
Abstract
Cryotherapy is used in individuals in the postoperative period (PO) of anterior cruciate ligament (ACL) repair, owing to its effects such as increased pain threshold, decreased cellular activity, and vasoconstriction. The aim of this study was to analyze the effect of cryotherapy on pain intensity in the immediate PO of ACL reconstruction. A scoping review was performed in the databases: Cochrane, Embase, Lilacs, LIVIVO, PEDro, PubMed, Scopus, and Web of Science; and gray literature: Google Scholar, CAPES Thesis Database, and Open Grey. PRISMA recommendation was followed. Two blinded reviewers performed the selection of studies: Phase 1—reading of titles and abstracts and Phase 2—Reading of the full texts and disagreements resolved in consensus. The references of 701 studies were identified, 603 from the main databases and 98 from the gray literature. After removal of duplicates, 387 studies were left for Phase 1—reading of titles and abstracts according to eligibility criteria and for Phase 2—28 studies for reading of full texts. Two studies were excluded: one randomized clinical trial and another sandwich study. Finally, 15 studies were included in this review. Cryotherapy is effective in reducing pain intensity because there were reductions in the scores of subjective pain scales in the immediate PO of ACL reconstruction. Cryocompression was shown to be superior to conventional cryotherapy.
Introduction
Anterior cruciate ligament (ACL) injuries occur mainly during sports practice, especially when there is a need for rapid changes of direction associated with body contact, such as in soccer players (Siegel et al., 2012). Most patients report traumatic movement (sprain), clicking, painful limitation of movement, and a sensation of distortion. Treatment of these injuries can be conservative or surgical and there are criteria, such as age, level of activity, associated injuries, interest in returning to sports, risks of surgery, and other comorbidities, that are taken into account to decide which technique will be used (Kohn et al., 2020). However, surgical treatment is chosen for almost all individuals who wish to return to sports practice (Siegel et al., 2012).
In the postoperative period (PO), typical symptoms occur and treatment, still in the hospital phase, has as main objectives the control of pain, edema, and inflammation, with cryotherapy being an indicated resource (van Grinsven et al., 2010). From changes in tissue temperature, there is an increase in pain threshold, decrease in cellular activity, and vasoconstriction reducing local circulation and causing a decrease in edema (Swenson et al., 1996; Algafly and George, 2007; Vieira Ramos et al., 2016). Cryotherapy can be applied in several ways, such as ice packs, gel packs, and sprays, among other modalities (Swenson et al., 1996).
However, there are contradictory results of this modality in other knee surgeries, such as in the case of arthroplasties, requiring further clarification (Thienpont, 2014; Thacoor and Sandiford, 2019). Therefore, the aim of this study was to analyze the available literature on the effect of cryotherapy on pain intensity in the immediate PO of ACL reconstruction.
Materials and Methods
Eligibility criteria
This is a scoping review study conducted according to PRISMA recommendations (Moher et al., 2009). The acronym PICOS was used to formulate the question applied in this study. P (population): patients in the immediate PO of ACL reconstruction; I (intervention): cryotherapy; C (comparison): control groups and other therapeutic modalities; O (outcome): analgesia; S (type of study): randomized and nonrandomized clinical trials, systematic reviews, and overviews.
Inclusion criteria were randomized and nonrandomized clinical trials, systematic reviews, and overviews; studies that evaluated cryotherapy as an analgesic intervention in the immediate PO of ACL reconstruction, compared with a control group and other therapeutic modalities; studies that used a pain intensity measurement scale. We excluded retrospective study designs, case studies, cohort studies, pilot studies, studies published in expanded abstract format, editorials, studies whose texts were not available in full, reviews, letters, personal opinions, books, and book chapters. Experiments with animals were not included.
Information sources
To check the set of publications, individual search strategies were developed for the indexed databases: Cochrane, Embase, Lilacs, LIVIVO, PEDro, PubMed, Scopus, and Web of Science; and gray literature: Google Scholar, CAPES Thesis and Dissertation Base, and Open Grey. A reference manager software (EndNote Web, Thomson Reuters) was used to collect references and initially exclude duplicates. An example strategy with the terms used for the search: “Cryotherapy,” “Cold Therapy,” “Cold Therapies,” “Anterior Cruciate Ligament Injuries,” “ACL Injuries,” “ACL Injury,” “Anterior Cruciate Ligament Injury,” “Anterior Cruciate Ligament Tear,” “ACL Tear,” “ACL Tears,” and “Postoperative Period.”
Study selection and data collecting process
After the data collection process, the references were imported into EndNote Web manager for removal of duplicate articles, automatically and manually. Then they were imported into Rayyan QCRI (Qatar Computing Research Institute), and again, the removal of duplicates was performed. This defined the studies included in Phase 1 for the reading of titles and abstracts, according to eligibility criteria, by two blinded reviewers. Conflicting studies were resolved by consensus between the reviewers; in case of disagreement, a third reviewer was requested to determine the inclusion or exclusion of the article. The final selection, Phase 2, was based on the reading of the full papers by the two reviewers. There was no restriction on the language or year of publication of the studies.
Collected data
Two other independent reviewers collected and mapped the data from the included studies and prepared Tables 1 and 2 using an Excel® spreadsheet, with the following data: general information about the study (authors and year of publication), data about the samples, type of study, time of injury, type of ACL surgery, intervention, comparison, site of application, PO period that used cryotherapy, duration of sessions, number of daily sessions, temperature control, and results.
Description of the Articles, Including Type of Study, Sample Characterization, Type of Surgery and Pain Scale, According to the Authors
ACL, anterior cruciate ligament; M, men; NRCT, nonrandomized clinical trial; NVS, numerical visual scale; RCT, randomized clinical trial; VAS, visual analog scale; W, women.
Summary of Included Clinical Trials
CCDI, dynamic cryocompression; CCEP, static cryocompression; CG, control group; EG, experimental group; NVS, numerical visual scale; VAS, visual analog scale.
For the summarization step of the fundamental elements of each study, an in-depth analytical reading was performed for the categorization of the publications that provided the illustration of topics of interest. In the final step, the results were compiled and reported, to present the overview of all the material, by means of a thematic construction, organized according to the elements that influence the answer to the question of this research. The main outcome analyzed in this study was the intensity of pain.
Results
Study selection
A total of 603 studies were identified from indexed databases and 98 from gray literature. The searches were conducted on a single day, July 1, 2021. For Phase 1—reading titles and abstracts, a total of 304 studies, of which 276 were excluded according to eligibility criteria. For Phase 2—reading the full texts, 28 studies were included. Finally, using the same criteria, 15 studies were included in this review. Figure 1 summarizes the complete selection process.
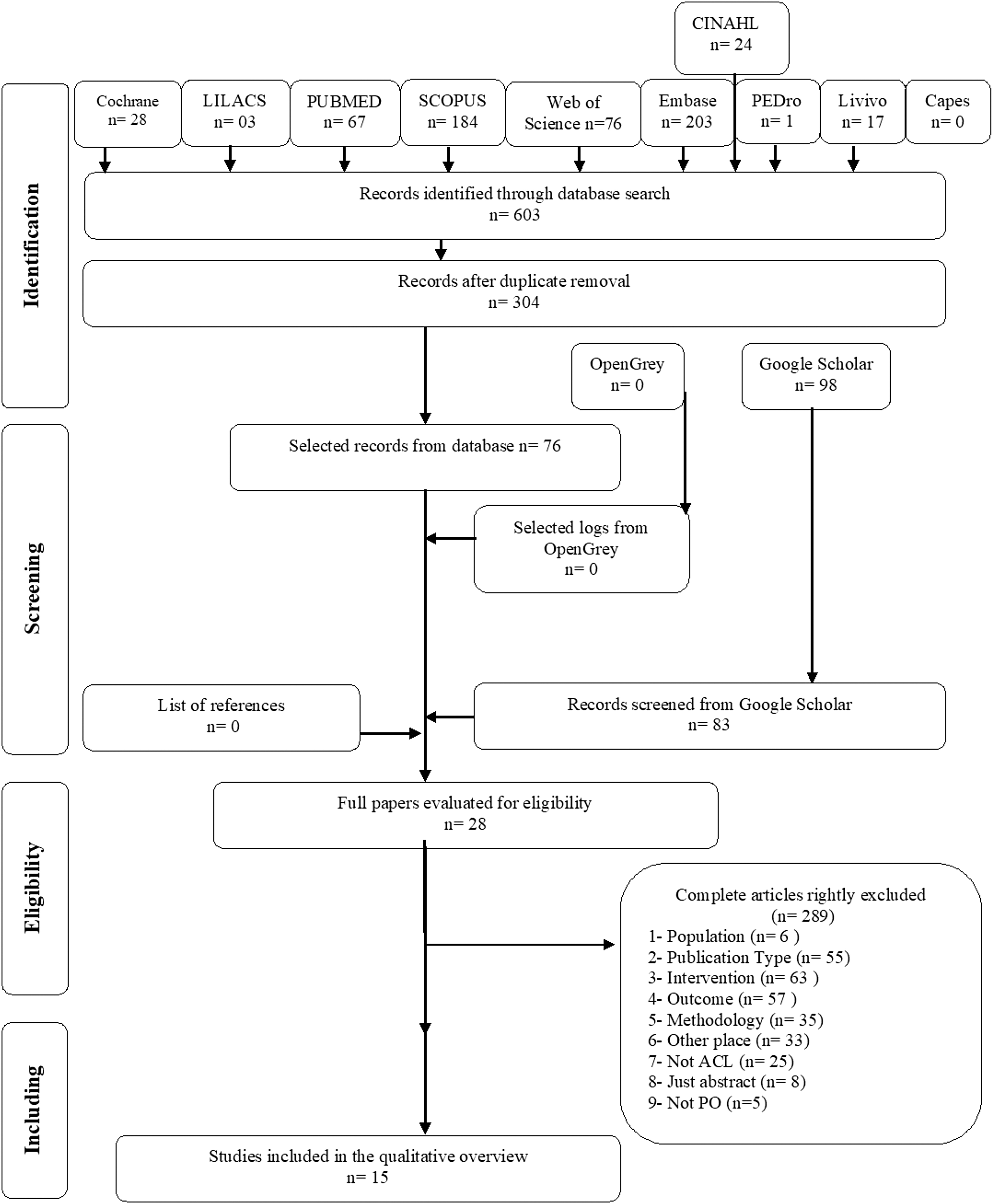
Flowchart of literature search and selection criteria, based on PRISMA (Moher et al., 2009).
Characteristics of the studies
Nine randomized clinical trials were included (Daniel et al., 1994; Schröder and Pässler, 1994; Brandsson et al., 1996; Edwards et al., 1996; Barber et al., 1998; Dambros et al., 2012; Waterman et al., 2012; Ruffilli et al., 2015; Kijkunasathian et al., 2017); one nonrandomized clinical trial (Murgier and Cassard, 2014); two systematic reviews (Martimbianco et al., 2014; Gatewood et al., 2017); two systematic reviews with meta-analysis (Raynor et al., 2005; Davey et al., 2021); and one critical literature review (Bednarski and Kiwerski, 2019). The publication date ranged from 1994 to 2021. In three studies, the sample was composed only of men (Schroder and Pässler, 1994; Murgier and Cassard, 2014; Kijkunasathian et al., 2017), the others by men and women, with a total sample of 577 subjects (Tables 2).
Results of the individual study
Collection instruments
To measure the outcome of this study (pain intensity), the following instruments were used: visual analog scale (VAS) (Daniel et al., 1994; Schröder and Pässler, 1994; Edwards et al., 1996; Dambros et al., 2012; Waterman et al., 2012; Kijkunasathian et al., 2017); visual numerical scale (Ruffilli et al., 2015), and Likert scale (Brandsson et al., 1996; Barber et al., 1998).
Outcome—pain intensity
Only the study by Brandsson et al. (1996) showed significant differences in the cryotherapy group (p < 0.05). The studies by Schröder and Pässler (1994), Barber et al. (1998), Waterman et al. (2012), Ruffilli et al. (2015), and Dambros et al. (2021) showed no statistical differences, but there was a reduction in pain scores and consumption of analgesic medications. Four studies that used cryocompression had positive results such as lower pain scores, reduced edema, and lower consumption of analgesic medications (Schröder and Pässler, 1994; Brandsson et al., 1996; Waterman et al., 2012; Murgier and Cassard, 2014). The two studies comparing ice pack and cryocompression had better results with cryocompression treatment (Schröder and Pässler, 1994; Waterman et al., 2012). Studies by Daniel et al. (1994), Edwards et al. (1996), and Kijkunasathian et al. (2017) showed no statistical differences in intergroup analysis, as well as no significant reduction in pain intensity.
ACL surgical procedure and mechanism of injury
About the type of surgery, four studies evaluated the OP of arthroscopic ACL reconstruction using the patellar tendon (Schröder and Pässler, 1994; Brandsson et al., 1996; Edwards et al., 1996; Barber et al., 1998), one study by “all inside” arthroscopic ACL reconstruction using the patellar tendon (Brandsson et al., 1996), two studies of arthroscopic ACL reconstruction using the hamstring (Dambros et al., 2012; Kijkunasathian et al., 2017), one study by the “over the top” method using the semitendinosus and gracilis tendon (Ruffilli et al., 2015), one study by Tape Locking Screw using the semitendinosus tendon (Murgier and Cassard, 2014), and one study did not specify the tendon used and that was arthroscopic reconstruction (Waterman et al., 2012). None of the studies specified the mechanism of injury.
Cryotherapy technique
Cryotherapy under the anterior surface of the knee was applied in the studies by Schröder and Pässler (1994), Kijkunasathian et al. (2017), and Dambros et al. (2012); three others under the entire knee surface (Barber et al., 1998; Waterman et al., 2012; Murgier and Cassard, 2014); two under the entire knee surface except at the patella (Brandsson et al., 1996; Edwards et al., 1996); one under the sides of the knee (Daniel et al., 1994); and one study did not specify (Ruffilli et al., 2015). The PO period of the intervention use ranged from 1 to 42 days, with sessions lasting from 20 minutes to 72 hours.
Discussion
The purpose of this scoping review was to investigate the state of the art in the use of cryotherapy as an intervention to reduce pain levels during the PO of ACL reconstruction surgery. Knowing that pain caused by surgical trauma in the immediate PO is an important barrier to the beginning of early rehabilitation, and that cryotherapy is considered a simple, inexpensive, and widely used analgesic modality in the acute phase of musculoskeletal injuries (Algafly and George, 2007; Dambros et al., 2012). It is important to provide information on the efficacy of this form of treatment in reducing pain in this condition; however, the results observed show that the subject is still open.
All the studies analyzed used subjective pain sensation scales. It is proposed that pain reduction by cryotherapy occurs by reduction in the conduction speed of nerve fibers by asynchronous transmission in pain fibers, release of endorphins and inhibition of spinal neurons, besides an increase in the refractory period, which leads to a gradual reduction in the transmission of impulses in the sensory nerves (Algafly and George, 2007; Bednarski and Kiwerski, 2019; Davey et al., 2021). Furthermore, studies show that cryotherapy reduces tissue blood flow and local cellular metabolism, making it indicated for the treatment of soft tissue and bone tissue injuries after acute traumatic injury to a large joint (Nadler et al., 2004).
Among the 10 selected studies, 5 analyzed cryotherapy associated with compression as a modality of therapy (Schröder and Pässler, 1994; Brandsson et al., 1996; Edwards et al., 1996; Waterman et al., 2012; Murgier and Cassard, 2014), 3 used continuous flow cooling devices (Daniel et al., 1994; Barber et al., 1998; Ruffilli et al., 2015), 1 used ice packs (Dambros et al., 2012), and 1 used thermal gel packs (Kijkunasathian et al., 2017).
Brandsson et al. (1996) and Edwards et al. (1996) compared cryocompression with placebo, but only in the first study was cold-associated compressive therapy superior to placebo in reducing pain. Both Schröder and Pässler (1994) and Waterman et al. (2012), compared cryocompression with ice pack, both obtained favorable results for cold therapy with compression, which significantly reduced pain compared with cryotherapy alone.
Murgier and Cassard (2014) made a comparison between a group submitted to intermittent dynamic cryocompression (GameReady®) and the other group to static cryocompression (IceBand®). There were no significant differences in pain scores between the two groups, but in the dynamic cryocompression group there was less analgesic consumption and better recovery of range of motion of the knee joint after surgery.
Dambros et al. (2012) compared the effects of the ice pack with placebo and found that the intervention group had a significant absolute and percentage improvement compared with the control, both in pain measurements and in range of motion of the knee joint. Kijkunasathian et al. (2017) performed a comparison between the cold thermal gel bag and the Robert Jones bandage. They found that the thermal gel bag was efficient in reducing pain, in addition to reducing edema, promoting greater patient satisfaction, and tended to have a better functional outcome.
Daniel et al. (1994); Barber et al. (1998), and Ruffilli et al. (2015) used as the primary form of intervention continuous flow cooling devices, a device that allows the regulation and maintenance of the therapy temperature, thus reducing the risk of damage to the patient's skin. Barber et al. (1998) and Ruffilli et al. (2015) obtained positive results regarding the reduction of pain scores. However, Daniel et al. (1994) demonstrated that, although this form of therapy decreased the skin temperature of individuals, it was not efficient in reducing pain, or in reducing the amount of analgesics used.
Owing to the heterogeneity of the types of ACL reconstruction surgery observed in the studies, no relationship was found between surgical techniques and the therapeutic results promoted by cryotherapy, with regard to analgesia, as well as in other variables analyzed, such as knee range of motion, edema, and overall patient satisfaction.
Another variable analyzed, and which may be a determining factor for the quality of the patient's prognosis and the effectiveness of the proposed therapies in the PO of ACL, was the time of injury until the surgical intervention was performed, because of the possibility of degenerative changes and neuronal plasticity of the pain matrix (Rahmati et al., 2017). Of the 10 studies, only those by Daniel et al. (1994), Schröder and Pässler (1994), and Ruffilli et al. (2015) presented the time of injury of the patients. Thus, analysis becomes difficult owing to the lack of information considered relevant.
Regarding the time of therapy, the application of cryotherapy ranged from 1 to 42 days. Therefore, it is also difficult to analyze the relationship between therapy time/pain reduction, because both in studies with long periods of therapy and in studies with short periods, time was not a determining factor in the amount of analgesia generated. Regarding the duration of the session, in six of them the cryotherapy time was at least 24 hours (Daniel et al., 1994; Schröder and Pässler, 1994; Brandsson et al., 1996; Edwards et al., 1996; Barber et al., 1998; Murgier and Cassard, 2014) and in two of them there was no significant difference (Daniel et al., 1994; Edwards et al., 1996).
Among the studies with shorter times per session—from 20 to 30 minutes (Dambros et al., 2012; Waterman et al., 2012; Kijkunasathian et al., 2017), two of them had significant improvement (Dambros et al., 2012; Waterman et al., 2012), varying from two to six sessions per day.
Four studies carried out temperature control (Daniel et al., 1994; Barber et al., 1998; Murgier and Cassard, 2014; Ruffilli et al., 2015), the temperature range was from 0°C to 21.11°C. Only in one study was improvement in pain and edema not achieved (Daniel et al., 1994).
As for the site of application, three studies used the entire knee surface (Barber et al., 1998; Waterman et al., 2012; Murgier and Cassard, 2014) and obtained significant improvement for pain; other two studies applied to the entire knee surface minus the patella (Brandsson et al., 1996; Edwards et al., 1996), and for Edwards et al. (1996) there was no improvement in pain; when applied to the anterior surface of the knee in one study the improvement was significant (Dambros et al., 2012) and there was no success for Daniel et al. (1994); Kijukunasathian et al. (2017) used ice on the sides of the knee, with no efficacy in pain relief. The study by Ruffilli et al. (2015) did not specify the application site, but demonstrated good results on the first postoperative day.
Three reviews (two systematic and one critical review) and two meta-analyses were selected to complement the study findings on the efficacy of cryotherapy in reducing postoperative pain in ACL reconstruction surgery. In the systematic review by Martimbianco et al. (2014), 10 clinical trials were analyzed, totaling 573 patients (n = 573). From them, the researchers concluded that cryotherapy significantly reduces pain in the PO of ACL reconstruction, and that this form of therapy does not increase the risks of adverse events, in the short term (up to 48 hours after surgery).
Gatewood et al. (2017), in a systematic review, analyzed 25 studies of devices used after arthroscopic knee surgery. Of these 12 were related to cryotherapy. Regarding the reduction in pain by cryotherapy, the researchers concluded that this therapeutic modality was the most consistent in reducing pain and narcotic consumption during the immediate PO of arthroscopic knee surgery. Furthermore, they concluded that cryocompression appeared to be more effective than conventional cryotherapy in reducing pain and the use of analgesics after knee arthroscopy. However, they also concluded that cryocompression devices did not show better outcomes than compression alone.
In the critical review by Bednarski and Kiwerski (2019), the main objective was to evaluate the effectiveness of cryotherapy, including cryostimulation, after ACL reconstruction surgery. The researchers included 16 publications, 1 meta-analysis, 2 systematic reviews, and 13 clinical trials. They indicated that cryotherapy procedures are frequently used in patients with musculoskeletal injuries and in the treatment with postoperative patients of orthopedic surgeries. They concluded that owing to the low cost and easy applicability of ice and cryotherapy devices, these forms of treatment appear to be good techniques for rehabilitation of patients after ACL reconstruction surgery.
The meta-analysis by Raynor et al. (2005) combined research with scientific evidence that evaluated the effectiveness of using cryotherapy after arthroscopic ACL reconstruction surgery. Six randomized clinical trials were included, which analyzed knee pain using VAS. This article concluded that cryotherapy has a positive effect on postoperative pain control and that in future studies cold therapy should be compared with other methods of analgesia, such as continuous anesthesia and new analgesic medications. Furthermore, the authors comment that the cost–benefit relationship should be analyzed to quantify the relationship between the benefit generated to the patient and the costs and difficulty in applying the cryotherapy technique.
In the systematic review with meta-analysis of multiple treatments performed by Davey et al. (2021), 74 randomized clinical trials were analyzed with the objective of determining the best available evidence in the management of postoperative pain caused by ACL reconstruction surgery, and to optimize the patient's prognosis. Regarding cryotherapy, the study concluded that this form of treatment has good evidence to promote pain control and reduce the use of opioids in the PO of ACL reconstruction surgery.
Because cryotherapy is considered a promising analgesic technique, of low cost and easy clinical applicability, its application in the immediate PO of arthroscopic surgery for ACL reconstruction becomes a possible ally for pain management in this situation. However, new studies dealing with the time of therapy are necessary for a better therapy, because the results are very heterogeneous.
Conclusion
Based on the studies analyzed, it is concluded that cryotherapy is effective in reducing the intensity of pain, as there were reductions in subjective pain scale scores in the immediate PO of ACL reconstruction, and the application of cryotherapy to the entire surface of the knee produces better analgesic effects. Cryocompression was shown to be superior to cryotherapy with ice packs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding agency. The resources were the institution's own and aid (Unioeste).