
Abstract
Perioperative bleeding is a critical challenge in adolescent idiopathic scoliosis (AIS) surgery. Preventing hypothermia is associated with decreased development of coagulopathy, blood transfusion rate in various surgery groups. We hypothesized that blood loss would be reduced in patients who were kept normothermic by implementation of aggressive warming methods in AIS. This randomized-controlled study included patients aged 12–18 years who were scheduled to undergo elective scoliosis deformity correction surgery. The patients were divided into two groups: the study group (Group S) was heated aggressively with three different heaters including compressed-air blower heater, intravenous fluid heating, and a heating bed, while the control group (Group C) received only heating with a standard compressed-air blower heater. Tympanic, esophageal, and axillary body temperatures were measured, and hemoglobin and arterial blood gas analyses were repeated during the anesthesia period. Daily bleeding-coagulation parameters were recorded on postoperative days 0, 1, and 2. Forty-eight patients were randomized, and 39 patients were included into the final analysis. The total amount of intraoperative bleeding (p = 0.027) was significantly lower, and duration of surgery (p = 0.025) and length of hospital stay (p = 0.002) were significantly shorter in Group S. Significant linear relationships were found between the core body temperature and the amount of bleeding (β = 0.0001; p = 0.009), operation time (β = 0.003; p = 0.015), and length of hospital stay (β = 0.027; p = 0.044) with linear logistic regression analysis. We reported that normothermia was preserved in the multiheated group, which diminished blood loss, operation time, and the length of hospital stay. Consequently, we suggested that active heating should be applied in AIS surgeries. ClinicalTrials.gov (NCT04686214).
Introduction
Scoliosis is a three-dimensional vertebral deformity, and adolescent idiopathic scoliosis (AIS) is a common form among pediatric patients (Cheng et al., 2015; Comité Nacional de Adolescencia SAP, 2016). It is diagnosed radiologically, when the Cobb angle exceeds 10° and other causes of scoliosis are excluded (Weinstein, 2019). Curves exceeding 40°–50° require surgical treatment (Gürkan et al., 2013). Perioperative hypothermia is challenging in long-duration surgeries with a high bleeding risk, such as scoliosis surgery (Gürkan et al., 2013). During AIS posterior instrumentation surgery, bleeding of 750–1500 mL is reported (Li et al., 2015).
A body core temperature of 35–35.9°C is considered mild, 34–34.9°C as moderate, and <33.9°C as severe hypothermia (Giuliano and Hendricks, 2017; Ruetzler and Kurz, 2018). Perioperative hypothermia has various causes, including anesthesia-related thermoregulation suppression, direct exposure of body cavities to cold, and administration of cold intravenous fluid (Nieh and Su, 2016). Core body temperature is measured in the esophagus with a probe, or at the tympanic membrane with a thermistor (Ruetzler and Kurz, 2018). Although practical, axillary temperature measurement has low reliability (Sund-Levander and Grodzinsky, 2013). To prevent perioperative hypothermia, passive isolation systems, such as blankets and surgical drapes alone, are insufficient (Sund-Levander and Grodzinsky, 2013; Bindu et al., 2017). Compressed air-blower systems are effective for active heating (Ruetzler and Kurz, 2018). In addition, intravenous fluid warmers are recommended if faster transfusion is planned [>15 mL/(kg·h) in children] (Bindu et al., 2017). Underbody heating beds are used where the trunk is exposed during surgery (Bindu et al., 2017). Although hypothermia reportedly impairs coagulation in in vitro tests, it is controversial whether mild hypothermia increases bleeding (Schmied et al., 1996; Kander and Schött, 2019). Hypothermia may increase coagulopathy (Grant et al., 2009).
The probability of major neurological deficits in spinal deformity correction surgeries is 0.01–0.05% (de Haan and Kalkman, 2001). The combined use of motor-evoked potential (MEP) and somatosensory-evoked potential (SSEP) is fairly successful for detecting neurological damage (Strike et al., 2017; Ferguson et al., 2014). In addition to iatrogenic nerve injury, evoked potentials are affected by physiological variables, including anesthesia and hypothermia effects (Strike et al., 2017). The effect of hypothermia on neuromonitoring has generally been examined in studies in which therapeutic hypothermia and severe hypothermia (<34°C) were applied (Jou et al., 2000; Markand et al., 1990; Madhok et al., 2012; Nevalainen et al., 2017). However, no randomized-controlled study to date has compared the effects of moderate hypothermia in AIS surgery.
The aim of this randomized-controlled study was to compare the effectiveness of heating in AIS surgery. We hypothesized that blood loss would be reduced in patients who were kept normothermic by implementation of aggressive warming methods, compared with a group in which mild–moderate hypothermia was allowed, by using a standard single heater in AIS correction surgery. Second, we hypothesized that, in the mildly hypothermic group, the operation duration, extubation time, intensive care unit stay, and length of hospital stay would be prolonged. Moreover, we hypothesized that, in this group, the amount of drain effluent and the incidence of infection and complications would increase postoperatively, and neuromonitoring values would deteriorate.
Materials and Methods
Patient selection
This prospective, randomized-controlled study was approved by the Istanbul University, Istanbul Faculty of Medicine Ethics Committee (2019/145) . The study was conducted between February and December 2019 at the Department of Orthopedics and Traumatology of the Istanbul Faculty of Medicine. The following patients were included in the study: patients aged 12–18 years who were evaluated as having AIS based on axial skeletal deformity, who were scheduled to undergo elective deformity correction surgery, and who did not have scoliosis due to a secondary cause. We excluded patients with body weight <35 kg; morbid obesity (body mass index >40 kg/m2); known allergy; known bleeding-coagulation disease; use of drugs that affect blood clotting parameters in the previous week; presence of hepatic, renal, hematological, and rheumatological disease and hypertension; a personal or family history of psychiatric disorders, or lack of cooperation. All operations were performed by the same surgeon with 10 years of vertebral surgery experience.
All patients diagnosed with AIS who required posterior instrumentation for deformity surgery under general anesthesia were informed in writing and verbally about the study at least 1 day in advance, and written consent was obtained from the patients as well as their parents. Randomization of consenting patients was performed by means of computer software on the day of operation. The study group was randomly divided into two groups: the study group (Group S) was heated aggressively with three different devices including compressed-air heater, intravenous fluid heating, and a heating bed, while the control group (Group C) received only heating with a standard single compressed-air blower heater. If patients' tympanic or esophageal body temperature measurements fell below 34°C (severe hypothermia) during the intraoperative period, they were excluded from the study.
Anesthesia induction and maintenance
After standard anesthesia monitoring (electrocardiogram, noninvasive arterial blood pressure, oxygen saturation with pulse oximeter, axillary body temperature), all patients received standard general anesthesia induction (0.05 mg/kg intravenous [iv] midazolam, 2 mcg/kg iv fentanyl, 2 mg/kg iv propofol, 0.4 mg/kg rocuronium). After being ventilated for 2 minutes, patients underwent tracheal intubation. A mechanical ventilator was set to a tidal volume of 8 mL/kg, respiratory frequency of 12–18 breaths/min, inspired oxygen fraction (FiO2) of 40%, and positive end-expiratory pressure of 4–5 cmH2O. During the operation, the frequency was adjusted to maintain normocapnia (continuous monitoring EtCO2 30–35 mmHg, partial arterial carbon dioxide pressure 35–45 mmHg with intermittent arterial blood gas [ABG]). If oxygen saturation <95% or partial arterial oxygen pressure <100 mmHg, FiO2 was increased. Invasive arterial pressure, hemodynamic monitoring system, stroke volume variation (SVV) measurements, and central venous catheterization cannulation were applied to the patients. An instant body temperature monitoring probe was used for continuous esophageal temperature monitoring, and a bladder catheter was used to monitor hourly urine output.
Total intravenous anesthesia was provided with propofol and remifentanil infusion for anesthesia maintenance. The dose of propofol was 100–160 mcg/(kg·min) (starting with a high dose and reducing the dose every 10 minutes), and the remifentanil dose was in the range of 0.08–0.25 mcg/(kg·min). Propofol and remifentanil infusion doses were altered to maintain a mean arterial pressure (MAP) between 60 and 65 mmHg, by the controlled hypotension method. After anesthesia induction, tranexamic acid was administered at 10 mg/kg before the surgery after which infusion was continued at 1 mg/(kg·h) throughout the surgery.
The operating room environment temperature was kept at 23°C in both groups. All patients were operated in the prone position. During positioning, supports were placed around the thorax and abdomen, arms were opened to the side, not to exceed 90°C from the body, soft gel supports were placed under the elbows and arms, slight flexion was provided to the hips and knees, and a neutral position of the neck was maintained by placing a mirrored head pillow.
Targeted fluid therapy was applied with balanced crystalloid fluids throughout the operation. If the SVV, which can be continuously monitored by invasive arterial monitoring, was >13%, it was accepted as a volume deficit and 250 mL fluid was loaded and it was re-evaluated. Fluid responsiveness was accepted as a 13% increase in stroke volume after fluid loading. If the SVV was <13%, but the MAP was <60 mmHg, the cardiac index (CI) was evaluated. If the CI was >2.5 L/(min·m2), a vasopressor agent was administered, whereas if the CI was <2.5 L/(min·m2), an inotropic agent was administered. High lactate values in hourly ABG (>2.5 mmol/L) and low central venous oxygen saturation (mixed venous oxygen saturation [SvO2] <70%) were also used as auxiliary parameters in terms of volume deficiency. After the surgery, total intravenous anesthesia infusion was stopped and muscle strength was evaluated by tests, such as clenching the fists, performing a 10 seconds head lift, and tongue movement, and then patients were extubated.
A restrictive transfusion protocol was applied throughout the operation, and 10–15 mL/kg of erythrocyte suspension (ES) was given at values below the 7 g/dL threshold value. The volume of total intraoperative bleeding was calculated from the volume of blood accumulated in the aspirator, minus irrigation fluid, plus the blood volume on the gauze pad, as calculated by weighing the gauze pads on a precision scale.
Neuromonitoring
After prone positioning of the patient, electrodes were placed on the scalp and extremities for MEP and SSEP monitoring. MEP and SSEP values were recorded at baseline and throughout the operation, and were interpreted by a single, nationally certified technician who was present throughout the operation. The amplitude, in milliamps, for MEP and the latency, in milliseconds, for SSEP were recorded. The neuromonitoring values of the upper extremity were considered to evaluate the effect of the surgery, as minimal in the evoked potentials, and the effect of physiological variables, such as anesthetic agents and hypothermia, as maximal (ulnar nerve stimulation for SSEP, biceps muscle response for MEP). At the end of the operation, the first basal MEP and SSEP value, the last of these values, and the arithmetic mean of all these values during the operation were recorded.
We also recorded demographic data, preoperative heart rate, MAP, tympanic body temperature, esophageal body temperature, and axillary body temperature. These parameters were remeasured at 30-minute intervals during the anesthesia period. Hemoglobin (Hgb) and ABG analyses were repeated at 1-hour intervals, and these parameters were recorded throughout surgery. Daily bleeding-coagulation parameters (prothrombin, activated partial thromboplastin time, and international normalized ratio), Hgb, hematocrit, and platelet values, losses from drains, if any, and type and amount of blood product administered, were recorded on postoperative days 0, 1, and 2. The patient's intensive care unit and hospital length of stay, and whether postoperative complications and infection developed, were recorded. We reported asthma, smoking, and obesity as comorbidities.
Statistical analysis
The Number Cruncher Statistical System 2007 (Kaysville, UT) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, and maximum) were used to evaluate the study data. The normality of data distribution was tested using the Shapiro–Wilk test and graphical analysis. Student's t-test was used for comparisons of normally distributed quantitative variables between the two groups, and the Mann–Whitney U-test was used for comparisons of quantitative variables that did not show a normal distribution. Paired-samples t-test was used for within-group comparisons of quantitative variables with a normal distribution. Wilcoxon signed-rank test was used for within-group comparisons of quantitative variables that did not show a normal distribution. Pearson's chi-square test, Fisher's exact test, and the Fisher–Freeman–Halton exact test were used to compare qualitative data. Linear logistic regression analysis was used to assess the correlation of temperature changes with research parameters. Statistical significance was accepted at p < 0.05.
Power and Sample Size Program (P.S version 3.1.2) was used for sample size analysis. With predicted alterations in the amount of bleeding of 20%, at least 34 patients were required to reject the null-hypothesis at a power of 0.8 and α of 0.05. Considering a 10% dropout, at least 38 patients were required.
Results
We initially evaluated 62 patient candidates; 5 of them refused to join the study, and 9 patients did not meet the inclusion criteria. Forty-eight patients were randomized, but 39 patients completed the study and were evaluated in the final analysis (Fig. 1). Demographic data of the patients are demonstrated in Table 1. There were no significant differences in demographic data between the groups (Table 2).
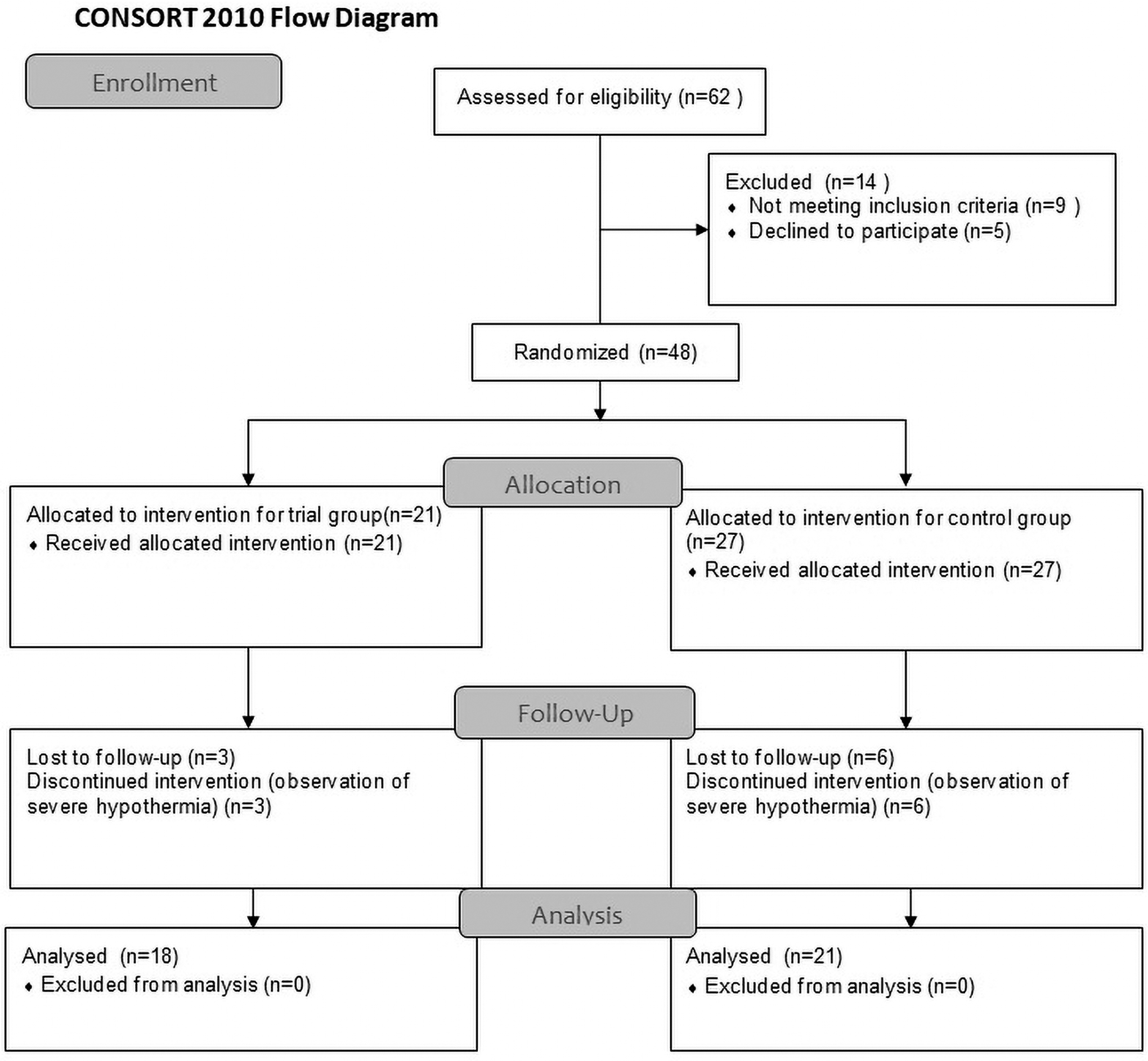
Flow diagram.
Demographic Data
ASA, American Society of Anesthesiologists; BMI, body mass index; Max, maximum; Min, minimum; SD, standard deviation.
Evaluation of Demographic Characteristics by Groups
Student's t-test.
Pearson's chi-square test.
Fisher's exact test.
Surgery data are detailed in Table 3. The duration of surgery in Group S was significantly shorter than that in Group C (p = 0.025) and the total amount of intraoperative bleeding in Group S was significantly lower than that in Group C (p = 0.027). The time between anesthesia termination and extubating was significantly shorter in Group S than in Group C (p = 0.014). The length of hospital stay of the patients was significantly shorter in Group S (p = 0.002). The 48-hour postoperative drain effluent was also significantly less in Group S (p = 0.014) (Table 3).
Evaluation of Data Collected at the End of the Operation and at Discharge According to the Groups
p < 0.05, **p < 0.01.
Student's t-test.
Fisher–Freeman–Halton test.
Mann–Whitney U-test.
Fisher's exact test.
ICU, intensive care unit.
Although there was no significant difference in the intraoperative MAP and heart rate monitoring values between the groups, the mean tympanic, esophageal, and axillary temperatures were significantly higher (p = 0.001 by all three analyses) in Group S (Table 4; Fig. 2).
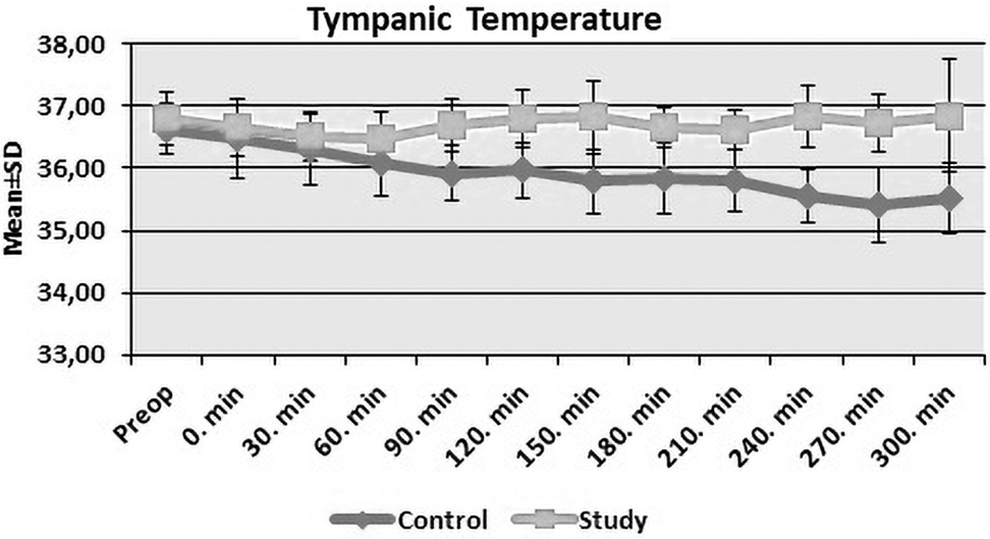
Distribution of tympanic temperature measurements of groups according to time. SD, standard deviation.
Evaluation of Heart Rate, Mean Arterial Pressure, Esophageal Temperature, Axillary Temperature, and Tympanic Temperature Measurements by Groups
p < 0.01.
Student's t-test.
Mann–Whitney U-test.
MAP, mean arterial pressure.
A decrease in the Hgb, hematocrit, and platelet values and an increase in the international normalized ratio (INR) were observed from preoperatively to 48-hour postoperatively, but no significant difference was found between the groups (p = 0.464, p = 0.746, p = 0.725, p = 0.382, respectively). Intraoperative and postoperative ES (p = 0.405, p = 0.215, respectively), crystalloid (p = 0.680), and colloid (p = 0.724) amounts in urine output (p = 0.078) showed no significant difference between the groups. Although a difference was observed in the initial and postoperative pH, Hgb, base excess, and lactate values between the groups, the differences were not statistically significant (p = 0.413, p = 0.800, p = 0.662, p = 0.271, respectively).
There was no significant difference in the baseline, final, and mean neuromonitoring values of the groups (SSEP: p = 0.101, p = 0.213, and p = 0.117, respectively; MEP: p = 0.921, p = 0.778, and p = 0.573, respectively). No significant difference was found between the groups in terms of the presence of 10% latency elongation (p = 0.290) in SSEP and 10%, 30%, or 50% amplitude changes in MEP (p = 0.554).
The correlation of the data obtained in this study with the temperature changes was evaluated by regression analysis. After generating regression models, a statistically significant linear relationship was found between the core body temperature and the mean esophageal (β = −1.143; p = 0.001), axillary (β = −0.52; p = 0.001), and tympanic temperatures (β = −1.144; p = 0.001). In addition, significant relationships were found between the core body temperature and the amount of bleeding (β = 0.0001; p = 0.009), operation time (β = 0.003; p = 0.015), length of hospital stay (β = 0.027; p = 0.044), and extubation times (β = 0.019; p = 0.011) (Table 5).
Linear Regression Analysis
p < 0.05 was considered statistically significant.
CI, confidence interval.
Discussion
In this study, patients in whom normothermia was preserved by using multiple active warming methods during the intraoperative period in AIS surgery and mild–moderate hypothermia were compared. Normothermia was successfully maintained by active warming techniques, and significantly reduced intraoperative bleeding, length of hospital stay, surgery duration, and time to extubation.
Anesthesia-induced hypothermia impairs platelet functions and coagulation enzymes in the coagulation cascade (Rajagopalan et al., 2008). Maintaining perioperative normothermia and preventing intraoperative heat loss are associated with decreased development of infection, coagulopathy, blood transfusion rate, and cardiovascular complications in patients (Kaye et al., 2019). Patients undergoing prolonged major operations are more prone to hypothermia and blood loss than those undergoing minor procedures (Kander and Schött, 2019). Maintaining normothermia in the perioperative period is recommended in the ERAS protocols (Elsarrag et al., 2019). However, since hypothermia may also be neuroprotective, no consensus has been reached regarding the appropriateness of case follow-up for perioperative mild hypothermia (Kaye et al., 2019). No randomized-controlled study has yet compared the effects of moderate hypothermia in AIS surgery (Schmied et al., 1996; Smith et al., 1998; Rajagopalan et al., 2008; Schur et al., 2018).
We reported that normothermia could be achieved at average body temperature values by using multiple active warming methods. In Group S, the intraoperative mean esophagus (p = 0.001), mean tympanic (p = 0.001), and mean axillary temperature (p = 0.001) values were significantly higher than those in Group C. Smith et al. (1998) examined the development of perioperative hypothermia (<36°C) in patients, warming Group S with convective and intravenous fluid heating. The patients in the active heating group were less hypothermic than those heated conventionally, but the mean temperature values remained above 36°C in both groups, with small intergroup differences (Smith et al., 1998). In another study involving orthopedic surgeries, active warming by pressurized air heater and heated intravenous fluid led to significant temperature differences from a conventionally heated group. Unlike in our study, the patients in both groups remained normothermic, as measured at the tympanic membrane and bladder (Winkler et al., 2000).
We found that hypothermia significantly increased bleeding. Similarly, Yi et al. (2018) reported that intraoperative blood loss was less in the group with preserved normothermia (by active heating) than in the group with mild hypothermia in patients undergoing open thoracic or hip replacement surgery. A meta-analysis showed that blood loss increased by 16% (4–26%), even when the temperature decreased intraoperatively by <1°C (mild hypothermia) (Schmied et al., 1996). In pediatric posterior spinal fusion surgery patients, Schur et al. (2018) found no differences in perioperative bleeding between the hypothermia (<35°C) and nonhypothermia groups. They used a retrospective study design and included scoliosis associated with secondary causes, unlike our study. In this study, in which the restrictive transfusion strategy was applied, the amount of intraoperative allogeneic blood transfusion and the number of patients who received transfusion were nonsignificantly higher in Group C. This lack of significance may be related to use of the patient blood management program recommended by guidelines and societies (Goobie et al., 2019).
The length of hospital stay in our normothermic Group S was significantly shorter than that in Group C (β = 0.027; p = 0.044), possibly due to earlier withdrawal of drains and mobilization, because the amount of drain effluent at 48 hours postoperatively was significantly less in Group S (p = 0.014). Wound infection and pneumonia, and electrolyte imbalance and lung expansion defects after 48 hours postoperatively, were similar between groups. A recent study found no difference in the length of intensive care unit stay or hospital stay, and complication developments between intraoperative normothermic and mildly hypothermic patient groups, although they included different types of surgery (Yi et al., 2018).
In our study, deformity correction surgery was performed by the same surgeon. Similar numbers of segments were involved in posterior instrumentation in both groups, but the surgery duration was significantly shorter in the normothermic than hypothermic group (β = 0.003; p = 0.015). Similarly, a retrospective study involving vertebral surgeries investigated the relationship between intraoperative temperature and the amount of total bleeding and reported a strong relationship between bleeding and surgery type and duration (Tedesco et al., 2014). Another retrospective study involving pediatric scoliosis surgery found that surgical time was longer in the normothermic than in the hypothermic group (Schur et al., 2018). The retrospective design and other confounding factors may have influenced their results.
The time between the end of anesthesia and extubation was significantly shorter in Group S than in Group C (β = 0.019; p = 0.011). Kanaya et al. (2017) found that low mean body temperature was a risk factor for prolonged extubation time (p < 0.01).
There was no significant difference in neuromonitoring values between the groups. Previous reports stating that hypothermia caused significant changes in SEPP latency or MEP amplitude values generally involved investigations on therapeutic hypothermia, in which body temperature was reduced to 32–34°C (Madhok et al., 2012; Nevalainen et al., 2017). In an animal study where body temperature was locally reduced to 28°C, an increase in MEP amplitude was observed up to 30°C, due to a neuroprotective effect, but there was no delay in MEP during ischemia (Meylaerts et al., 1999). Therapeutic hypothermia has been studied in neonatal asphyxia: although SSEP prolongation was observed, hypothermia did not decrease SSEP reliability (Nevalainen et al., 2017). A decrease to severe hypothermia (<34°C) in core body temperature values in patients after follow-up being terminated may have caused the differences in MEP and SSEP to be incoherent with the available data.
The study had some limitations. First, the study sample was smaller compared with studies performed in other major surgeries; this is not unexpected, as AIS surgery is not a common operation. Second, this was a single-center study, and each hospital may have different facilities and anesthesia protocols. Third, since the heating devices used in Group S were visible to the anesthesiologists, surgeons, nurses, and staff in the operating room, a double-blind study could not be performed. The last limitation was we did not use a bispectral index monitor or auditory-evoked potentials in electroencephalogram to monitor the depth of anesthesia in patients. Total intravenous anesthesia was provided with propofol and remifentanil infusion without a neuromuscular blocker for anesthesia maintenance. Clinical markers such as detection of the patient's movement with painful stimuli, increase in heart rate and blood pressure were used to assess the depth of anesthesia.
In summary, we found that normothermia was preserved in the multiheated group. This approach reduced blood loss in the perioperative period, shortened the duration of surgery, extubation time, and hospital stay, and reduced the amount of effluent from the drains at 48 hours postoperatively. Consequently, we propose that active heating should be implemented in AIS surgery. Nevertheless, AIS surgery is complex and many different variables can affect the patient. Thus, more randomized trials should be warranted to confirm our results.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.