successfully resuscitated, comatose (Glasgow Coma Scale Score ≤8) OHCA patients with presumed cardiac cause. Exclusion criteria were refractory shock (sustained systolic blood pressure <80 mmHg despite treatment), unwitnessed asystole as primary rhythm and time from return of spontaneous circulation (ROSC) to randomization above 4 hours. An analysis of the hemodynamic impact of the temperature intervention has been published previously (Bro-Jeppesen et al., 2014). The study was approved by the local scientific ethics committee (H-1-2010-059). A written informed consent was obtained from close relatives or guardians after hospitalization and from all patients regaining consciousness according to Good Clinical Practice.
Study procedures
TTM was initiated immediately after randomization. After 4 hours, all patients had reached target temperature, which was maintained for additional 24 hours followed by rewarming with 0.5°C per hour to 37°C. All patients were sedated, intubated, and mechanically ventilated. Active cooling with surface cooling (Thermowrap with Allon unit, Israel) was used. Sedation was titrated with propofol/fentanyl to a Richmond Agitation-Sedation Scale score of −4. If needed, neuromuscular blocking agents were used to reduce shivering.
Hemodynamic treatment goals consisted of central venous pressure of 10–15 mmHg, mean arterial blood pressure (MAP) ≥65 mmHg, and urine output >1.5 mL/kg/hour. Primarily, norepinephrine and dopamine were used as first-line vasopressors. Per protocol as soon as possible at the ICU, a balloon-tipped, 7.5F triple lumen PAC (Swan-Ganz, Edwards Lifesciences, Irvine, CA) was inserted. Cardiac output was measured using the thermodilution technique at insertion of the PAC (T0), after 24 hours (T24) and after 48 hours (T48). A rapid injection of 10 mL of cold isotonic glucose was used with a temperature gradient of at least 10°C. The mean of three measurements with <10% variance was used. As previously reported, interobserver comparison of cardiac output measurements in 13 patients showed low bias (0.42%; mean difference of 0.02 ± 0.52 L/min) with a good reproducibility assessed by a coefficient of variation of 3% corrected for duplicate measurements. The impact of hypothermia on cardiac output from thermodilution has previously been published (Bro-Jeppesen et al., 2014; Grand et al., 2020a, b). Upon insertion of the PAC (T0), cardiac output was estimated with transthoracic echocardiography and simultaneous with thermodilution. Furthermore, in a consecutive group of the first 130 patients the paired measurements were also performed after 28 hours before commencing rewarming (T28), and at normothermia, 48 hours after ROSC (T48). Transthoracic echocardiography was performed with the Philips CX50 cardiac ultrasound system (Philips Healthcare, Best, The Netherlands) with the patient in supine position tilted 15° toward left to allow for acquisition of apical views. Images were stored for offline analysis using Philips Xcelera analysis software version 3.1 (Philips Healthcare). For Doppler recordings, the average of at least three consecutive cardiac cycles were recorded during stable heart rhythm avoiding post-extra systolic beats. Two experienced echocardiographers (J.B.J. and J.K.) performed all recordings and the following analyses. The stroke volume (SV) was calculated by measuring: (1) the left ventricular outflow tract diameter (LVOT) from the parasternal window used to calculate the cross-sectional area (LVOT area = [diameter of LVOT/2]2 × π) and (2) from apical 5 chamber view the LVOT blood velocity profile was recorded with pulsed-wave Doppler and the area under the velocity time curve termed “Velocity Time Integral” (VTI) measured, which represent the stroke length (Quiñones et al., 2002). The product of VTI (cm/stroke) and the cross-sectional area of the valve (cm2) produce an estimate of SV (cm3/stroke). Cardiac output was automatically calculated by the software by multiplying SV with heart rate.
The offline analyses were performed blinded to allocated temperature treatment and to invasive measurements. Data from PAC measurements were collected for research purposes only. Mixed venous oxygen saturation (SvO2) and lactate were analyzed from the PAC at T0, T28, and T48. In addition, heart rate, MAP, and temperature were obtained for the first 48 hours after ROSC.
The main variables of interest were mean bias between Doppler-CO and PAC-CO of all measurement pairs, correlation of methods and proportion of measurement pairs, which were within acceptable range of each other. Acceptable range was defined as 1 L/min difference between measurements. Additional analyses were made for TTM at 33/36°C. We defined low cardiac output as a measurement <3.5 L/min.
Statistics
Categorical data are presented as count and percentages. Continuous data are presented as median (quartile 1 and quartile 3) or mean ± standard deviation (SD) according to distribution of data. Categorical data were compared using Fisher's exact test. Student's t-test or Mann–Whitney U-test was used for continuous data as appropriate. A two-sided p-value <0.05 was considered statistically significant. For agreement between the two methods, Bland–Altman analyses were applied calculating bias and presented with limits of agreements (LOA) (bias ±2SD). We used Spearman correlation coefficients to estimate correlations displayed as rho (r) and p-values. We calculated sensitivity and specificity of Doppler to estimate low cardiac output compared with thermodilution (gold standard) in addition to positive and negative predictive values (NPVs). All statistical analyses were performed using the SAS statistical software, version 9.4 (SAS Institute, Cary, NC).
Results
A total of 171 OHCA patients were included in the trial from November 2010 to January 2013. Nineteen (11%) patients were excluded because of missing PAC data (7 patients died before insertion of PAC, 10 patients did never receive PAC by discretion of the treating physician, and 2 patients did not have registered hemodynamic data). Eleven (6%) did not have echocardiographic data registered, resulting in 141 patients included in this study. Baseline data and comorbidities of study population stratified according to temperature strata are given in Table 1. Patients were 61 ± 11 years, 86% were men, and the body mass index (BMI) was 26 ± 4 kg/m2. Cardiac arrest was witnessed in 91% of cases, 80% had shockable rhythm as the first registered, time to return of spontaneous circulation was 23 (14–30) minutes, 57% had ST elevations in initial ECG, and percutaneous coronary intervention was performed in 55% of patients.
Prehospital and Prearrest Data of Study Population
AMI, acute myocardial infarction; BMI, body mass index; CAG, coronary angiography; COPD, chronic obstructive pulmonary disease; CPR, cardiopulmonary resuscitation; PCI, percutaneous coronary intervention; Q1–Q3, interquartile range; ROSC, return of spontaneous circulation; SD, standard deviation; TCI, transitory cerebral ischemia; TTM, target temperature management.
Comparing Doppler with thermodilution
There were 120 paired cardiac output measurements at T0, 99 paired measurements at T28, and 82 paired measurements at T48, resulting in a total of 301 paired measurements (Fig. 1).
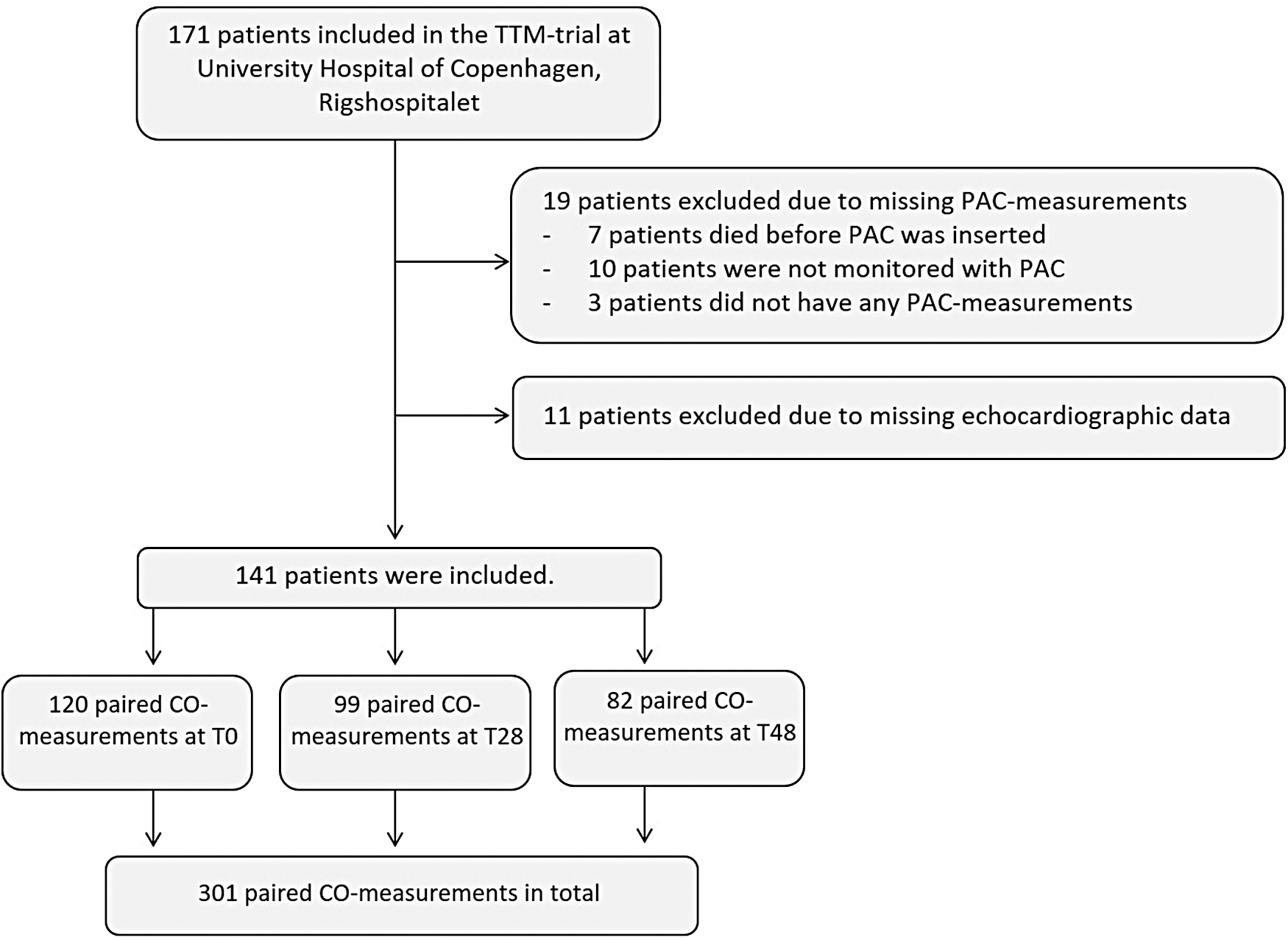
Consort diagram depicting the flow of patients included in the TTM trial at Copenhagen University Hospital Rigshospitalet. CO, cardiac output; PAC, pulmonary artery catheter; TTM, targeted temperature management.
Overall correlation between methods was R2 = 0.36. Average PAC-CO was 5.28 ± 1.94 L/min and Doppler-CO was 4.06 ± 1.49 L/min with a mean bias of 1.22 L/min (LOA −1.92 to 4.36 L/min) (Fig. 2). Of all paired measurements, 105 (35%) were within clinical acceptable range, which we defined as 1 L/min. A total of 148 (49%) were within 1.5 L/min; 195 (65%) were within 2 L/min; and 232 (77%) were within 2.5 L/min.
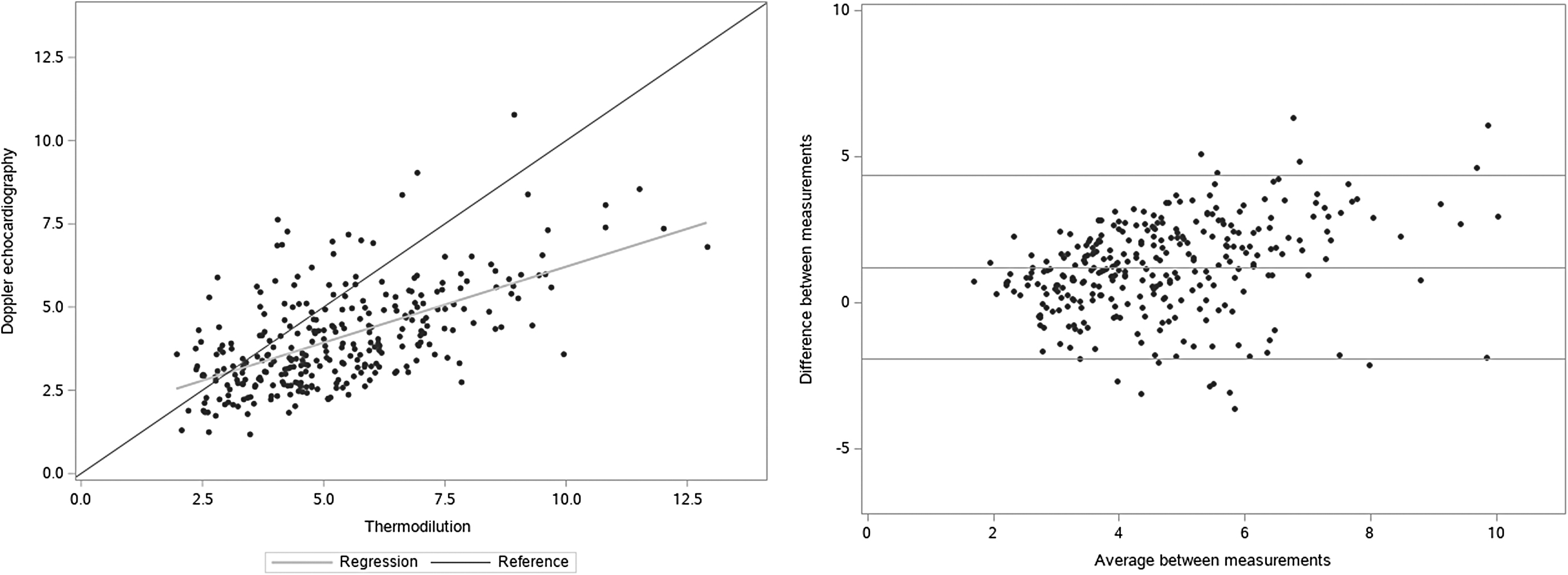
Bland–Altman plot (right) and linear regression (left) comparing cardiac output measured with Doppler-CO and PAC-CO. Doppler-CO, Doppler echocardiography; PAC-CO, thermodilution using pulmonary artery catheters.
For patients with BMI below the median, the correlation between methods was R2 = 0.34. For patients with BMI above the median, the correlation between methods was R2 = 0.40. BMI did not significantly affect the correlation between methods (pinteraction_BMI*doppler = 0.34).
The lowest quartile of PAC-CO was 3.42 L/min. The lowest quartile of Doppler-CO was 2.87 L/min. Ten (33%) patients were in the lowest quartile of both Doppler and thermodilution.
In the lowest quartile of Doppler-CO, 13% had elevated lactate (>2 mmol/L). In the lowest quartile of PAC-CO, 36% had elevated lactate (>2 mmol/L). In the highest quartile of Doppler-CO, 24% had elevated lactate (>2 mmol/L). In the highest quartile of PAC-CO, 8% had elevated lactate (>2 mmol/L).
Low cardiac output, defined as a cardiac output measurement <3.5 L/min, was present in 43 measurement in both modalities (true positive), 13 had low PAC-CO, but not low Doppler-CO (false negative), 87 had low Doppler-CO but not low PAC-CO (false positive), and 158 measurement pairs were not low in any of the modalities (true negative). Using thermodilution as the gold standard, sensitivity and specificity of Doppler-CO for identifying low cardiac output is calculated as follows: sensitivity = 43/43 + 13 = 77%. Specificity = 158/158 + 87 = 64%. Positive predictive value: 43/(43 + 87) = 33%. NPV = 158/(158 + 13) = 92%.
Cardiac output during hypothermia
During TTM there was 50 patients with paired cardiac output measurements in the TTM33 group and 49 paired measurements in the TTM36 group. Average cardiac output was significantly higher in the TTM36 group compared with the TTM33 group measured both by Doppler (TTM33: 3.26 ± 0.97 L/min, TTM36: 3.93 L/min, p < 0.0001) and thermodilution (TTM33: 4.08 ± 1.27 L/min, TTM36: 5.15 L/min, p < 0.0001) (Fig. 3). In TTM33, mean bias between Doppler and thermodilution was 0.81 L/min (LOA −1.55 to 2.95 L/min) and correlation was R2 = 0.56 (Fig. 4). In TTM36, mean bias between Doppler and thermodilution was 1.22 L/min (LOA −1.66 to 4.10 L/min) and correlation was R2 = 0.28 (Fig. 3). Interaction analysis showed that Doppler and thermodilution correlated significantly better in patients in the TTM33 group compared with TTM36 (p = 0.035).
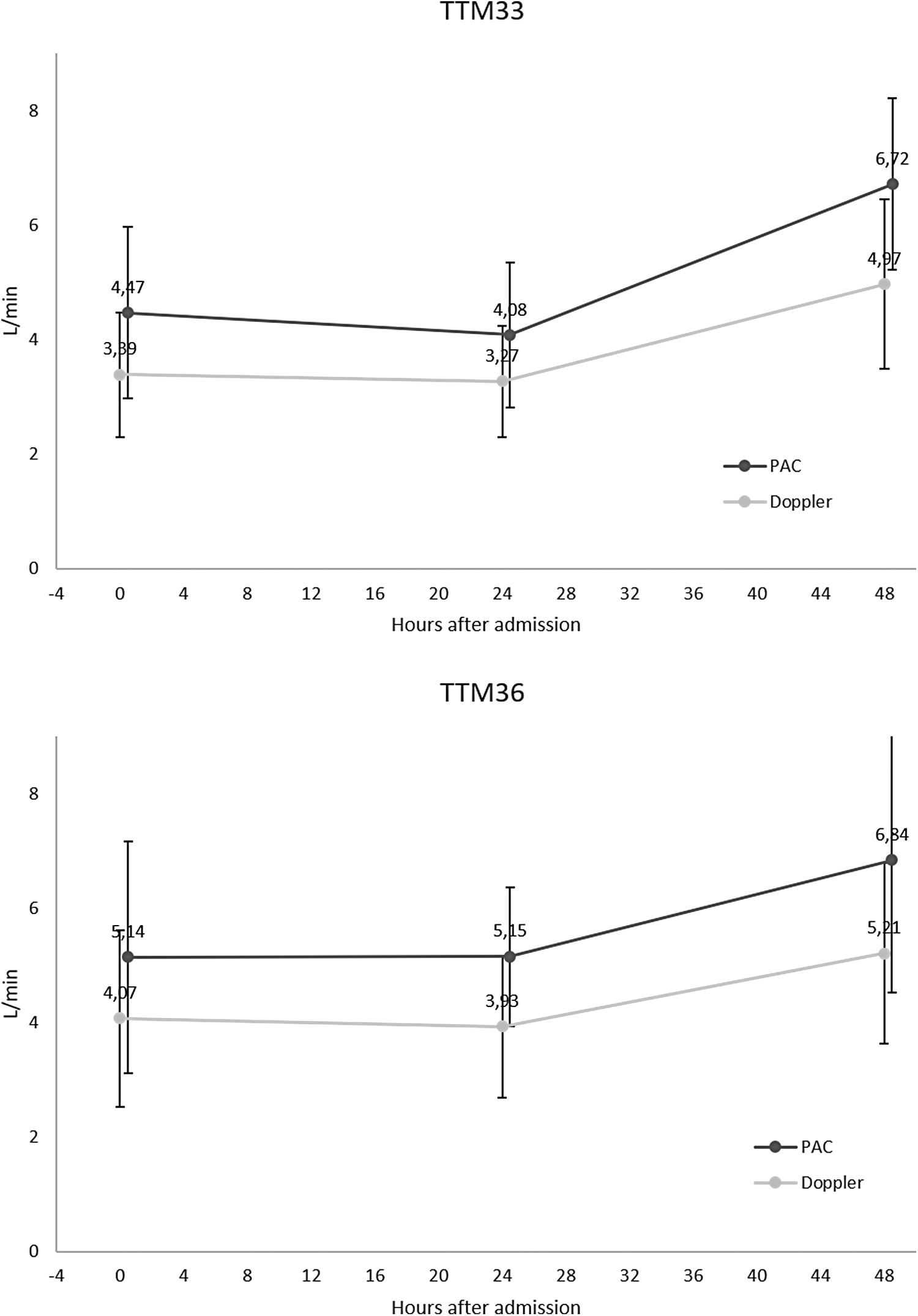
Temporal changes in cardiac output measured by two different methods during TTM at 33°C (top graph) and 36°C (bottom graph). PAC indicates cardiac output measured by PAC; Doppler indicates cardiac output measured by Doppler-CO. The colored dot represents the mean value. Error bars represent standard deviation.
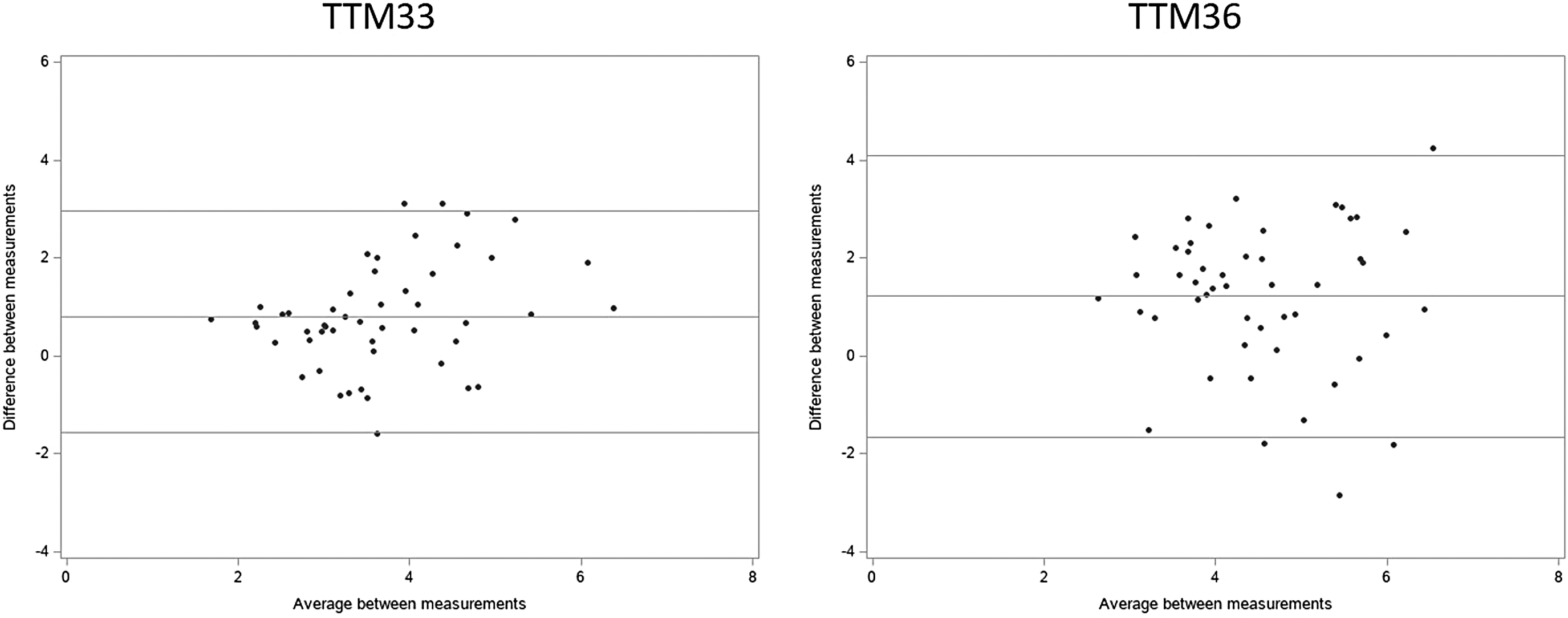
Bland–Altman plot comparing cardiac output measured with Doppler-CO and PAC-CO. Measurements are performed during the maintenance phase of TTM (T28). TTM at 33°C (left graph); and TTM at 36°C (right graph).
Correlations between cardiac output and hemodynamic variables
Correlations between mean hemodynamic variables during TTM with cardiac output measured with thermodilution and Doppler at admission are given in Table 2. Cardiac output measured with Doppler correlated significantly with heart rate and LVEF. However, this modality did not correlate with any other hemodynamic variable or with body surface area. Cardiac output measured with thermodilution correlated significantly with heart rate, LVEF, central venous saturation, height, weight, and body surface area. The correlation with heart rate was, however, much weaker than for Doppler (Doppler: R2 = 0.23, p < 0.0001; thermodilution: R2 = 0.06, p = 0.04).
Correlations Between Hemodynamic Variables and Cardiac Output Measured by Doppler (Left Column) and Thermodilution (Right Column) by Spearman Correlation Coefficients (r)
Bold indicates statistical significance.
BSA, body surface area; CI, cardiac index; CVP, central venous pressure; LVEF, left ventricular ejection fraction; MAP, mean arterial blood pressure; n/a, not applicable; PCWP, pulmonary capillary wedge pressure; SvO2, mixed venous oxygen saturation; VTI, velocity time integral.
Discussion
We prospectively and consecutively collected paired measurements of cardiac output with two methods: Doppler-CO and thermodilution in ventilated patients undergoing TTM after OHCA. To our knowledge, this is the largest validation study of cardiac output measurements in comatose OHCA survivors included as part of a clinical pragmatic trial. We found an overall moderate correlation and a clinically significant underestimation by Doppler with mean bias of ∼1 L/min. Considering the individual measurement pairs, only 35% were within clinical acceptable range, which we prespecified as 1 L/min. However, the Doppler method was able to identify patients with low CO <3.5 L/min with good accuracy.
Transthoracic Doppler-CO is a widely used noninvasive approach of estimating hemodynamic function and cardiac output. In the hands of skilled users, this modality has been showed to give accurate estimates of cardiac output in previous small studies of non-OHCA patients (Huntsman et al., 1983). Our data indicate that Doppler-CO can rule out low CO with an acceptable NPV of 92%, suggesting that the Doppler method may be useful in a clinical setting. However, our data identified a systematic bias in terms of the precision of estimating CO by Doppler in comatose OHCA patients, owing to a clinically significant underestimation of cardiac output and only moderate correlation. This means that Doppler with acceptable certainty can categorize patients with low cardiac output but is less useful when a precise measurement is needed, that is, for research purposes. This study was pragmatic, and we used the measurements from the LVOT, although the setting for acquiring ultrasound was not optimal. In patients with ideal ultrasound conditions, the validity of Doppler may be better. However, in patients with lower BMI as a measure of better ultrasound conditions, the validity of Doppler did not improve. Invasive hemodynamic monitoring has recognized complications in the clinical setting, some of which may be detected by the adjuvant use of echocardiography. Furthermore, echocardiography gives extensive clinical information regarding mechanical cardiac complications, valvulopathy, or reduced systolic function information besides measuring cardiac output. Therefore, it is unlikely, that one method, Doppler or thermodilution, can stand alone in a patient with unexplained hemodynamic instability (Jensen et al., 2021).
Staer-Jensen et al. (2018) did a similar study in 26 patients undergoing TTM. They compared pulse index continuous cardiac output (PICCO) (Litton and Morgan, 2012), which is a combination of pulse contour analyses and transpulmonary thermodilution, with Doppler-CO. They measured Doppler cardiac output as in this study. Of the 23 paired measurements, Staer-Jensen et al. found a low bias between PICCO and transthoracic echocardiography (TTE); however, LOA were wide (they report SV as opposed to cardiac output, so absolute number cannot be compared with our data). Visual examination of their Bland–Altman plots indicated that they also found better agreement when cardiac output is low (Staer-Jensen et al., 2018), but they did not compare measurements at different temperature levels.
In a similar study of 15 patients subjected to TTM after cardiac arrest, Souto Moura et al. compared PICCO with Doppler-CO for estimating cardiac output. Under normothermia, in contrast to our findings, they found a good correlation between measurements with all the measurements differing by <0.5 L/min. However, during hypothermia defined as <36°C, the bias and precision fell; the mean bias was −0.43 L/min, with LOA of −1.60 to 0.75, and 44% (8/18) of the paired measurements were within 0.5 L/min (Souto Moura et al., 2018).
A recent meta-analysis aiming at analyzing the consistency and interchangeability of cardiac output measurements by Doppler-CO and thermodilution identified 68 studies comparing the two modalities (Zhang et al., 2019). No significant differences were found between the methods (random effects model: mean difference, −0.14 L/min; 95% confidence interval, −0.30 to 0.02; p = 0.08). However, in some scenarios, such as high CO, low sedation, or with physiological structural changes, the accuracy of measurement by Doppler-CO was questionable. Of note, only one study investigated cardiac arrest patients (Souto Moura et al., 2018).
Thermodilution is generally considered the gold standard, thus measurements from Doppler-CO should be interpreted with caution in OHCA patients undergoing TTM. We found that thermodilution cardiac output correlated significantly with SvO2 and body surface area, which is expected and supports the validity of thermodilution.
In addition to complications for the patients, thermodilution have some limitations. The accuracy can be affected by blood and injectate temperature, volume of injectate, improper positioning of the PAC, and wrong injection technique (Levett and Replogle, 1979). Based on these considerations, it is to be expected that thermodilution measurements have considerable imprecision. It could be hypothesized that a lower body temperature (i.e., 33°C) would influence the thermodilution methods by affecting the temperature gradient. However, our data indicate that correlations and agreements between methods were not negatively affected during hypothermia. In addition, Doppler-CO has some sources of imprecision, because the measurements are highly dependent on the quality of TTE imaging, which can be challenging during hypothermic conditions with sedated patients on a ventilator. Aortic blood velocity is measured by means of the Doppler effect, using the relationship (Huntsman et al., 1983). Angle between the ultrasound beam and the blood flow vector is assumed to be 0°, so in the case of an angle >0°, the blood velocity will be underestimated. Placement of the pulsed-wave Doppler should be in the LVOT. Our data were measured in the acute setting with patients bedridden on their back, which may contribute to an angular error. This may explain, why our data indicate some differences between the two methods. Furthermore, the cross-sectional area of the aortic valve is assuming the valve is a perfect circle, which is often not the case. Because the diameter is squared, small imprecisions can have great effect on the estimate. The use of three-dimensional echocardiography to determine the exact area of the aortic valve is possible and could be investigated in future studies.
Limitations
There are several limitations in this study. First, this was a retrospective single-center study without sample size calculations limiting firm conclusions and external validity. Second, image quality of echocardiography assessment was challenging with sedated patients on a ventilator. Third, although measurements were performed at the same time point, one measurement was performed after the other thus making possible small variations in hemodynamics during the seconds/minutes from one measurement to the other. Fourth, we did have a significant number of excluded patients. Research in the acute setting with severely sick intensive care patients is difficult and the number of patients without hemodynamic measurements shows that the two methods can be challenging to perform in some patients. Fifth, although the results of the two methods were blinded from the investigators, some degree of unblinding cannot be excluded, because patient data were accessible in the department. Sixth, we used thermodilution as the gold standard; however, there is imprecision related to this method also. Nevertheless, these limitations reflect real-life conditions.
Conclusions
Cardiac output measured with Doppler-CO correlated moderately with cardiac output measured with a PAC-CO. There was a mean bias of 1 L/min, with Doppler measuring lower, which may have potential clinical significance. Absolute cardiac output values from Doppler should be interpreted with caution. However, Doppler can be used to exclude low cardiac output with relatively high accuracy. TTM at 33°C did not negatively affect the correlation or bias of cardiac output measurements.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
J.K. was supported by unrestricted grants from the Novo Nordisk Foundation: NNF17OC0028706. C.H. was supported by an unrestricted grant from Lundbeck Foundation (R186-2015-2132). The TTM trial was supported by independent research grant from TrygFonden (Denmark) (Grant No: 7-12-0454).