
Abstract
In acute myocardial infarction (AMI), myocardial reperfusion injury may undo part of the recovery after revascularization of the occluded coronary artery. Selective intracoronary hypothermia is a novel method aimed at reducing myocardial reperfusion injury, but its presumed protective effects in AMI still await further elucidation. This proof-of-concept study assesses the potential protective effects of selective intracoronary hypothermia in an ex-vivo, isolated beating heart model of AMI. In four isolated Langendorff perfused beating pig hearts, an anterior wall myocardial infarction was created by inflating a balloon in the mid segment of the left anterior descending (LAD) artery. After one hour, two hearts were treated with selective intracoronary hypothermia followed by normal reperfusion (cooled hearts). In the other two hearts, the balloon was deflated after one hour, allowing normal reperfusion (control hearts). Biopsies for histologic and electron microscopic evaluation were taken from the myocardium at risk at different time points: before occlusion (t = BO); 5 minutes before reperfusion (t = BR); and 10 minutes after reperfusion (t = AR). Electron microscopic analysis was performed to evaluate the condition of the mitochondria. Histological analyses included evaluation of sarcomeric collapse and intramyocardial hematoma. Electron microscopic analysis revealed intact mitochondria in the hypothermia treated hearts compared to the control hearts where mitochondria were more frequently damaged. No differences in the prespecified histological parameters were observed between cooled and control hearts at t = AR. In the isolated beating porcine heart model of AMI, reperfusion was associated with additional myocardial injury beyond ischemic injury. Selective intracoronary hypothermia preserved mitochondrial integrity compared to nontreated controls.
Introduction
In ST-elevation myocardial infarction (STEMI), primary percutaneous coronary intervention (PCI) is the preferred revascularization strategy in current guidelines to restore blood flow to the ischemic myocardium and to limit infarct size (IS) (O'Gara et al., 2013). Consequently, this decrease of IS translates to a decrease in the risk of complications, such as heart failure and mortality (Stone et al., 2016). Paradoxically, reperfusion itself can also have harmful effects and cause additional damage to cardiomyocytes that were still viable immediately before reperfusion. This so-called “myocardial reperfusion injury” diminishes the beneficial effects of early revascularization, consequently increasing IS (Yellon and Hausenloy, 2007).
Myocardial reperfusion injury is still not completely understood, resulting from the inability to assess biochemical processes and ultrastructural changes in-vivo that occur during transition from ischemia to reperfusion. Importantly, this understanding is essential for the development of an effective therapy for myocardial reperfusion injury, which currently still does not exist for humans.
Hypothermia proved to be effective to decrease IS in preclinical studies (Miki et al., 1998). Unfortunately, these promising results could not be reproduced in randomized controlled trials in patients with STEMI (El Farissi et al., 2021a). Reasons for this failure of systemic hypothermia in human trials are well recognized (El Farissi et al., 2021b). Therefore, in the new era of hypothermia treatment for STEMI patients, new methods using therapeutic hypothermia should be explored. In these methods, hypothermia should be provided either locally, for example, directed to the affected organ and personalized, for example, only provided in selected patient categories that most likely will benefit from hypothermia.
Recently, a new cooling method termed selective intracoronary hypothermia has been developed, and tailor-made to use during primary PCI in patients with STEMI (Otterspoor et al., 2017). It overcomes many important limitations of systemic hypothermia. Currently, this method is being investigated in a European, multicenter, randomized controlled, proof-of-principle study in patients with anterior wall STEMI (NCT03447834) (El Farissi et al., 2021c). A predefined safety analysis of the EURO-ICE trial suggested that this technique can be implemented within the routine of primary PCI without safety concerns in patients with anterior STEMI (El Farissi et al., 2021c).
In this proof-of-concept study, we explored the early (ultra)structural changes underlying myocardial reperfusion injury and the potential protective effects of hypothermia in the isolated beating porcine heart.
Methods
Heart acquisition, preparation, and instrumentation
Four hearts of Dutch Landrace pigs (n = 4), slaughtered for regular human consumption, were obtained to perform ex vivo beating heart biosimulation experiments. The harvesting and preparation of the hearts have previously been described (de Hart et al., 2011). The protocols of the slaughterhouse and laboratory were developed in accordance with EC regulations 1069/2009 regarding the use of slaughterhouse animal material for diagnosis and research, supervised by the Dutch Ministry of Agriculture, Nature and Food Quality and approved by the associated legal authorities of animal welfare (Food and Consumer Product Safety Authority). No additional IRB approval was required according to legislation.
A Judkins Right 6 Fr guiding catheter was fixated in the ostium of the left coronary artery. In addition, a pressure/temperature wire (PressureWire X™; Abbott, Minneapolis, MN) was advanced into the distal left anterior descending (LAD) artery. By using this PressureWire X, a designated monorail balloon-infusion catheter (CoolCell®; Hexacath, Paris, France) was advanced to the mid LAD artery.
After preparation, the hearts were connected to the ex vivo biosimulator platform (PhysioHeart™; LifeTec Group, Eindhoven, The Netherlands) to reinstate coronary perfusion with heparinized, and oxygenated 38°C blood, after which spontaneous contraction started. Hearts were stabilized for at least 15 minutes to obtain sinus rhythm. To assess the quality of the preparations, the system was switched to working mode to determine cardiac output, after which it was switched back to Langendorff mode for the experiment (de Hart et al., 2011).
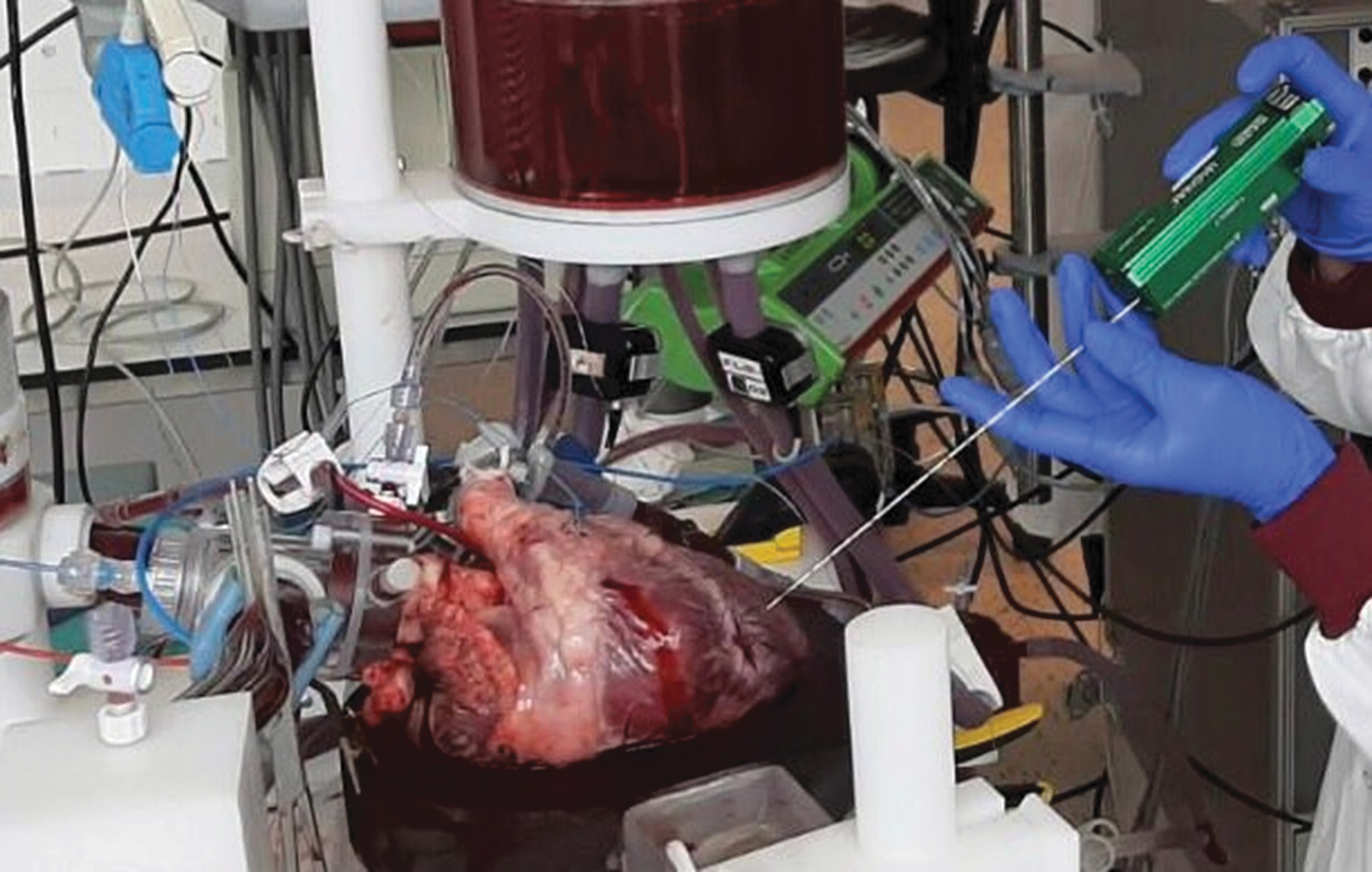
The CoolCell catheter was positioned in the LAD artery distal to the first diagonal branch (Fig. 1). Optimal positioning of the CoolCell was confirmed by brief inflation of the balloon while assessing the cyanotic discoloration of the apical-anterior wall. This was further confirmed by infrared camera visualization. In the corresponding myocardium, the myocardium at risk (MaR), thermistors were placed in the proximal, mid, and distal part to monitor myocardial temperature.

Schematic overview of experiment with selective intracoronary hypothermia. A pressure-temperature wire, after connecting it to the Coroventis software, is placed in the distal LAD artery. The CoolCell® catheter is advanced over this pressure-temperature wire and positioned in the mid LAD. The CoolCell catheter is connected to infusion pumps filled with saline. Both the distal coronary pressure (green curve on Coroventis screen) and distal coronary temperature (blue curve on Coroventis screen) are continuously recorded. Inflation of the balloon makes it uniquely possible to induce hypothermia before reperfusion occurs. LAD, left anterior descending.
Experiment
An anterior wall myocardial infarction was created by occluding the mid LAD artery for 1 hour in the Langendorff perfused pig hearts (Fig. 2).

Timeline of experiments. An anterior wall myocardial infaraction was created by inflating a balloon in the mid LAD artery for the duration of 1 hour. Biopsies were taken at onset of the experiment (t = BO), just before reperfusion (t = BR) and after reperfusion (t = AR), indicated by the black arrows.
After 1 hour, selective intracoronary hypothermia was applied in 2 hearts (cooled hearts) as previously described (Otterspoor et al., 2017). First, saline at room temperature was infused through the infusion lumen of the CoolCell catheter into the distal LAD to cool off the MaR for a duration of 7 minutes while the balloon was still inflated, that is, before reperfusion. This cooling phase is called the “occlusion phase”. Thereafter, the balloon was deflated and infusion was then continued with “cold” saline at 4°C for 10 more minutes. This second cooling phase is termed the “reperfusion phase” (Fig. 1). During this phase, 4°C saline was used to compensate for the mixing with warm blood flow. After the cooling procedure, normal reperfusion was continued for 10 minutes, after which the hearts were terminated.
In the other 2 hearts, the balloon was deflated after 1 hour, allowing normal reperfusion with 38°C blood for 10 minutes without any additional treatment (control hearts). After 10 minutes, the hearts were terminated.
Due to the extra time needed for the occlusion phase (± 7 minutes), the ischemic time in the cooled hearts is 1 hour and 7 minutes in comparison to an ischemic time of 1 hour in the control hearts, respectively.
During these experiments, biopsies were taken at set time points, using the Bard® Magnum® Biopsy System and 18 Gauge caliber needles size with needle length of 20 cm. Penetration depth was set to 22 mm (Fig. 3). At each time point, biopsies were taken from the MaR and from the remote area (RA, left ventricular posterior wall) (Fig. 2). Biopsies were taken before occlusion (t = BO), 5 minutes before reperfusion (t = BR), and 10 minutes after reperfusion (t = AR).
Biopsies are taken during the experiment, using the Bard® Magnum® Biopsy System and 18 Gauge caliber needles size.
At the end of the experiment, the hearts were terminated in Langendorff mode by injecting a 10 mL bolus of KCl solution (1 mmol/mL) in the blood supply line. Directly after contractility stopped, the Langendorff perfusion was ended. Hereafter, the hearts were disconnected from the setup and a strip of tissue of the myocardial wall from both the MaR and the RA was isolated for further analysis.
Tissue weight
Edema assessment
At termination (t = AR), samples have been collected to quantify edema. Samples have been weighted fresh in Eppendorf tubes and quickly snap frozen in liquid nitrogen. Subsequently the vials are placed into the lyophilizer (Labconco) for water removal. The day after, the desiccated samples have been reweighed. The difference between the wet sample weight and after lyophilization has been plotted as a measure of the amount of fluid present in the sample, and as indirect indication of edema.
Electron microscopy
Biopsies were obtained from the MaR and RA, fixed in 4% formaldehyde +2% glutaraldehyde in 0.1 M sodium cacodylate buffer, pH 7.4 O/N at 4°C. The biopsies were rinsed and stored in 0.1 M Sodium Cacodylate buffer, pH 7.4 at 4°C until further processing. Postfixation was performed with 1% OsO4 0.1 M phosphate buffer, pH 7.4 for 2 hours. Samples were then dehydrated in a series of acetone and embedded in Epon (SERVA). Ultrathin sections were cut (Leica Ultracut UCT), collected on formvar and carbon-coated grids for transmission electron microscopy (TEM), and stained with uranyl acetate and lead citrate (Leica AC20).
Micrographs were collected on a JEOL1010 TEM equipped with a Veleta 2k × 2k CCD camera (EMSIS, Munster, Germany) or on a Tecnai12 (FEI/Thermo Fisher Scientific) equipped with a Veleta 2k × 2k CCD camera (EMSIS) and operating SerialEM software. A qualitative assessment of mitochondrial structure, lysosomes, and lipid droplets was performed. Results are presented in a descriptive manner.
Immunostaining
Biopsies were fixed overnight in 4% buffered formalin, processed, and subsequently embedded in paraffin to prepare sections with a thickness of 5 μm. Sections at different depth have been collected from each sample: at t = AR, three serial sections at 150 μm distance were collected per glass, for the other biopsies (t = BO and T = BR) five serial sections at 100 μm distance.
After deparaffinization, antigen retrieval was performed, depending on the used primary antibody (Table 1). For heat-mediated antigen retrieval, the tissue slides were heated in a 97°C water bath for 30 minutes in citrate buffer (0.01 M Trisodium citrate, pH 6) or TRIS-EDTA buffer (Tris 9.9 mM, EDTA 1 M, pH 9.0). After heating, slides were slowly cooled down to room temperature (30 minutes). Nonspecific binding was blocked by 5% bovine serum albumin (BSA; Roche) in PBS/0.1% Tween-20 (Sigma) for 40 minutes at room temperature. Primary antibodies were prepared in the optimized concentrations (Table 1) in 1:5 diluted blocking solution. Tissue slides were incubated overnight at 4°C and thereafter washed with PBS/0.1% Tween-20. The secondary antibodies were diluted 1:250 in PBS/0.1% Tween-20 and applied as shown in Table 1.
Preparation of the Primary Antibodies
After 1.5 hours of incubation at room temperature the sections were washed with PBS/0.1% Tween-20 two times for 5 minutes and rinsed in PBS for other 5 minutes. For counterstaining of cells, DAPI (SIGMA) diluted 1:1000 in PBS/0.1% Tween-20 was applied for 10 minutes. Sections were rinsed two times in PBS for 5 minutes and mounted in Mowiol 4–88 (SIGMA). Negative controls were generated with the same procedure omitting the primary antibody during the first incubation.
Histology
Tissue slides were deparaffinized in xylene and rehydrated in a graded series of ethanol. Mayer's Hematoxylin (Sigma) and aqueous Eosin Y (Sigma) staining was performed to determine tissue morphology. Sirius Red (Sigma) staining was performed to identify collagen distribution in our samples as follows: the rehydrated slides were immersed for 1 hour in 0.1% picrosirius red solution (0.1% Direct Red 80, SIGMA dissolved in saturated aqueous 1.3% picric acid; Sigma), washed in 0.1% acidified water for 1 minute following another 1 minute wash in 0.5% acidified water. Sections are then dehydrated with a series of alcohol and mounted in Entellan (Sigma).
Image acquisition
Image acquisition of H&E and Picrosirius Red was performed with the Zeiss Axio Observer Z1 using 20 × magnification. Twenty images per slide were acquired randomly from the biopsy samples (T0, T55) and 21 images per slide were obtained randomly from the large tissue samples (T70). For fluorescent staining image acquisition was performed with the Zeiss Axiovert 200 M, at 14-bit depth: 15 images per slide were randomly acquired for all samples at 32 × magnification.
Image analysis
Hematoma assessment
Pictures of H&E-stained samples were taken and qualitatively assessed for signs of hematoma by four blinded observers. Images were ranked into four categories: 0 – No visible hematoma: none or only several blood cells (outside blood vessels) 1 – Low: small number of blood cells (above low tens), or slightly higher count but very spread out. Still most interstitial area free of erythrocytes, 2 – Medium: all images that do not clearly belong to other categories, 3 – High: very large aggregates of erythrocytes relative to tissue area (>20% by eye) and/or most interstitial space filled with erythrocytes.
Endothelial injury of the microvasculature
Vascular endothelial injury was assessed in αSMA/CD31 stained samples by quantifying the percentage of vessels that are CD31 negative vessels but αSMA positive.
Interstitial space analysis
Macro-based semiautomated analysis using ImageJ was implemented to quantify collagen deposition as a percentage of the total surface of tissue within the image. This method was based on the method used by Hadi et al. (2011) and had been optimized for our purposes.
Sarcomeric damage
Absence of cross striations to evaluate sarcomeric injury was assessed semiquantitatively using cTnI immunohistochemistry. Scoring on a scale of 0–3 was performed by 3 independent observers, in which healthy tissue with 80–100% cross striations in the myocardium was scored as 0. A grade of 1 indicates 60–80% healthy cross-striations, grade 2 marks 40–60%, healthy striations, and finally grade 3 represents the mostly damaged tissue with <40% healthy cross-striations.
Intercalated disc remodeling
Connexin 43 (Cx43) immunofluorescence was analyzed as an indication for tissue damage. In addition to mediating cell-cell electrical coupling, Cx43 is also a gap junction protein that is important in tissue repair and ventricular remodeling after MI. Cross section images were selected manually before being processed and binarized using a semiautomated self-developed script in MATLAB to detect and measure the ellipses of intercalated discs using the Cx43 marker. As a result of cardiac injury, redistribution of Cx43 to the intercalated discs on the lateral sides of the cardiomyocytes, results in a reduction of the aspect ratio of the ellipse, closer to a circular aspect ratio of 1. To validate script methodology, a subset of the images was manually analyzed by four independent observers
Early monocyte/macrophage infiltration
Percentage of CD64-positive cells in the myocardium was used to detect monocyte/macrophage infiltration. Macrophages play a critical role in homeostatic maintenance of the myocardium and recovery of tissue after injury, both in the absence and presence of reperfusion (Yonggang et al., 2018).
Results
Experimental setup
Mean total preexperiment ischemic time between acquisition and reperfusion was 2 hours and 29 minutes (Table 2). Duration of warm ischemia was 3 minutes in all hearts and duration of cold ischemia 2 hours 17 minutes to 2 hours and 35 minutes. Cardiac output in working mode ranged from 2.25 L/min to 9.5 L/min. Coronary blood flow in Langendorff mode was 0.85–1.1 L/min.
Baseline Characteristics
Defined by the time from slaughter to administration of cardioplegia.
Defined by the time between cardioplegia and onset of Langendorff perfusion.
Selective intracoronary hypothermia
Duration of the occlusion phase lasted 6–8 minutes and coronary temperature decreased by 6–9°C compared to baseline during this phase (Fig. 4). The distal coronary pressure (distal to the inflated CoolCell catheter) increased by 30 mmHg after start of infusion of saline.
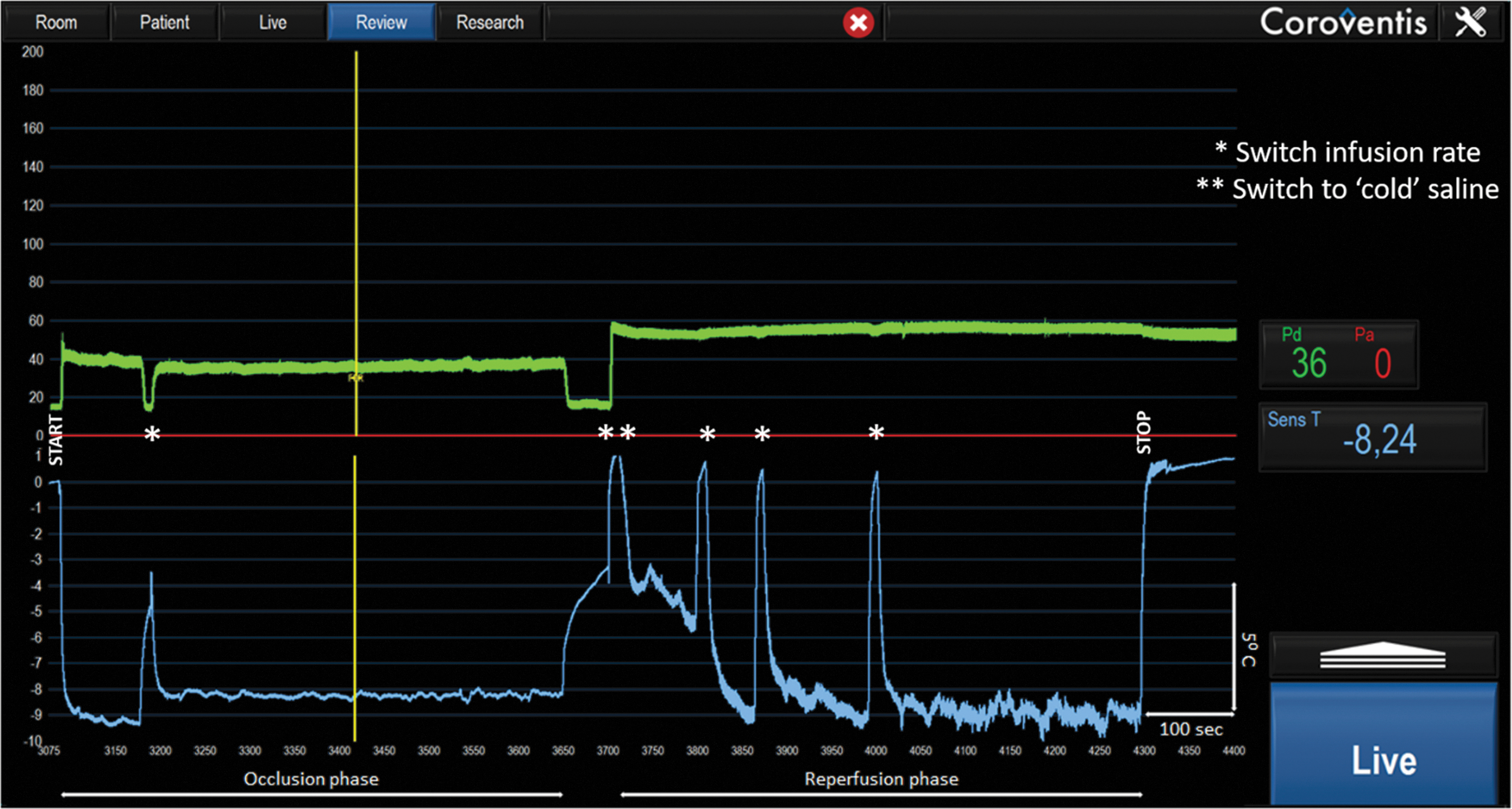
Coroventis recording of a Langendorff perfused pig heart during treatment with selective intracoronary hypothermia. The aortic pressure (Pa, red) is lacking in this model (due to the Langendorff setup of the experiment) and shown here as a flat line. The distal coronary pressure (Pd, green) and distal intracoronary temperature (Sens T, blue) are shown. Notice that the Pd is higher during the reperfusion phase because the balloon is deflated.
During the reperfusion phase, distal coronary temperature decreased by 4– 10°C compared to baseline and this phase lasted 8–10 minutes. Total infused saline ranged from 210 mL to 288 mL.
Ischemic injury—electron microscopy
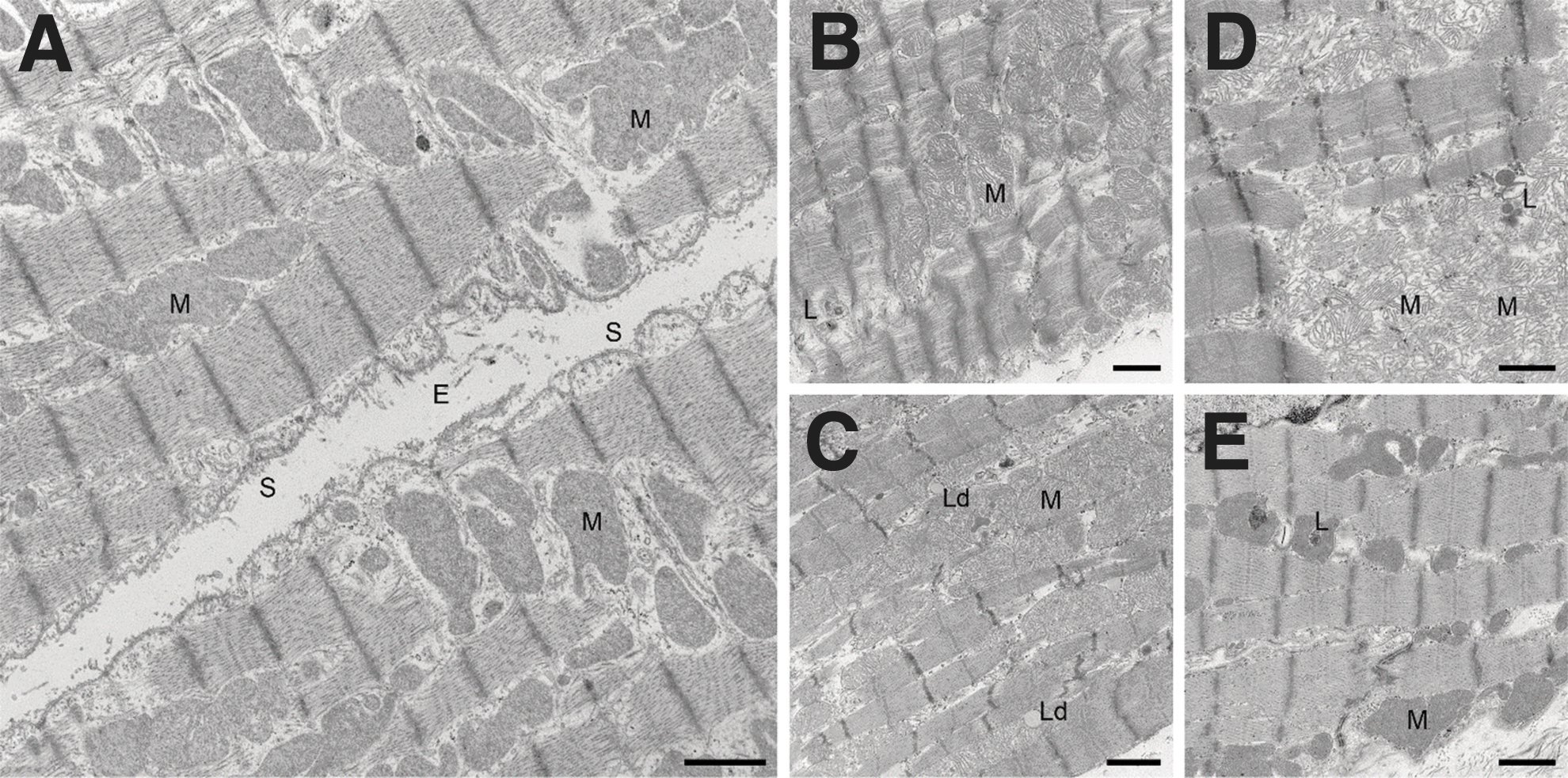
EM analysis of the control tissue showed normal organization of muscle tissue with dense mitochondria (M) and an intact sarcolemma (S) (Fig. 5A). After ischemia no apparent differences could be observed between the control (Fig. 5B) and cooled (Fig. 5C) hearts. In both conditions mitochondria were slightly swollen with more loosely arranged cristae and the sarcolemma was disrupted at several places with more debris present in the endomysium. In the RA, no difference was observed at t-BR compared to t = BO.
Electron microscopic view at t = BO
Ischemic injury—histology
Histological analysis of the myocardial tissue at t = BR demonstrated features typically associated with early ischemic injury, in particular, contraction band necrosis (Fig. 6A). In addition, we observed vascular endothelial injury with interstitial hemorrhage (Fig. 6D, E). As expected, no difference was observed between the control and cooled hearts.
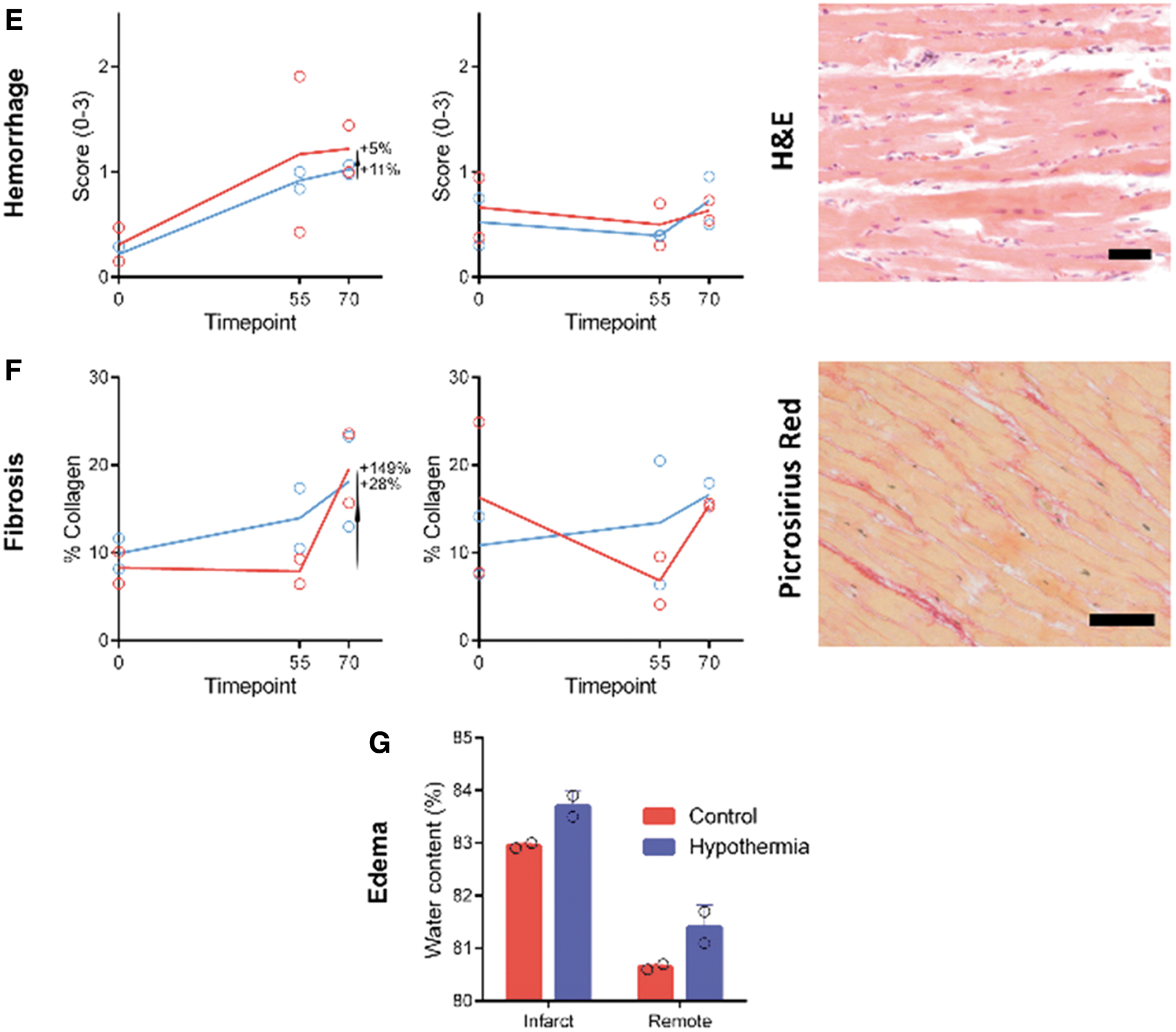
Histological examination at t = BO, t = BR and t = AR of the MaR in the cooled and control hearts. Histological analysis and representative tissue sections include sarcomeric collapse
Reperfusion injury—electron microscopy
At t = AR, a clear difference in the morphology between the hypothermia-treated hearts and control hearts was observed (Fig. 5D, E). In control hearts, mitochondria were frequently and extensively damaged (Fig. 5D), whereas mitochondria in the hypothermia-treated hearts had remained intact (Fig. 5E). Overall, the control hearts showed more tissue shrinkage, extensive disruption of the sarcolemma at several places and debris in the endomysium. In both control and hypothermia treated hearts, sometimes lipid droplets were observed in between the muscle fibers in close relationship with mitochondria.
Reperfusion injury—histology
Microscopically, hypothermic reperfusion had no detectable effect on reperfusion injury. Histologic evaluation revealed a consistent increase in sarcomeric injury, leading to a substantial loss of healthy cross-striations after reperfusion in both treatment groups (Fig. 6A). Vascular endothelial injury gradually increased after ischemia as the number of CD31-positive vessels decreased. However, selective intracoronary hypothermia halted this progression of endothelial injury in comparison to the control hearts (Fig. 6D). Vascular damage was further confirmed by the presence of loose erythrocytes in the cardiac interstitial space (Fig. 6E). A decrease of edema could not be confirmed as the myocardial water content did not differ between cooled and control hearts, 83.0% ± 0.0% versus 83.7% ± 0.2%, respectively (Fig. 6G).
As shown in Figure 6F, reperfusion injury considerably increased collagen accumulation in both groups. Collapse of the extracellular matrix due to cardiomyocyte death may result in patchy fibrosis, as production of new matrix proteins takes longer than the 10 min time window used in this study. On the contrary, no increase in fibronectin was detected in either group (data not shown).
Discussion
This present proof-of-concept study sought to explore the protective effects of selective intracoronary hypothermia on various mechanisms involved in myocardial reperfusion injury to further optimize TH for STEMI patients. Since all systemic methods have failed, TH research should be directed at exploring local hypothermia methods. Therefore, basic research using local hypothermia elucidating responsible cellular mechanisms is mandatory.
The existence of myocardial reperfusion injury has been questioned since it was first described in 1960 (Jennings et al., 1960). The uncertainty of this existence relates to the inability to accurately investigate the progression of injury during the transition from myocardial ischemia to reperfusion. This uncertainty is reinforced by the hitherto lack of an effective treatment for myocardial reperfusion injury (Yellon and Hausenloy, 2007). Using the ex vivo isolated beating heart model, tissue analyses could now be performed both before and after reperfusion. To the best of our knowledge, this is the first study where this was done. This makes it possible to truly discriminate ischemic injury from reperfusion injury.
Myocardial reperfusion injury and recovery take place at different length scales (nm-cm) and at different time scales (minutes-hours). In this study short intervals after reperfusion (10 minutes) were used to evaluate the initial mechanisms and effect of hypothermia. Necessarily, we analyzed the tissue at various lengths scales using a range of technologies covering ultrastructural to structural markers of key cardiac functions.
Indeed, as previously has been described, additional (myocardial reperfusion) injury beyond ischemic injury arises after reperfusion (Yellon and Hausenloy, 2007). This effect could be demonstrated both by electron microscopy and histology as shown in Figures 5 and 6.
The key finding in this study was that mitochondria were better preserved after application of hypothermia compared to control hearts, as demonstrated by electron microscopic analyses (Fig. 5D, E). Except for a possible protective effect on endothelial injury, no other differences could be demonstrated with histology. The contradiction in these data may be related to the timeline of the experimental setup. Structural changes of the myocardium in the reperfusion phase take time to occur and to observe a clear effect, longer timer intervals after reperfusion should be used.
We hypothesize that, in the first minutes after reperfusion, the protective effects of selective intracoronary hypothermia are only visible at the ultrastructural level, for example, mitochondria, while protection on a histological level merely can be observed using longer time intervals. This is even more true for a macroscopic evaluation. Therefore, in human patients, considerable time (months) is necessary between index procedure and performing cardiac imaging to evaluate a possible effect on left ventricular function (Ibanez et al., 2019).
This proof-of-concept study is the first to assess the effects of selective intracoronary hypothermia on myocardial reperfusion injury, evaluated by electron microscopy and histology. Kim et al. (2005) and Otake et al. (2007) reported successful application of catheter-based hypothermia in acute myocardial infarction (AMI), but analyses on histology or cell structure were not performed. On the contrary, Ferrari et al. (1990) demonstrated a protective effect of hypothermia on mitochondrial respiratory function in isolated rabbits' hearts in relationship to cardioplegia. In this proof-of-concept study, the protective effect of hypothermia in the context of AMI was demonstrated by structural preservation of mitochondria with TEM.
Most other studies on other hypothermia for cardioprotection in AMI did not use the ex vivo beating heart biosimulation but used in vivo experiment within different species. As a result, in these live animal experiments ischemic injury could not be distinguished from reperfusion injury and the contribution of both entities to the total injury remains unclear. Furthermore, these studies mainly looked at IS reduction (Miki et al., 1998; Götberg et al., 2008; Hale et al., 2013) or focused on other aspects of reperfusion injury such as the no-reflow phenomenon (Götberg et al., 2008; Hale et al., 2013) or assessed the protective effect on other endpoints, such as energy preservation (Simkhovich et al., 2004) and cell survival proteins (Ning et al., 1998).
Limitations
This study is a proof-of concept study. The findings can only be seen as hypothesis generating.
First, only four beating porcine hearts were included in this study. To compensate for this small sample size, analyses were performed by multiple blinded reviewers. Second, while these isolated beating porcine hearts serve as a sophisticated alternative to classical in vivo animal studies, the results cannot simply be extrapolated to in vivo tests in animals or humans with AMI. Not all physiologic feedback mechanisms are present in the isolated heart and unknown variables may play a role. However, the use of isolated beating porcine hearts facilitates in taking biopsies before and after reperfusion to investigate the differences, which is not possible in classical animal experiments. Third, as biopsies are taken from the same heart during the complete experiment, there is a chance of selection bias as only a small portion of the heart is investigated and not the entire myocardium.
Conclusion
In a model of AMI in isolated beating porcine hearts, an increase of myocardial damage is observed immediately after reperfusion on histological evaluation, confirming existence of myocardial reperfusion injury. Selective intracoronary hypothermia, as a cardioprotective therapy for myocardial reperfusion injury, seems to preserve mitochondrial integrity.
Footnotes
Acknowledgment
The Eindhoven Center for Multiscale Electron Microscopy (CMEM of Eindhoven University of Technology) is acknowledged for their support in tissue preservation for electron microscopy analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The electron microscopy infrastructure used for this work is partially financed by the research program National Roadmap for Large-Scale Research Infrastructure (NEMI; project number 184.034.014 to J.K.), which is financed by the Dutch Research Council (NWO).