
Abstract
Avoiding redistributional hypothermia that decreases core temperature by 0.5–1.5°C within the 1st hour of surgery is difficult. The efficacy of prewarming using a forced-air warming (FAW) device with a lower-body blanket on redistribution hypothermia during epidural procedures have not been investigated. After ethics approval, 113 patients undergoing laparoscopic surgery under general anesthesia combined with epidural anesthesia were enrolled. Intervention (prewarming) group patients who were warmed from operating room entry, including during epidural anesthesia, was compared with the control group that was warmed from just before surgery started. In total, 104 patients (52, control; 52, prewarming) were analyzed. In the prewarming group, compared to the control group, the core temperature 20 minutes after anesthesia induction (36.9 ± 0.4 vs. 37.1 ± 0.4°C, p < 0.02) was significantly higher. The core temperature was higher in the prewarming group than in the control group until 3 hours after the surgery. In the prewarming group, compared to the control group, the core temperature-time integral below baseline till 180 minutes after surgery start (65.1 ± 64.0 vs. 8.1 ± 18.6°C/min, p < 0.0001) or 30 minutes after anesthesia induction (5.3 ± 6.2 vs. 2.0 ± 4.7°C/min, p < 0.0001) were significantly smaller. Postoperative shivering was comparable between the groups. Prewarming during epidural catheter insertion with a FAW device could safely prevent a core temperature decrease induced by redistribution or heat loss without additional preparation, effort, space, or time requirements.
Introduction
Body temperature management is important during surgery to prevent complications (Hart et al., 2011; Fettes et al., 2013). In a relatively recent retrospective study that analyzed cases involving 45,304 patients from a single institution, noncompliant patients who did not use an appropriate active warming device during surgery or who were hypothermic (<36°C) during the postoperative period had an increased risk of infection, ischemic events, and mortality compared to compliant patients (Scott et al., 2015). The main mechanisms of heat loss during the 1st hour of surgery related to anesthesia are thermal redistribution between the central and peripheral compartments due to the opening of the arteriovenous shunt and the alteration of the response mechanisms of the hypothalamus by anesthetics. Among the four potential heat-loss mechanisms (radiation, conduction, convection, and evaporation), radiation usually contributes the most (Sessler, 2000).
Hypothermia during general anesthesia has a characteristic pattern of exhibiting an initial rapid decrease in core temperature due to redistribution, followed by a linear reduction in core temperature due to heat loss. It is especially difficult to avoid redistribution hypothermia that decreases core temperature by 0.5–1.5°C within the 1st hour of surgery (Hart et al., 2011). Consequently, several body warming methods or techniques for preventing redistribution hypothermia were reported. However, some aspects were not investigated, including the effects of prewarming on redistribution hypothermia using forced-air warming (FAW) device with a lower body blanket during epidural procedures.
Epidural catheter inserted into the epidural space matched the position of the skin incision for postoperative pain control, but the patients' temperature could be decreased by the operating room (OR) cold environment during this procedure. In addition, stress could cause a transfer of heat from the periphery to the core, inducing a fast body temperature decrease after induction of anesthesia. On using a lower body blanket, patients are kept warm continually right from admission to their entry into the OR.
The current study tested the hypothesis that prewarming with FAW during epidural catheter insertion would (1) maintain preoperative core temperature, and (2) prevent postoperative shivering and not influence other adverse events. Then, the primary endpoint of this study was to determine the effect of prewarming with FAW devices on body temperature during surgery. The temperature-time integral below baseline till 180 minutes after surgery start was calculated. As sensitivity analysis of primary outcome, the temperature-time integral below baseline till 30 minutes after anesthesia induction was also calculated. In addition, the effect of age or sex was examined as subgroup analysis. The secondary endpoint was to compare the development of postoperative shivering or adverse events between the two scenarios.
Methods
Study design
The Clinical Research Ethics Committee of Kyushu University, Fukuoka, Japan, approved this open, randomized control, single-center, exploratory clinical trial (April 14, 2020) (ID No. 20192035). The study is registered at UMIN Clinical Trials Registry (April 15, 2020) (UMIN000040065). All aspects of the study protocol complied with the Declaration of Helsinki (2013).
A total of 120 patients (over 20 years old) undergoing laparoscopic surgery in the supine position under general anesthesia combined with epidural anesthesia were assessed for eligibility from April 20, 2020 to August 20, 2020. These criteria were chosen to prevent body temperature changes caused by the operating procedure and positional changes. The exclusion criteria were patients with serious complications, especially those with American Society Anesthesiologist physical status IV, or subjects without an adequate medical record. These eligibility criteria remained constant throughout the study. After obtaining written informed consent, the participants were randomized to one of two groups by permuted-block randomization in block size of 4 (Excel, Microsoft Corporation, Redmond, WA). The randomization process was performed by K.N., who was independent of the analysis process (Supplementary Data).
Warming method
The patients in the intervention group (prewarming group) were warmed using the 3M Bair Hugger FAW system (Model 750; 3M Company, Maplewood, MN) and an underwarming blanket (Model 585; 3M Company), which together comprised the FAW device, with the warming temperature set to 43°C, from the time they entered the OR until their extubation from the OR, including the period of epidural catheter insertion. The warming temperature started at 43°C, and the core temperature was target to 38°C to prevent excess hyperthermia. The patients in the control group were warmed from the start of surgery until their discharge from the OR with the same device used in the intervention group. In both groups, all patients were covered by a cotton blanket for passive insulation from the start of the epidural anesthesia induction procedure.
Anesthesia method
For the anesthesia procedure, after entering the OR, a peripheral vein cannula was inserted into all the patients, and they were administrated a crystalloid solution along with the application of an active warming device (Level 1, Hot Line™; Smiths Medicals, St. Paul, MN) under standard monitoring conditions. The epidural catheter insertion procedure for postoperative pain control was performed in the lateral position in all the patients. Anesthesia was induced in all the patients via the intravenous administration of fentanyl, propofol, and rocuronium. It was maintained with desflurane (4–5%), sevoflurane (1–1.5%), or propofol (2.5–4 μg/mL, target-controlled infusion), remifentanil, and a 40–50% oxygen-room air mixture. Additional bolus infusions of fentanyl and rocuronium were administered as needed.
Toward the end of the surgery, all the patients were administered a bolus local anesthetic agent via an epidural catheter and acetaminophen intravenously. Body core temperature measured using the SpotOn™ temperature system (3M Company) and peripheral temperature at the fingertip (Surface Type Thermistor Temperature Probes, Nihon Kohden, Japan) were recorded in both groups from the entry onto the OR until the completion of surgery (Eshraghi et al., 2014; Evron et al., 2017; Sastre et al., 2019). Before and during surgery, the air-conditioning temperature in the OR was set to 28°C and 25°C, and the humidity was set to 50% and 40%, respectively.
Measurements
The body temperature at OR entry (baseline), at the start of surgery, every 30 minutes until 3 hours from the start of surgery, and at the end of surgery were extracted from the patient's electronic anesthesia record provided by the warehouse system (FineData™, Nihon Kohden, Japan). Comparisons of postoperative shivering or infection development at the epidural puncture site between the groups were compared.
Analysis
Since this was an exploratory study, a sample size calculation was not performed. The researchers aimed for 120 participants because it would be feasible to enroll and give enough information to prepare for the confirmatory trial. No interim analysis was planned or conducted. From a medical standpoint, we cannot refer to previous studies because there were few reports which investigated the effect of FAW during epidural anesthesia on prewarming. In addition, there are medical differences in treatment efficacy or data variability between similar prior and this method using FAW. Specifically, in the prior method, FAW was also used after epidural anesthesia, including before, or the patient was transferred to the OR after prewarming because prewarimg was mainly performed in an extra-OR. Then, the number of cases in this study was designed from feasibility as an exploratory positioned clinical trial.
Data are reported as mean ± standard deviation, and estimates are reported mean and 95% confidence interval (CI). To assess the differences in the primary outcome in body temperature between the groups with and without prewarming, an unpaired t-test was used. The patient characteristics, development of shivering as secondary outcomes in the two groups were compared using Fisher's exact test. The GraphPad Prism (version 8.4.3; GraphPad Software, San Diego, CA) was used to perform all statistical analyses. Two-sided p-values of <0.05 were considered statistically significant in all the analyses. When parametric tests are performed on skewed data, a bias is introduced.
However, this bias is in the conservative direction, which makes it harder to be statistically significant. In this study, we were interested in how much the difference between groups is, but the nonparametric method does not answer the research question. Therefore, parametric statistical methods were used. The results of the conservative analysis also showed a significant difference, which does not undermine the significance of the study.
This randomized controlled trial was reported according to the updated guidelines for reporting parallel group randomized trials (CONSORT 2010 statement).
Results
Baseline characteristics
In total, 120 patients treated at the Kyushu University Hospital from April 20, 2020 to August 24, 2020 were assessed in this study. Six patients were excluded before randomization because epidural anesthesia induction was cancelled due to anticoagulant therapy. One patient was excluded from this study because of his aversion to being a research subject after surgery. Five patients in the control group and four patients in the prewarming group were excluded because their data at OR entry were missing. Finally, 104 patients, 52 patients in the control group, and 52 patients in the prewarming group, were analyzed in this study (Fig. 1; Supplementary S1). There were no missing data on body temperature in the full-analysis set; therefore, no values imputation was required.
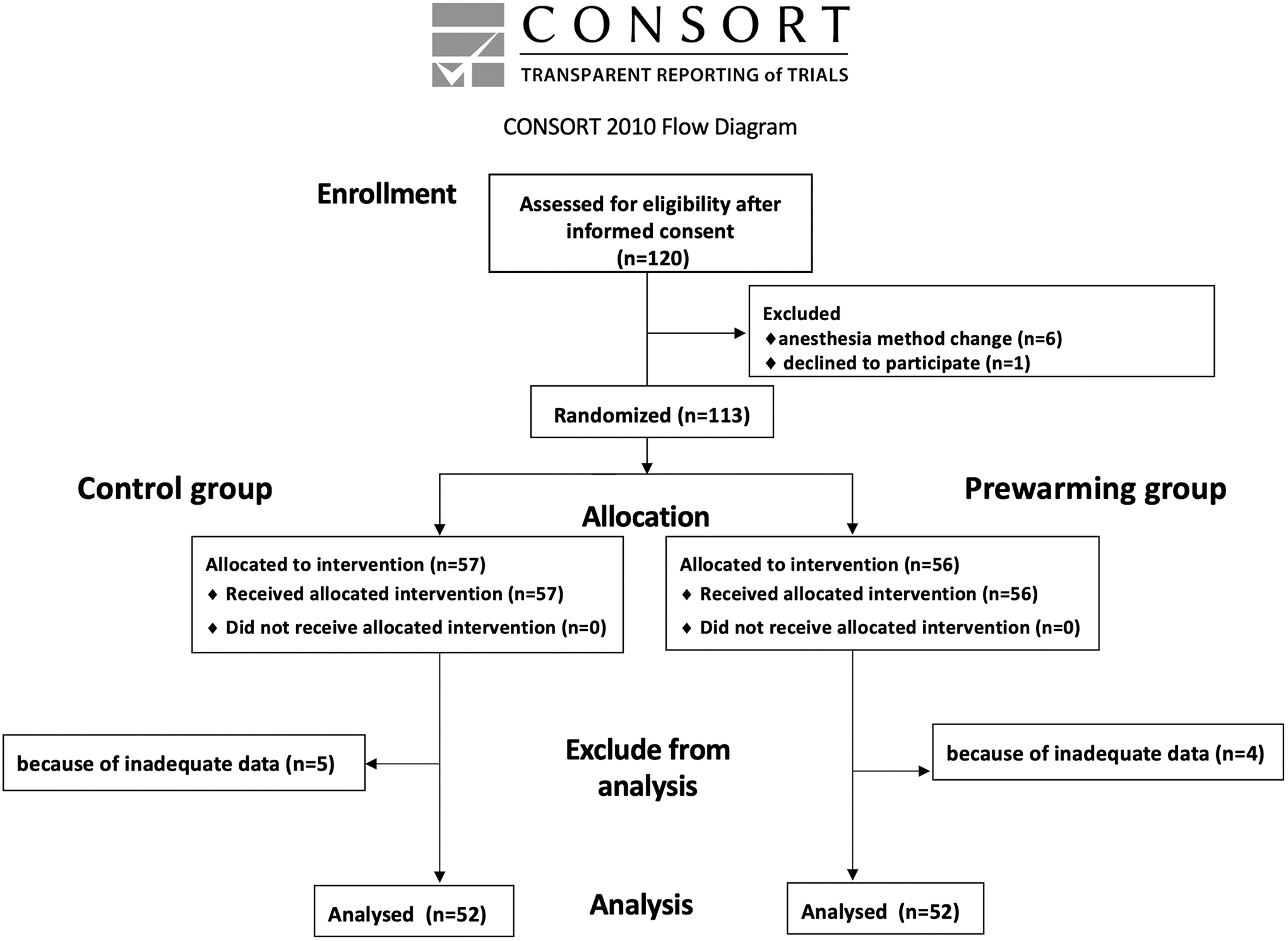
Study inclusion/exclusion flow diagram.
Core temperature: primary outcome
Core temperatures at entering or anesthesia induction between both groups were almost identical. In the prewarming group, compared to the control group, the core temperature 20 minutes after anesthesia induction (36.9 ± 0.4 vs. 37.1 ± 0.4°C, p < 0.02) was significantly higher (Table 1). Core temperature was higher in prewarming group than control group till 3 hours after surgery start.
Comparison of Core Temperature Between the Control and Prewarming Groups
SD, standard deviation.
In the prewarming group, compared to the control group, the core temperature-time integral below baseline till 180 minutes after surgery start (65.1 ± 64.0 vs. 8.1 ± 18.6°C/min, p < 0.0001) was significantly smaller (Fig. 2A; Table 2).

Comparison of the effect of prewarming on core temperature.
Primary Outcome: The Effect of Prewarming with Forced-Air Warming Device from Epidural Procedures on Body Temperature During Surgery
CI, confidence interval.
In the prewarming group, compared to the control group, the core temperature-time integral below baseline till 30 minutes after anesthesia induction (5.3 ± 6.2 vs. 2.0 ± 4.7°C/min, p < 0.0001) was significantly smaller (Fig. 2B; Table 2).
The effect of age or sex: subgroup analysis
We analyzed baseline subgroups (age-category and sex) by the core temperature-time integral below baseline till 180 and 30 minutes after surgery.
Subgroup results were generally consistent with the overall result (Table 2).
Development of shivering: secondary outcomes
The development of postoperative shivering was comparable [control: 3/52 (5.8%), prewarming: 1/52 (1.9%), p = 0.62] in both the groups. The odds ratio for postoperative shivering in the prewarming group was 0.32 (95% CI: 0.02–2.2).
Discussion
Although the primary endpoint was statistically significant, the mean temperature difference between the two groups 1 hour after the start of surgery was 0.68°C. In addition, the mean temperature 1 hour after the start of surgery and 30 minutes after the anesthesia induction was, respectively, 0.3°C and 0.1°C higher than the baseline in the prewarming group (Table 1; Fig. 2B; Supplementary S2). Several studies have also reported the effective prewarming method to prevent decreasing core temperature during surgery, but few reports could succeed to prevent redistributive hypothermia.
Furthermore, previous prewarming techniques required additional time or space. Specifically, the techniques reported were warming patients in the ward before the transfer to the OR using a self-warming blanket (Torossian et al., 2016), warming patients with a warming suit in the preoperative area (Perl et al., 2014; Akhtar et al., 2016), warming patients with a FAW device 15 minutes before and after the epidural catheter insertion procedure (Horn et al., 2002), or warming patients with a FAW device in the preoperative care unit (Horn et al., 2016). Similarly, Kaufner reported that prewarming using a Flex warming gown (3M™, St. Paul, MN) during epidural catheter insertion was useful in preventing a decrease in body temperature during surgery (Kaufner et al., 2019). Their warming gown only warms the front of the body, including the upper arms, and the epidural catheter should be inserted in the sitting position.
Recovery core temperature
Currently, laparoscopic surgery is the most widely used surgical technique; the associated heat loss is lower than that observed in open surgery. However, it took 3 hours till core temperature was recovered to level at entering in control group (Table 1). Potentially, prewarming could be more beneficial in preventing a decrease in body temperature in any type of surgery.
Prevention of temperature redistribution
In patients undergoing off-pump coronary artery bypass surgery, prewarming with a FAW device applied only during the induction of anesthesia could prevent a decrease in core temperature compared to in a nonprewarming group during the first 3 hours of anesthesia (Cho et al., 2016). This report indicated that prewarming during the induction of anesthesia could be efficient in preventing a decrease in body temperature. In addition, it was reported that active warming with a FAW device set to 43°C resulted in an increase of 69 kcal in the heat content measured in the arms and legs during the first 30 minutes of warming in a volunteer study (Sessler et al., 1995). The reason why redistribution hypothermia was not detected in prewarming group in this study could be due to this heat generation and accumulation.
The tendency of difference in peripheral temperature (Supplementary S3) could be explained by the higher increase of peripheral temperature by FAW in the prewarming group than by heat distribution in the control group. These results also indicated that peripheral temperature might be an indicator of the effects of prewarming. However, we must carefully evaluate the peripheral temperature because the fingertip attached peripheral temperature sensor is placed above FAW under the blanket, so it is easily affected by environmental temperature.
On the contrary, the slow rise in peripheral temperature and the fact the temperatures measured by the zero-heat-flux sensor in both groups were very similar (Table 1) and clinically insignificant (<0.5°C) might mean that the prewarming technique was not very effective. These results might be attributed to the fact that the OR temperatures (25–28°C) were also higher than those usually recommended, which may cause apparent lack of redistribution in both groups. Specifically, temperatures at 30 minutes after induction was only 0.3°C lower than at 10 minutes after induction or baseline in the control group (Table 1). Another possible bias factor is the method used to measure core temperature. The zero-heat-flux sensor has long equilibration times (about 10 minutes), which might make it difficult to measure the rapid heat transfer that occurs during induction of anesthesia (Table 3).
Comparison of Perioperative Values Between the Control and Prewarming Groups
Moreover, forced-air blankets working under the patient are less effective for several reasons, including less body surface area exposed to convective heating (because lateral heating compared to frontal heating with blankets placed on top of the patient) and more extensive radiation and convective heat getting lost in the environment (Fernandez-Mere and Alvarez-Blanco, 2012).
Development of shivering
In this study, the temperature at the end of surgery and postoperative development of shivering were almost the same between the two groups. This result might be due to the extended surgical procedure and antishivering effects of acetaminophen (Shirozu et al., 2020) or the strict maintenance of the warming strategy using fluid warming or FAW. Recently, Sessler et al. (2022) reported that a core temperature of at least 35.5°C during surgery is sufficient to prevent major cardiovascular events and surgical site infections. However, the risk of postoperative shivering has not been investigated, and high-risk cardiovascular patients were not included in their study. On the contrary, postoperative management and antibiotic efficacy have improved, and old data may not be helpful. Therefore, further research is warranted.
As a limitation, this was a single-center study. Since this study was an exploratory trial, it should be validated by a multicenter confirmative trial. In addition, this clinical trial was done without accounting for sample size. Although, the temperature difference between both groups at 30 minutes after induction and at 1 hour after surgery start were small at 0.3°C and 0.6°C, the difference of 0.5°C was regarded as clinically important difference during anesthesia (Perl et al., 2014). The fact that core temperature did not decrease from control in prewarming group could be also a clinically important detection (Table 1). Second, FAW was activated from surgery start in control group, nevertheless National Institute for Health and Care Excellence guideline recommended intraoperative warming with FAW device from anesthesia induction in patients having anesthesia for more than 30 minutes.
However, many anesthesiologists in clinical setting are likely to use it from the start of surgery for possibility of dust contamination. In this prewarming method, the effect of prewarming could be dependent on epidural catheter insertion time, so it is possible that heating may not be adequate. However, the strength of this study was the fact that it was done without disrupting the normal anesthesia method.
In conclusion, prewarming applied from the time of entry into the OR, including during epidural catheter insertion, using a FAW device with an underblanket could safely prevent a decrease in patient body temperature caused by redistribution induced by anesthesia without the need for additional preoperative preparation, effort, space, or time. In addition, it also could prevent a decrease in core body temperature during surgery.
Footnotes
Acknowledgments
We express our deepest appreciation to Mrs. Yoko Kondo, who works in Kyushu University Hospital, for their assistance in this study.
Authors' Contributions
K.S.: methodology, formal analysis, and writing—original draft. K.N., R.T., K.O., and K.N.: data curation and writing—review. K.F., M.H. and K.Y.: writing—review and editing, and supervision.
Author Disclosure Statement
No external funding and no competing interests declared.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.