
Abstract
To illustrate our experience with two cases of neonatal life-threatening hyperkalemia during therapeutic hypothermia (TH) despite a normal acid–base status, urine output, and preserved renal function. Clinical cases are presented from Pediatric Intensive Care Unit (PICU) admission to the onset of the hyperkalemia, with related complications and after resolution. Similar cases were not retrieved from a critical review of pertinent literature. Severe hyperkalemia pathophysiology and risk factors have been debated. Two full-term adequate for weight female neonates were admitted to PICU because of perinatal asphyxia who underwent TH. Prenatal history was completely uneventful, nor hereditary genetic conditions were reported; moreover, long-term follow-up ruled out any metabolic or renal disease. Despite an accurate evaluation of previous clinical series and literature on TH and perinatal asphyxia, these hyperkalemic episodes remain unexplained. The hypoxic–ischemic insult may affect multiple organs, mainly central nervous system, heart, lung, and kidneys; acute muscle breakdown and consequent rising of myoglobin may also have a precipitating role in acute kidney failure (AKF) and hyperkalemia. Electrolyte imbalance is a possible finding as a consequence of combined cell injury and AKF. In contrast, an isolated severe hyperkalemia is exceedingly rare in nonoliguric neonates.
Introduction
Perinatal asphyxia is not infrequent even in developed countries, having an incidence of ∼1–2 per 1000 live births (Pierrat et al., 2005; McGuire, 2007), thus representing an important cause of cerebral palsy and associated neurological disabilities in children. The hypoxic–ischemic insult may lead to multiple organ dysfunction affecting central nervous system, heart, lungs, and kidneys; at the same time, myoglobin derived from muscle breakdown in asphyxiated infants plays a major role in precipitating renal failure, as recognized >30 years ago (Kojima et al., 1985). Electrolyte imbalance is described as a possible complication of cellular injury and kidney impairment in these patients. However, to our knowledge, no cases of severe life-threatening hyperkalemia have ever been reported in the absence of oliguric renal failure. We describe our clinical experience with two full-term neonates who presented this rare complication under the course of therapeutic hypothermia (TH): pathophysiology and risk factors remain on debate.
Illustrative Case 1
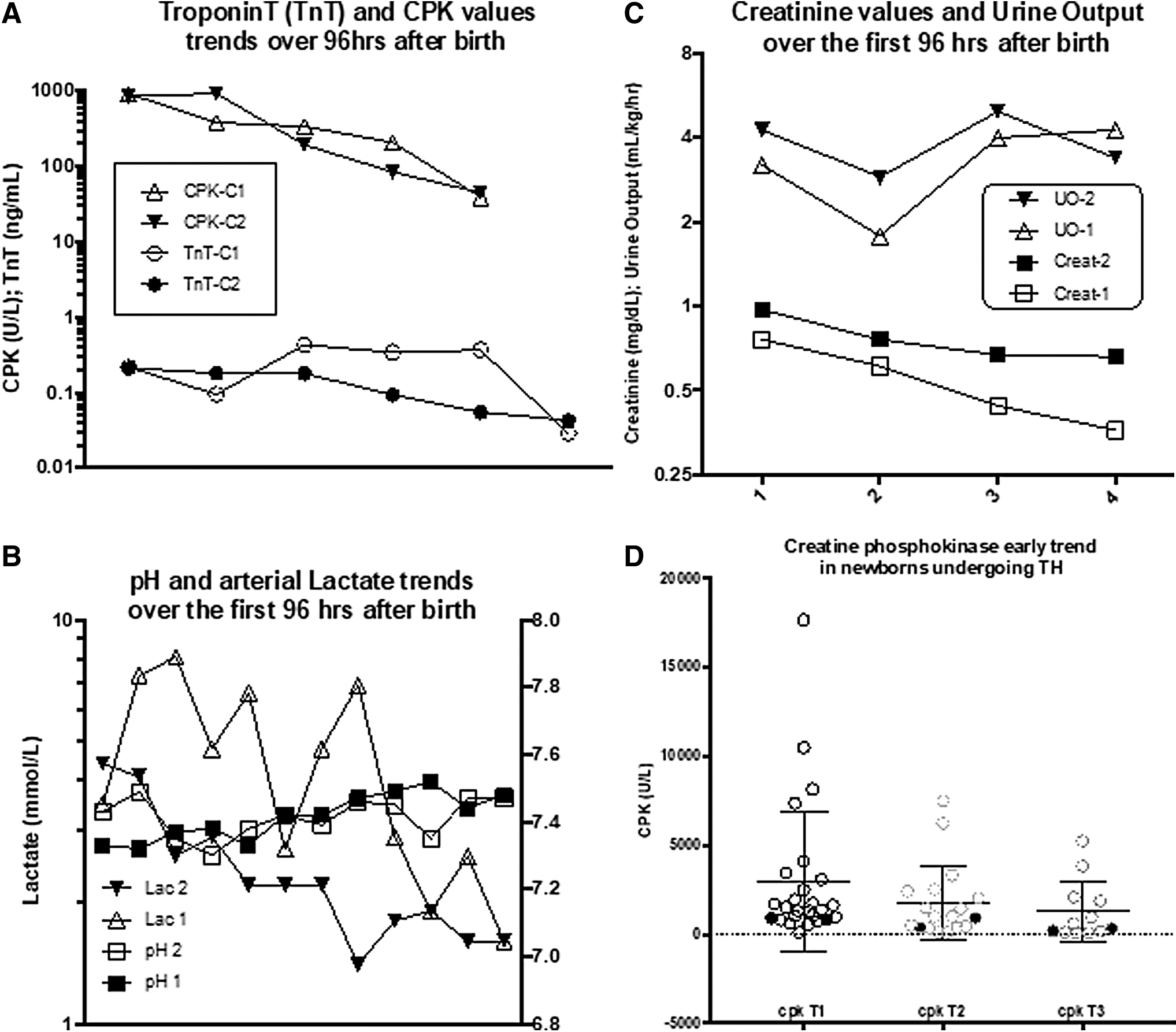
A full-term female infant [body weight (BW) 3.7 kg] demonstrated sudden fetal distress just after the beginning of her mother's labor at 38 weeks of gestation and was born by vaginal delivery. Amniotic fluid was markedly hemorrhagical, and a placental disruption was diagnosed. At birth, she was tachypneic and dyspneic, Apgar score was 4–5 at 1 and 5 minutes, respectively. No cardiac arrest nor requirement for chest compressions was reported. She was given oxygen support and porcine surfactant bronchoalveolar lavage. Her cord blood pH was 6.98, base excess (BE) −20 mol/L, and lactates 8 mmol/L. After a few minutes on nasal prongs continuous positive airway pressure (CPAP), due to increasing respiratory distress and neurological impairment, she underwent tracheal intubation and referral for TH. Respiratory conditions worsened again, despite a repeated Curosurf™ administration, evolving toward severe hypoxemia. High ventilation settings were needed shortly after Pediatric Intensive Care Unit (PICU) admission (Oxygenation Index 27). Before echocardiographic assessment, a test dose of intratracheal iloprost showed a marked oxygenation response, demonstrating early pulmonary hypertension, and 20 ppm inhaled nitric oxide (iNO) was introduced. Her respiratory condition stabilized, and oxygen support could be decreased to 0.40 over 2 hours. A fluid load was performed, achieving a central venous pressure of 8 mmHg, whereas hemodynamics stabilized after epinephrine 0.1 mcg/(kg·min) introduction, then i.v. milrinone was added; urine output was maintained using fenoldopam 0.2 mcg/(kg·min) infusion. Midazolam and remifentanil were used during the 72-hour TH. On day 3, a sudden increase of potassium level was noticed (peak 10.2 mEq/L), in absence of oliguria/acidosis (3.5 mL/[kg·h] urine output), with moderate rhabdomyolysis signs (peak creatine phosphokinase [CPK] 961 UI/L, normal values 30–170 UI/L) and myoglobinuria. Cardiac enzymes were also increased (Troponin T [TnT] 0.45 ng/mL, normal values <0.014 ng/mL; creatine-Kinase-MB (CK-MB) 13, normal values <5.0 ng/mL), without any contractility impairment. Emergency medical treatment (including insulin/glucose and bicarbonate) successfully controlled hyperpotassemia, which resolved without relapses. Muscle enzyme levels declined over the next 3 days. The infant could be weaned from the respiratory and hemodynamic support uneventfully, and spontaneous respiration was resumed after a further 3-day course of nasal CPAP. Neurological assessment was normal, and she could be fed orally without problems. On cerebral ultrasound, a minimal choroid plexus bleeding was detected, without clinical correlates.
Illustrative Case 2
A female infant was born at term (39 weeks gestational age) from an uneventful pregnancy (BW 2.95 kg), whereas meconium-stained amniotic fluid and respiratory distress were present immediately after birth. Apgar score was 5–5 at 1 and 5 minutes, respectively. Despite postnatal care, the baby remained hyporeactive and a metabolic acidosis developed (pH 7.1, BE −19 mol/L), requiring intravenous fluid loading and bicarbonate administration. On arrival to the PICU, she was still lethargic: crying was poorly inducible with a marked hypotonia. She underwent tracheal intubation and central line placement; TH was induced through a cooling mattress. Low dose midazolam and remifentanil were introduced, whereas a mean arterial pressure 48–52 mmHg was obtained with colloid loading: both urine output and renal markers were within limits. Early values of TnT were 0.250 ng/mL (normal values <0.014 ng/mL), with CPK 850 UI/L (normal values 30–170 UI/L) and CK-MB 31.8 ng/mL (normal values <5.0 ng/mL).
Five hours after TH introduction, a ventricular arrhythmia suddenly developed, evolving into pulseless ventricular tachycardia, requiring resuscitation and DC shock with sinus rhythm restoration. Hyperkalemia (K+8.5 mEq/L) was demonstrated. After electrolyte correction, she required a norepinephrine–dobutamine association, together with further colloid loading to achieve hemodynamic stabilization. Urine output was further enhanced by adding a fenoldopam drip. Two-dimensional echocardiogram assessment revealed right heart enlargement and increased right ventricle pressure (systolic pulmonary artery pressure 50 mmHg). Mechanical ventilation was required until day 6, when a 72-hour nasal CPAP course was introduced. The baby was discharged at 9 days postadmission. Despite early irritative signs on the EEG, the clinical and neurological status was normal, as was the brain MRI performed 1 week later. Early chest imaging of both patients is presented in Figure 1.

Admission chest X-rays.
Discussion
We report two episodes of life-threatening hyperkalemia—one of them associated with a ventricular arrhythmia—occurring during TH application for perinatal asphyxia.
In the literature, neonatal hyperkalemia has been rather related to postischemic oliguria, a well-described event occurring after perinatal asphyxia (Airede et al., 1997; La Rosa et al., 2017). In fact, impaired kidney function leads to a reduction in potassium excretion rate, usually associated with reduced urine production (oliguric/anuric renal failure): the occurrence of severe hyperkalemia in the absence of renal impairment is exceedingly rare (Selewski, 2015).
In contrast, in both cases rhabdomyolysis has been evidenced. The relationship between hypothermia and rhabdomyolysis has been mainly shown in cases of accidental cold exposure (Korantzopoulos, 2003), thus TH can be theoretically a triggering event after hypoperfusion and hypoxia caused by perinatal asphyxia (Lim, 2008); also, in our cases lactate levels possibly witness such a mechanism (Fig. 2).
Given that rhabdomyolysis and myoglobinuria might be a complication of perinatal asphyxia/TH (and rewarming can interrupt its progression, together with an improvement of the global cardiocirculatory performance can interrupt its progression), even if the association of myoglobinuria with perinatal asphyxia and neonatal renal failure has been infrequently described (Kojima et al., 1985), it seems reasonable an easier occurrence of renal failure in asphyxiated infants with rhabdomyolysis/myoglobinuria (Kasik, 1985).
However, to the best of our knowledge, rhabdomyolysis-related hyperkalemia has never been described over the course of multiple controlled investigations on TH in neonatal hypoxic–ischemic encephalopathy, independently on the severity of initial injury (e.g., resuscitation time and cardiorespiratory impairment). Furthermore, we had never recorded before any case of oliguric renal failure among surviving newborns, provided with a timely resuscitation and renal perfusion maintenance, despite the presence of even high levels of rhabdomyolysis and myoglobinuria.
To date, rhabdomyolysis has been rarely reported after controlled hypothermia in adults (Krychtiuk, 2013): in our clinical experience of neonatal TH, we observed CK values up to 10,000 UI/L, in the absence of any hyperkalemia, provided the renal function was maintained. According to literature data (Lackmann, 1991), serum potassium levels in infants with asphyxia can vary. Most authors rather report hypokalemia under TH: in fact, hypothermia produces hypokalemia by inducing a potassium shift from extracellular to intracellular/extravascular spaces (Koht, 1983), with seldom hyperkalemia during rewarming (Sprung, 1990).
Neonatal hyperkalemia and rhabdomyolysis have been otherwise described in the setting of rare metabolic myopathies, such as acyl-CoA dehydrogenase deficits (Korematsu, 2009), whereas in our infants no further metabolic investigations have been performed and metabolic myopathies were later excluded. The 12- and 24-month clinical and motor function follow-up resulted excellent, as neurological developmental stages.
A distinct entity, namely nonoliguric hyperkalemia (NOHK) in which calcium, phosphorus, and glycemic alterations are also present, has been described in premature neonates (Yaseen, 2009), although no reports exist about NOHK in-term or near-term infants undergoing TH.
Until now, the etiology of sudden bloodstream potassium release in individual neonates undergoing TH is unknown, thus a strict surveillance should be kept depending on the extent of rhabdomyolysis and the severity of AKI. At our institution, fenoldopam (Alsabbagh, 2013) drip infusion or i.v. aminophylline (Bhat, 2006; Bhatt, 2019) is currently used, beyond renal perfusion maintenance, to avoid oliguria and further renal damage in asphyxiated newborns undergoing TH.
Footnotes
Authors' Contributions
Individuation of the illustrative cases and study design were carried out by M.P., A.T., L.P., O.G., T.C.M., and G.Z. Data collection and critical literature evaluation were carried out by L.P., T.C.M., C.B., E.P., and G.Z. Text drafting was by L.P. and T.C.M. Revision of the study and evaluation of contents were done by M.P., M.P.D.C., G.D.R., G.C., and D.D.L. Final approval was obtained by M.P., M.P.D.C., G.C., and D.D.L.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.