
Abstract
This study compares the treatment outcomes between target temperature management (TTM) and normal temperature management (NTM) for cardiac arrest after traumatic brain injury (TBI). Two reviewers searched PubMed/MEDLINE, China National Infrastructure database for studies reporting on the use of TTM and NTM. All publications from inception to October 2021 were considered. Randomized control trials (RCTs) with cardiac arrest after TBI diagnoses were made based on the 2019 American Stroke Association (ASA) guidelines,1 wherein the included cardiac arrest patients underwent TTM or NTM treatment were included in this study. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommended tool was used for assessing the risk of bias of the included RCTs. In all, 1920 publications were identified. However, after applying the inclusion and exclusion criteria, 6 RCTs, including 1617 patients who received TTMs (n = 826) and NTMs (n = 791), were considered eligible. The meta-analysis indicated that compared with NTM, TTM did not show a decrease in the mortality, however, for those mild patients in the early stage, TTM still can decrease the mortality and better the prognosis. Compared with NTM, TTM is an effective measure to treat mild and severe patients in the early stage and improve the prognosis.
Introduction
Traumatic brain injury (TBI) is a life-threatening condition which may lead to the impairment of physical, psychosocial, and cognitive functions. It is mainly caused by external assault leading to brain damage (Panchal et al., 2019). The initiator of the TBI can be widely, including traffic accidents, military incidents, fall downs, sports accidents, construction accidents, violent crime, and gun shots. It is reported that more that 20 million people around the globe are living with the TBI-related disability (Capizzi et al., 2020). These disable people are unable to return to normal life, which cause very serious economical burdens. Studies from World Health Organization have estimated that more than 100 billion dollars of expenditures occur annually as a outcome of TBI from lost incomes of the TBI-related people and their friends (Tarvonen-Schröder et al., 2018).
Target temperature management (TTM) is a standardized procedure which can decrease the metabolism of the brain and minimize the neuronal loss or damage, aiming to improve the prognosis of the patients (Bergman et al., 2015). However, in recent years, many studies considered the TTM, compared with normal temperature management (NTM), did not decrease the all-cause mortality at 90 days (Andrews et al., 2017; Cooper et al., 2018). TTM can be classified into several subgroups according to the temperature scale achieved; ultra profound (0–5°C), profound (5–10°C), deep (10–28°C), mild (33–36°C), and moderate (10–28°C) (Tisherman et al., 1999).7 In the TBI cases, some studies produced positive results while some studies produced negative outcomes. Some systemic reviews also reported the negative outcomes (Crossley et al., 2014; Zhu et al., 2016; Crompton et al., 2017).
A large meta-analysis (Crompton et al., 201) conducted a positive outcome indicating that the TTM is an effective way to treat the TBI. This outcome may be due to the influence of large number of low-quality studies. We aimed to conduct a comprehensive, systemic, and reliable meta-analysis to conclude the benefits and limitations of the TTM by analyzing the mortality rates, neurologic damage, and adverse effects.
Methods
This meta-analysis was constructed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist.
Eligibility criteria
Studies meeting the following criteria were included in the analysis: (1) randomized control trials (RCTs); (2) Cardiac arrest diagnosis as per the 2018 American Stroke Association (ASA) guidelines; (3) patient age >18 years; and (4) TTM or NTM as a treatment measure. No restrictions were placed on race or nationality. The following studies were excluded: (1) reviews, case reports, and expert reviews; (2) animal studies; (3) in vitro studies; (4) repeat publications or data duplication; and (5) non-TTM studies. Interventions included TTM and NTM. In some cases, patients were first treated with TTM, but later treated via NTM laterally; these patients were included in the TTM group.
Search strategy
Two reviewers independently searched the PubMed/MEDLINE, China National Knowledge Infrastructure database, WANFANG database, and China Biology Medicine database for RCTs, wherein TTM or NTM was used to treat cardiac arrest after TBI patients via manual search. The RCTs comparing between TTM and NTM regarding cardiac arrest after TBI treatment were shortlisted. Further, the studies were filtered for the publication year, and all studies published until January 2021 were included. The search keywords were “traumatic brain injury,” “TTM,” “cardiac arrest,” “NTM,” “random allocation,” “random,” “randomly,” and “randomized.”
We searched for articles in all languages, and the articles were translated when necessary. We also searched for some relevant references in the articles; the retrieval was constructed by the free words and the subject words plus the free words. The titles and abstracts were searched for the abovementioned keywords using the following search operators: “target temperature management” OR “normal temperature management” OR “cardiac arrest after traumatic brain injury.”
Literature quality screening and quality evaluation
We used tools recommended by the PRISMA (Liberati et al., 2009) to assess the risk of bias of the studies included in the analysis. Quality assessment was performed by two reviewers individually, and in case of a disagreement, a third reviewer was consulted. The quality of studies can be divided into three levels.
Level A: the study meets the requirements of the randomization, allocation concealment, blinding, standard follow-up, and proper methodology. This level represents the minimum risk of bias.
Level B: the study meets one or more of the following requirements: randomization, allocation concealment, blinding, standard follow-up, and proper methodology. This level represents moderate risk of bias.
Level C: the study does not meet any of the afore-mentioned requirements. This level represents high risk of bias.
In the 6 studies we enrolled, 5 met Level A and 1 met Level B (Table 1).
Quality Assessment
RCT, randomized control trial.
Data extraction
Researchers extracted data from articles by reading the titles and abstracts, then screened the studies that met the eligibility criteria, and constructed an Excel sheet named “Data extraction archive.” The following data were recorded: general information (author, publishing date, language, nationality, and research type); quality data (allocation concealment, blinding method, and follow-up); intervention data (treatments and control measures); outcome data; and all measurements recorded in the original studies.
Outcomes
In the enrolled studies, one or two of the following main research indicators must be included: (1) primary endpoint: mortality and (2) secondary endpoint: severe nervous system damage. We use odds ratios (ORs) and 95% confidence intervals (CIs) to assess the outcome quantitatively.
Statistical analyses
This meta-analysis is based on binary-continuous method. The outcome measures were evaluated by ORs and 95% CIs. We used Stata SE to analyze the collected data. The I2 statistic was applied for the analysis owing to the heterogeneity. p-Values <0.05 or I2 value higher than 50% indicated heterogeneity, and its origin was taken into consideration. Following this, if the heterogeneity still existed, a random effect model was adopted for analysis. In contrast, a fixed-effect model was adopted when the p-value was >0.05 or the I2 value was not more than 50%. The stability of this meta-analysis was evaluated by eliminating any of the studies successively. We drew a forest plot and risk-of-bias plot using STATA SE (version 15). The funnel plot and the sensitivity analysis (publication bias) were also acquired using STATA SE (version 15).
Results
We identified 4207 references, including 3740 from PubMed/MEDLINE, 37 from CNKI, 3 from WANFANG, 171 from CBM, and 256 from EMBASE. The deadline for the publication date was set for July 31st, 2021. Following this, the study selection was carried out based on the eligibility criteria and the duplicate studies were removed in this process. After reading the title and abstract, 1038 articles were excluded according to the exclusion criteria. Finally, 1617 subjects of 6 studies that met the inclusion criteria were selected for further analysis. The screened flowchart is as follows (Fig. 1). The basic characteristics of patients enrolled in the study can be seen in Table 2.

Screened flowchart. NTM, normal temperature management; RCT, randomized control trial; TTM, target temperature management.
The Basic Characteristics of Patients
CA, cardiac arrest; NTM, normal temperature management; TBI, traumatic brain injury; TTM, target temperature management.
Effect of TTM and NTM on the mortality of patients and in terms of moderate and severe nervous system injury in cardiac arrest after traumatic injury patients
Further, 6 studies in our analysis were associated with morbidities. Of the 1617 patients included in these 6 studies, 826 patients underwent TTM treatment, and 791 patients underwent NTM treatment. In the TTM group, the death number is 505 compared to the 485 in NTM group, The TTM cannot decrease the mortality of cardiac arrest after traumatic injury (CATI) patients. (Heterogeneity chi-squared = 10.78 [d.f. = 5] p = 0.056, I-squared [variation in relative risk [RR] attributable to heterogeneity, Estimate of between-study variance Tau-squared = 0.0181], Test of RR = 1: z = 0.22 p = 0.829, No statistical variance) (Fig. 2).
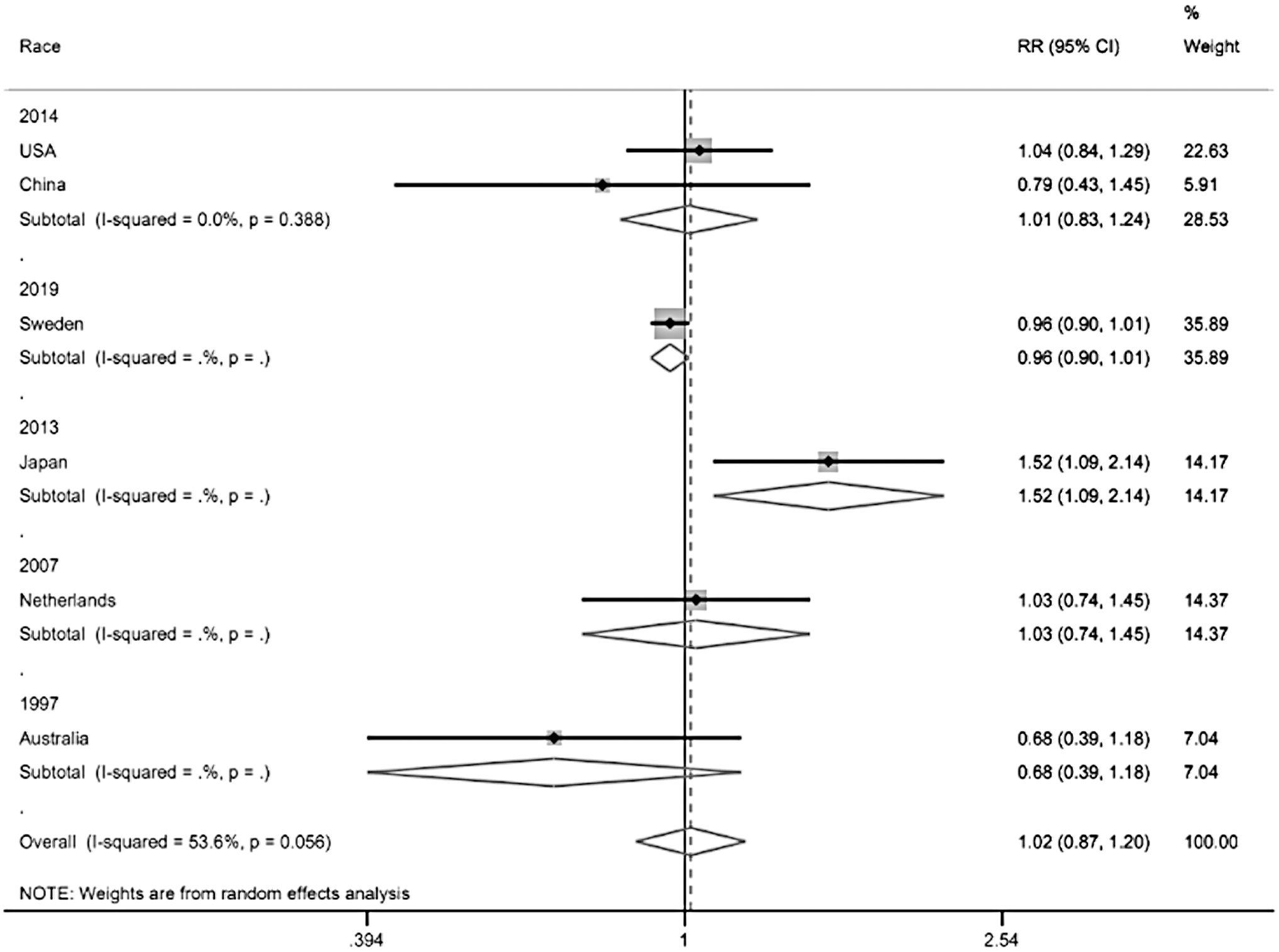
The Forrest of mortality subgroup analysis. CI, confidence interval; RR, relative risk.
Further, 6 studies in our analysis were associated with morbidities. Of the 1617 patients included in these 6 studies, 826 patients underwent TTM treatment, and 791 patients underwent NTM treatment. The number of patients with moderate nervous system injury in the TTM group was 33 and that in the NTM group was 45. The number of patients with severe nervous system injury in the TTM group was 35 and that in the NTM group was 57. It seems that TTM can decrease the number of moderate and severe patients.
We analyzed the related data and concluded that the TTM can decrease the number of moderate and severe CATI patients (Figs. 3 and 4) (Forrest picture Heterogeneity chi-squared = 2.83 [d.f. = 3] p = 0.419, I-squared [variation in OR attributable to heterogeneity] = 0.0%, Test of OR = 1: z = 3.59 p = 0.000. Compared to the NTM group, the TTM can decrease the number of severe nervous system injury after the CATI) (Heterogeneity chi-squared = 1.31 [d.f. = 3] p = 0.727 I-squared [variation in OR attributable to heterogeneity] = 0.0%, Test of OR = 1: z = 2.60 p = 0.009. Owing to the analyzed result, the TTM can decrease the number of moderate nervous system injury after the CATI).

The Forrest of moderate nervous system damage. OR, odds ratio.

The Forrest of severe nervous system damage.
Discussion
This meta-analysis indicated that compared with the NTM, TTM is a safe and effective way to salvage patients suffering from CATI. We included 12 studies in our analysis with the aim to compare between TTM and NTM for treating CATI. Our statistical analyses showed that the number of deaths in the TTM group was slightly higher (505/990) than that in the NTM group (485/990). The number of patients with mild nervous system injury in the TTM group was 258 (n = 488) and that in the NTM group was 230 (n = 488) (Fig. 5).
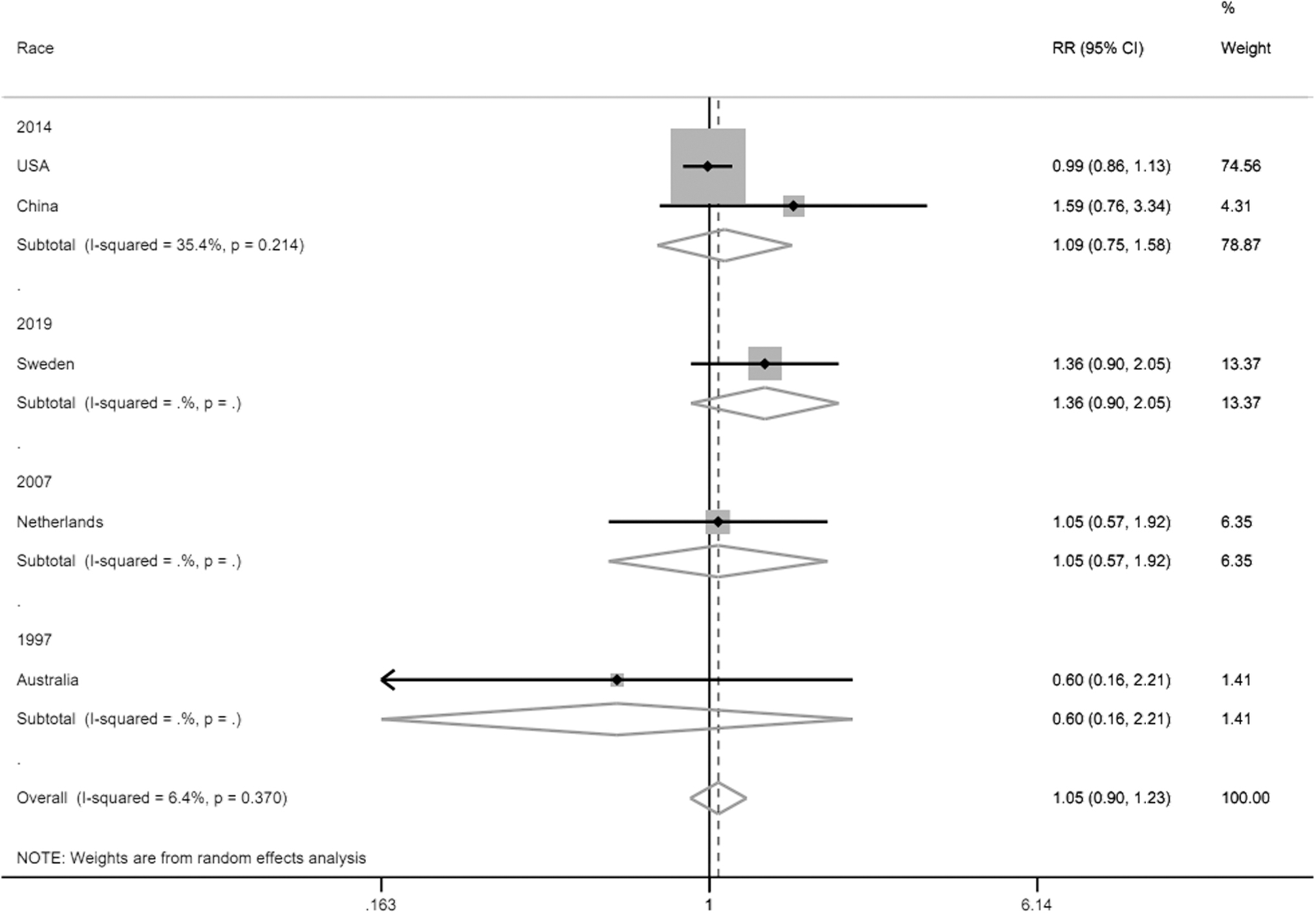
The Forrest of mild nervous system damage.
The number of patients with moderate nervous system injury was 33 in TTM group, while that number in NTM group was 45. The number of patients with severe nervous system injury was 35, compared to the 57 patients in NTM group, TTM seemed to decrease the severe number. Although TTM cannot decrease the mortality of CATI patients, it still can decrease the number of moderate and severe cases.
Postanoxic cerebral injury is the major complication after the cardiac arrest. The international experts' guidelines told us that the TTM is a recommendation after the out of hospital cardiac arrest (OHCA). However, the evidence is the major contributor, which guides us in the daily medical practices. In some predecessor's studies, the TTM at 33°C for 12–24 hours can improve the neurological outcomes compared to the NTM in the OHCA patients. But some subsequent studies raised some questionable issues about the efficacy of the TTM in other settings, such as the in-hospital cardiac arrest patients. After the TTM first came to our society, many studies were performed to illustrate the efficacy of the TTM. The TTM seems useless in bettering the outcomes of the CATI patients.
However, our study showed that they can reduce the number of the critical and moderate patients. This study has some limitations, the patients we enrolled are hard to find. Although TTM can reduce the condition in critically ill and moderately ill patients, this study has certain limitations and the sample size is limited. However, its role in improving outcomes in CATI patients has not been adequately demonstrated due to limitations in the scope of the study. In future research, we will increase the number of studies and the scope of the study area. Guidelines for the Management of Severe Traumatic Brain Injury 4th Edition also provide meta-analysis of Prophylactic Hypothermia application studies describing benefits and restriction of different study cases. Interestingly, there are no general conclusion regarding added value of hypothermia application for TBI patients' treatment, as every clinical case and every study is specific (Nancy et al., 2017).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.