
Abstract
To investigate the effects of different amounts of lavage fluids on vital signs, inflammatory response, main organ function, and electrolytes on dogs with seawater-immersed open abdominal injury by portable peritoneal lavage device. Twenty dogs were randomly divided into four groups according to different irrigation volume and irrigation time, they were divided into group A (50 mL/min, 1 hour, 3 L), group B (50 mL/min, 1.5 hours, 4.5 L), group C (50 mL/min, 2 hours, 6 L) and group D (50 mL/min, 3 hours, 9 L). Seawater-immersed open abdominal injury dog model was developed and portable peritoneal lavage device was used for lavaging and rewarming. The change of blood pressure, body temperature, heart beat rate, serum tumor necrosis factor-α, interleukin-6, superoxide dismutase, and other indicators of each group were observed before and after immersion, and immediately, 1, 3, and 5 days after lavage. Immediately after lavage, the body temperature, mean arterial pressure, and heart rate of each group gradually recovered to normal, and the recovery rate of group C was faster than that of group A and group B. The indicator of central venous pressure (CVP) continued to decrease immediately after lavaging. CVP in group C was lower than that of groups A and B (p < 0.05, respectively). The inflammatory response was enhanced in all groups after immersion and after lavage, and reached the highest level at 1 day after lavage. The level of interleukin-1β in group C was significantly lower than that in group A (p < 0.05) and no significant difference when compared with other groups on 1 day after lavage. Three days after lavage, all indexes gradually decreased to the level of preinjury. Alanine transaminase (ALT) and lactic dehydrogenase reached the highest level on 1 day after lavage, and the level of ALT in group C was lower than that in group A (p < 0.05). On 1 and 3 days after lavage, the level of Na+ in group C was lower than those in group A (p < 0.05) and no significant difference compared with those in group B and group D. Application of the portable abdominal lavage device with 6 L of lavage fluid (group C) has the best effect of treatment for seawater-immersed open abdominal injury, which can maintain better vital signs and reduce inflammation.
Introduction
With the deepening of human exploration of the ocean, there are more and more injuries in marine operations. A series of problems caused by seawater immersion wounds have been paid more and more attention. When an open abdominal injury is immersed in seawater, it is more likely to cause a decrease in body temperature, blood pressure, and osmotic pressure, making it more difficult to treat than an open abdominal injury. Previous studies (Huang et al., 2010; Zhang et al., 2017) have confirmed that there is significant effect with continuous warm liquid lavage for rewarming, which can improve the pathophysiological disorder after injury and improve treatment success rate.
Previously, we developed a portable peritoneal lavage device (Zhou et al., 2019) and demonstrated that it can be used for the treatment of seawater-immersed open abdominal injury on dogs to achieve the same effect of conventional abdominal lavage rewarming. It can also lavage without interruption for a short period when the rescue team waits for the delivery to hospital, thus we have more time for the delivery and follow-up treatment that meet on-site first aid requirements under naval conditions. In this study, we aimed at exploring the effect of different lavage fluid volumes on the treatment of seawater-immersed open abdominal injury using the portable peritoneal lavage device.
Materials and Methods
The grouping of experimental animals
This study was approved by the animal experiment committee of Xiamen University, and all the dogs were handled according to the Declaration of the National Institutes of Health Guide for Care and Use of Laboratory Animals. Twenty Chinese rural dogs (15–18 kg) were randomly divided into four groups: groups A, B, C, and D according to the amount of lavage fluid (3, 4.5, 6, and 9 L, respectively). To eliminate the influence of biological rhythm on the experimental results, the experiment was started at 8 am and fasting for 24 hours before modeling.
Experimental materials
As previously reported, the portable peritoneal lavage device is composed of three parts: a celiac cover, strap, and fixed bracket (Zhou et al., 2019) (Fig. 1). Artificial seawater was prepared according to the data from the Third Institute of Oceanography of the State Oceanic Administration of China. The main indicators are as follows: infiltration concentration 1250 ± 11.52 mmol/L, pH 8.2, sodium ion concentration 630 ± 5.33 mmol/L, potassium ion concentration 10.88 ± 0.68 mmol/L, chloride ion concentration 658.8 ± 5.25 mmol/L, and temperature 21°C. Laboratory temperature was 25°C. Low-tension lavage fluid contained 4.5% sodium chloride solution and 2.5% glucose solution was configured by the hospital's pharmaceutical factory.
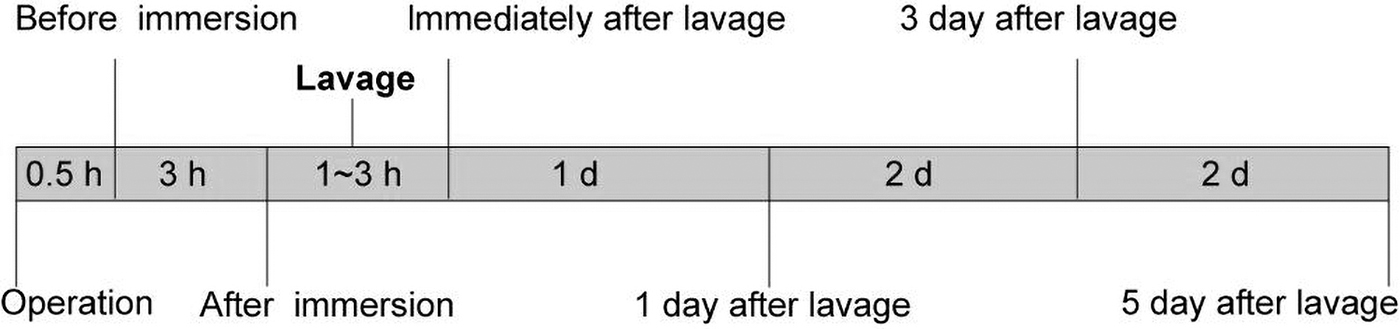
Schedule of the experiment model. Dogs underwent laparotomy to simulate abdominal open injury and then immersed in seawater for 3 hours. Afterward, each group of dogs received lavage using different amounts of fluid accordingly. Vital signs, inflammatory cytokines, major organ function, and other indicators of each group were observed before and after immersion, and immediately, 1, 3, and 5 days after lavage.
Establishment of animal model
Experimental animals were fasted for 24 hours before surgery. Each dog was anesthetized with an intramuscular injection of ketamine according to body weight (20 mg/kg) that was fixed with supine position on a surgical holder. Dogs were all preoperatively catheterized through the femoral artery and femoral vein of the forelimb, and propofol (3 mg/kg/h) was used to maintain anesthesia intraoperatively. Ventral midline incision of 8cm was performed by scalpel to create a surgical abdominal open injury. Dogs were immersed in artificial seawater at 25°C for 3 hours after injury. The immersion surface was over the xiphoid for 5 cm. Three hours later, dogs were pulled up from seawater.
The 3, 4.5, 6, and 9 L low-tension solutions (40°C) were immediately used for lavage through the abdominal wound. The lavage fluid speed was ∼50 mL/min and the corresponding lavage time was ∼1, 1.5, 2, and 3 hours. Specific practice: place the inlet pipe as far as possible into the deep of the abdominal cavity, fasted the celiac cover at the skin around the wound, and then fix it with the strap and fixed bracket. Then the low-tension solution was poured into the peritoneal at uniform speed by gravity through the inlet pipe and into the body of the dog (Fig. 1).
Monitoring of vital signs
All animals were catheterized from the femoral artery and vein, and pressure transducers were connected to an invasive Electrocardiograph monitor, which detects the situation of the heart rate, mean arterial pressure (MAP), and central venous pressure (CVP) at the time before immersion, after immersion, and immediately after lavage. The temperature was measured at the time points already mentioned by inserting the thermometer into the anus.
Serum inflammatory cytokines, electrolytes, and biochemical markers
Blood samples, 5 mL, were drawn at the time before and after immersion, and immediately, 1, 3, and 5 days after lavage. Serum was collected with centrifugation and the levels of tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), interleukin-6 (IL-6), vascular endothelial growth factor (VEGF), malonydialdehyde (MDA), and superoxide dismutase (SOD) in serum were determined by enzyme-linked immunosorbent assay. Visceral function indicator of blood urea nitrogen (BUN), alanine transaminase (ALT), aspartate aminotransferase (AST), lactic dehydrogenase (LDH), and electrolytes indicator of Na+, K+, Ca2+, and Cl− were detected by the clinical laboratory.
Statistical method
Data were analyzed with SPSS 22.0 software and visualized with GraphPad prism 8. All data are presented as mean ± standard deviation (SD). One-way analysis of variance (ANOVA) was used for multiple comparisons. Differences were considered significant at p < 0.05. Data are presented before immersion, after immersion, after lavage, and 1, 3, and 5 days after lavage.
Result
All animals reached the predefined target of open abdominal injury and lavage. There were no differences in blood loss between the groups, and there were no differences among study groups in any of the investigated variables before and after immersion.
Vital signs
The vital sign parameters of dogs are shown in Figure 2. Immediately after lavage, the body temperature, MAP, and heart rate indicators of each group gradually recovered. CVP and MAP increased significantly in group C compared with those in group A and group B (p < 0.05) (Fig. 2A, C), whereas they did not differ in group D.
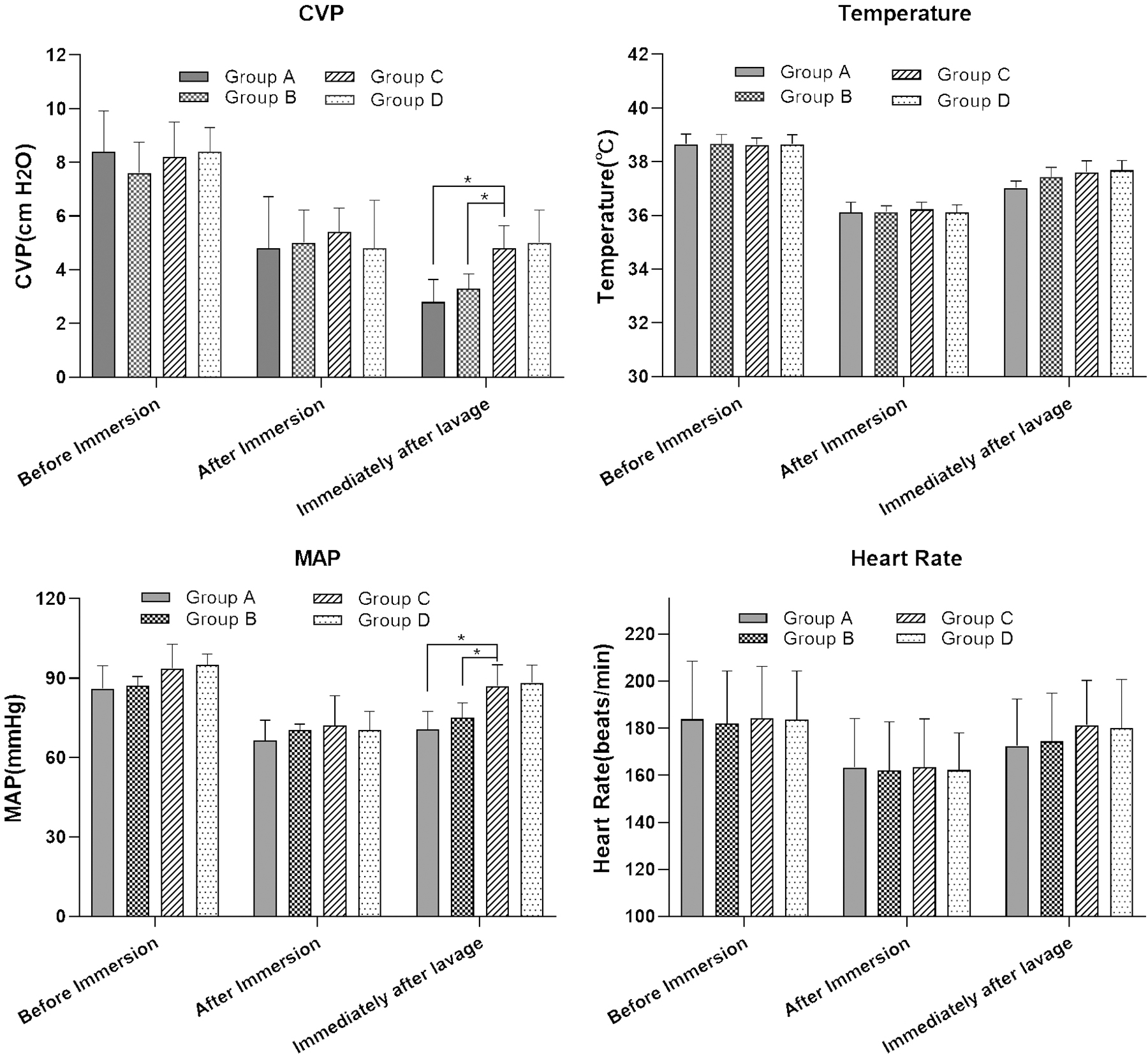
Comparison of the vital signs among different groups. Twenty dogs were randomly divided into group A (50 mL/min, 1 hour, 3 L), group B (50 mL/min, 1.5 hours, 4.5 L), group C (50 mL/min, 2 hours, 6 L), and group D (50 mL/min, 3 hours, 9 L), according to different amounts of lavage fluids. The CVP, MAP, temperature, and heart rate were detected at immediately after lavage. *p < 0.05, compared with group C. CVP, central venous pressure; MAP, mean artery pressure.
Inflammation
The inflammatory response was enhanced in all groups after immersion and after lavage, and reached the highest level at 1 day after lavage (Table 1). The level of IL-1β in group C was significantly higher than that in group A (p = 0.032) and no significant difference when compared with other groups on 1 day after lavage. Three days after lavage, all indexes gradually decreased to the level of preinjury and the IL-1β, and VEGF in group C recovered faster than those in group A and group B (p < 0.05, respectively), but no significant difference compared with that in group D (p > 0.05).
Comparison of Serum Inflammatory Cytokines Indicators of Four Groups of Dogs (n = 5, Mean ± Standard Deviation)
p < 0.05, compared with group C at each time point.
p < 0.05, compared with 1 day after lavage for group C.
IL-1β, interleukin-1β; IL-6, interleukin-6; MDA, malonydialdehyde; SOD, superoxide dismutase; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor.
Major organ function
BUN is an index for evaluation of the function of kidney and liver. It increased after immersion and was the highest immediately after lavage. The level of BUN in group C was significantly lower than those in groups A and B (p < 0.05), and with no significant difference compared with that in group D (p > 0.05) immediately after lavage. After that, the level of BUN recovered to the preinjury state gradually. ALT and LDH reached the highest level on 1 day after lavage. The level of ALT in group C was lower than that in group A (p < 0.05), whereas no significant difference when compared with that in group D (Table 2). There were no differences in AST levels between groups at all time points.
Comparison of Serum Inflammatory Cytokines Indicators of Four Groups of Dogs (n = 5, Mean ± Standard Deviation)
p < 0.05, compared with group C at each time point.
p < 0.05, compared with 1 day after lavage for group C.
ALT, alanine transaminase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; LDH, lactic dehydrogenase.
Electrolyte
Plasma concentrations of Na+, K+, Ca2+, and Cl − were comparable in all groups before immersion, and were increased rapidly after immersion without significant differences among groups (Table 3). After that, they decreased gradually. On 1 and 3 days after lavage, the level of Na+ in group C was lower than that in group A (p < 0.05) and no significant difference compared with that in group B and group D. Similarly, on 1 day after lavage, the levels of K+ and Cl − were significantly lower than those in group A and group B (p < 0.05), whereas with no difference when compared with those in group D (Table 3).
Comparison of Serum Inflammatory Cytokines Indicators of Four Groups of Dogs (n = 5, Mean ± Standard Deviation)
p < 0.05, compared with group C at each time point.
p < 0.05, compared with immediately after lavage for group C.
Discussion
Seawater is a special liquid with high osmosis, alkali, low temperature, and other physical and chemical properties. It contains >20 kinds of pathogenic bacteria that are harmful to the human body. Therefore, seawater-immersed open abdominal injury will cause serious pathophysiological changes different from the injury on land. If the abdominal cavity is immersed in hypertonic seawater, the internal environment will be severely disordered, resulting in the loss of a large amount of extracellular fluid, severe dehydration of the body, a sudden drop in effective blood volume, hemorrhagical shock, and even multiple organ failure (Meng et al., 2004; Cen et al., 2008).
Pathogenic bacteria in seawater can cause inflammation and pressure response in the body, enhance vascular permeability, release various inflammatory mediators and factors, and cause systemic inflammation. At the same time, the affected cells will release various proteolytic enzymes, cytotoxins, and lipolytic enzymes to destroy normal cell structure and cause a series of pathophysiological changes (Wang et al., 2004b; Ma et al., 2017). In addition, with the immersion of low-temperature seawater, the body will lose a lot of heat, which will cause the body's temperature to drop rapidly. Long-term hypothermia can severely inhibit breathing and heart rate, which may cause irreversible damage (Almeida et al., 2016). As a result of these symptoms, the survival rate and success rate of treatment are greatly reduced.
The first task of treating seawater-immersed open abdominal wounds is to pull the patient out of hypertonic seawater at an early stage and perform central rewarming rapidly and effectively. Our research uses continuous lavage with low pressure liquid at 40°C, so that the large blood vessels in the abdominal cavity are directly immersed in warm liquid, and the heat can be directly transferred to various organs and peripheral blood vessels, which is beneficial to restore the deep and peripheral body temperature (Wang et al., 2004a; Cao, 2015).
With the rapid rewarming of the abdominal organs, especially the liver, the activity of enzymes is enhanced, which can accelerate the elimination of acid metabolites and some toxins caused by low temperature seawater (Yuhong et al., 2000). In addition, like peritoneal dialysis, continuous lavage helps eliminate these metabolites and toxins in the body. Therefore, for the seawater-immersed open abdominal injury, simple and effective peritoneal lavage rewarming is the key to treatment.
However, there is usually only basic medical equipment in marine operations, and rescue teams cannot treat patients systematically and comprehensively. Our research team designed and developed a portable abdominal lavage device that is suitable for offshore operations (Zhou et al., 2019). Previous study has proved that the device can perform early and rapid peritoneal lavage and rewarming, effectively stabilize vital signs and correct electrolyte disorders, and play a role in reducing inflammation and shock. In this way, we have more time for delivery and follow-up treatment, thereby increasing the success rate of treatment.
Continuous peritoneal lavage has a significant effect on central rewarming, but how to control the amount of lavage fluid and lavage time is worthy of attention. In other words, at a certain lavage speed, the lavage time is particularly important. If the amount of lavage fluid is insufficient, the effect of early treatment will not be obtained due to the lack of rewarming time, which will reduce the success rate of treatment. In contrast, because we use low-tension or low-permeability liquids for lavage, if the lavage time is too long, water will gradually transfer from the external fluid to the cells, which will cause normal tissue cells to edema and cause internal environmental disturbances.
Furthermore, the cavity of the intestines contains a large number of resident bacteria such as Escherichia coli, Enterococcus, and anaerobic bacterium. These bacteria participate in the body's metabolism, immune regulation, and biological antagonism that play an important role in body ecological balance. After open abdominal injury and seawater immersion, animals suffer two severe injuries in a short period of time, resulting in impaired intestinal barrier function and increased intestinal mucosal cell permeability, leading to the migration of a large number of intestinal bacteria to the parenteral tissues (Han et al., 2009).
Prolonged lavage may result in more severe bacterial displacement, which will lead to microecological imbalance in the abdominal cavity and intestinal tract, even the double infection. Excessive lavage will continue to increase the pressure in the abdominal cavity, which not only affects blood circulation but also damages the breathing of the diaphragm. In addition, long-term use of low-tension liquid at 40°C for rewarming will cause the peripheral blood vessels of the abdominal cavity to dilate and reduce the blood returning to the heart, which will lead to a drop in blood pressure.
Therefore, the rewarming with the appropriate amount of lavage fluid can effectively correct the body pathophysiological changes and achieve the effect of early treatment. In this study, four groups with the amount of 3, 4.5, 6, and 9 L gradient liquid were used for lavage. The results showed that as the volume of lavage fluid increased, the recovery of body temperature, vital signs, electrolytes, and visceral function was improved, and the inflammatory factors returned to normal faster. The time for lavage and rewarming with 6 L of liquid is ∼2 hours, and the effect is significant. Further increase of lavage fluid will not significantly change the effect of lavage.
In summary, we use a portable abdominal lavage device to perform lavage with a gradient amount of low-tension liquid. The results showed that the use of 6 L of low-tension liquid lavage had the best warming effect, and the recovery of vital signs, electrolytes, visceral function, and inflammatory factors was better than in the other groups. However, due to the small number of groups, further experiments should be conducted on the optimal amount of lavage fluid.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the medical research grants from Nanjing Military Region of People's Liberation Army [Grant No. ZX21] and Natural Science Foundation of Fujian Province [Grant No. 2020J01133].