
Abstract
The association between procalcitonin (PCT) level measured 72 hours after cardiac arrest (CA) and neurological outcomes is unknown. We aimed to examine the association of serial PCT levels up to 72 hours with neurological outcomes in patients who underwent targeted temperature management (TTM) after CA. This retrospective observational study included adult comatose patients with CA undergoing TTM (33℃ for 24 hours) at the Chonnam National University Hospital in Gwangju, Korea, between January 2018 and December 2020. PCT levels were measured at admission and at 24, 48, and 72 hours after CA. The presence of early-onset infections (within 7 days after CA) was confirmed by reviewing clinical, radiological, and microbiological data. The primary outcome was poor neurological outcomes at 6 months and was defined by cerebral performance category 3–5. Among the CA survivors, 118 were included and 67 (56.8%) had poor neurological outcomes. The PCT level at 72 hours in the poor outcome group (3.01 [0.88–12.71]) was higher than that in good outcome group (0.56 [0.18–1.32]). The multivariate analysis revealed that the PCT level at 72 hours (adjusted odds ratio 1.241; 95% confidence interval, 1.059–1.455) was independently associated with poor neurological outcomes, showed good performance for poor outcomes (area under the receiver operating characteristic curve of 0.823), and was not associated with early-onset infections. The PCT level at 72 hours after CA can be helpful in predicting prognosis, and it did not correlate with early-onset infections in the study.
Introduction
Postcardiac arrest syndrome (PCAS) is fatal and results in serious complications such as multiple organ failure, mortality, and neurological sequelae (Ro et al., 2013; Kim et al., 2020). The mechanism of PCAS can be explained by ischemia–reperfusion injury, following myocardial dysfunction, coagulopathy, and systemic inflammatory response syndrome (SIRS) (Wada, 2017). SIRS leads to the production of pro-inflammatory cytokines and activation of leukocytes and endothelial cells (Wada, 2017).
Several studies have reported the relationships between biomarkers and PCAS outcomes. High S100 calcium-binding protein B (S-100B) and neuron-specific enolase (NSE) levels were associated with worse neurological prognoses (Stammet et al., 2017; Wihersaari et al., 2019). High neutrophil gelatinase-associated lipocalin levels were associated with in-hospital mortality in patients with PCAS (Elmer et al., 2016). In addition, increased levels of interleukin-6 was associated with worse neurological prognoses (Sugita et al., 2017). In addition, high procalcitonin (PCT) levels, used for diagnosing sepsis, were associated with PCAS prognosis (Annborn et al., 2013; Engel et al., 2013).
Most studies on PCT have focused on the period of 48 hours after cardiac arrest (CA) because cytokine levels increase in the acute phase (24–48 hours) after CA in humans, which are associated with worse outcomes (Adrie et al., 2002). However, as therapeutic hypothermia can slow inflammatory responses, the actual inflammatory response may develop in the rewarming phase or postrewarming period after targeted temperature management (TTM). Moreover, the international guidelines for postresuscitation care require that biomarkers values be considered for up to 72 hours after CA; thus, PCT does not deviate from this category (Nolan et al., 2021). Therefore, PCT levels >48 hours after CA may be associated with neurological prognoses; however, there few studies have investigated the association.
We hypothesized that a high PCT level was associated with poor neurological outcomes in patients with PCAS. Thus, this study aimed to examine the association between PCT levels at four time points (at admission and 24, 48, and 72 hours after CA) and 6-month neurological outcomes. Furthermore, we examined the association between PCT levels and early-onset infections in patients with PCAS.
Methods
Study design and population
This retrospective observational study using prospectively collected data included out-of-hospital CA (OHCA) survivors treated with TTM at the Chonnam National University Hospital in Gwangju, Korea between January 2018 and December 2020. We included adult (aged ≥18 years) comatose OHCA survivors treated with TTM. Furthermore, we excluded patients with interrupted TTM owing to transfer or death, patients who had target temperatures other than 33°C, patients who received either continuous renal replacement therapy or extracorporeal membrane oxygenation support during post-CA care, and patients who did not undergo blood sampling. The Institutional Review Board of Chonnam National University Hospital approved this study (CNUH-2021-141).
Targeted temperature management
Comatose OHCA survivors underwent TTM, in which a target temperature of 33°C was maintained for 24 hours. On completing the TTM maintenance period, the patients were rewarmed to 36.5℃ at a rate of 0.25°C/h. We administered midazolam and remifentanil for analgo-sedation and neuromuscular blockade through continuous infusion during TTM to enhance the efficiency of TTM and reduce metabolic activity in the brain. Amplitude-integrated electroencephalography was used to monitor subclinical seizures, and propofol was administered to control seizures.
Data collection
We obtained data on the following parameters from hospital records: age, sex, body mass index, pre-existing illness, witnessed collapse, bystander cardiopulmonary resuscitation (CPR), first monitored rhythm, etiology of CA, time from collapse to return of spontaneous circulation (ROSC), serum lactate level, glucose level, partial pressure of oxygen (PaO2), partial pressure of carbon dioxide, Glasgow Coma Scale score after ROSC, incidence of coronary angiography, and Sequential Organ Failure Assessment (SOFA) score within the first 24 hours after admission.
Blood samples to determine C-reactive protein (CRP) and PCT levels were collected at admission and 24, 48, and 72 hours after CA. CRP levels were measured using the high-sensitivity nephelometric method (Dade Behring; Marburg, Germany). The lower detection limit for CRP was 0.2 mg/L. PCT levels were quantitated using an immunoassay (Elecsys BRAHMS PCT Procalcitonin, Roche). The minimum and maximum limits of detection were 0.02 and 100 ng/mL, respectively.
Outcome measurement
We assessed the 6-month neurological outcomes after CA through phone interview using the cerebral performance category (CPC) scale (CPC 1, good performance; CPC 2, moderate disability; CPC 3, severe disability; CPC 4, vegetative state; or CPC 5, brain death or death) (Booth et al., 2004). All patients' charts were retrospectively reviewed in detail for evidence and type of infection by two authors (D.K.K. and S.J.R.). Disagreements between prospective diagnosis and retrospective assessment were resolved by consensus (D.K.K., S.J.R., and D.H.L.). Infections were defined according to commonly used criteria and according to previous studies on comatose patients with CA treated with TTM (Mongardon et al., 2011).
Pneumonia was defined by the presence of a new and persistent pulmonary infiltrate on chest radiography associated with either positive quantitative culture of the endotracheal aspirates or in the absence of a bacteriologic sample, in conjunction with purulent sputum and hypoxemia (PaO2/FIO2 < 300). We collected data of patients with early-onset infections, that is, those occurring during the first 7 days from ICU admission. All patients included in this study received a 72-h antibiotic prophylaxis intravenously with piperacillin/tazobactam. The primary outcome was a poor neurological outcome (CPC 3–5), and the secondary outcome was an early-onset infection.
Statistical analysis
Categorical variables are presented as frequencies and percentages and continuous variables as either means ± standard deviation or median values with interquartile ranges depending on the Shapiro–Wilk test results. Categorical variables were compared between groups using the χ2 test with continuity correction in 2 × 2 tables. Continuous variables were compared between groups using independent t-tests or Mann–Whitney U tests.
We applied multivariate logistic regression analysis to assess the associations between CRP and PCT levels and neurological outcomes. Variables with p-values <0.20 in the univariate comparisons were included in the multivariate regression model. We used a backward stepwise approach and sequentially eliminated variables with a threshold p-value >0.10 to build a final adjusted regression model (Supplementary Table S1). CRP and PCT levels at each time point were included in the final model. The results of the logistic regression analysis are presented as odds ratios (ORs) and 95% confidence intervals (CIs). We examined the predictive performance of CRP and PCT levels for poor neurological outcomes using area under the receiver operating characteristic curve (AUC). All analyses were performed using PASW Statistics for Windows, version 18.0 (SPSS, Inc., Chicago, IL) and MedCalc version 19.0 (MedCalc Software, bvba, Ostend, Belgium). Statistical significance was set at p-values <0.05 (two sided).
Results
Patient characteristics
A total of 128 OHCA survivors treated with TTM were identified during the study period. Among them, 118 patients met the inclusion criteria (Fig. 1). The mean age of the patients was 58.7 ± 15.3 years. In addition, 81 (68.6%) patients' OHCAs were witnessed by bystanders, 52 (44.1%) had a shockable rhythm, and 81 (68.6%) had a cardiac etiology. The median time to ROSC was 23.5 (15.8–39.3) minutes. At 6 months, 67 (56.8%) patients had poor neurological outcomes (Table 1).
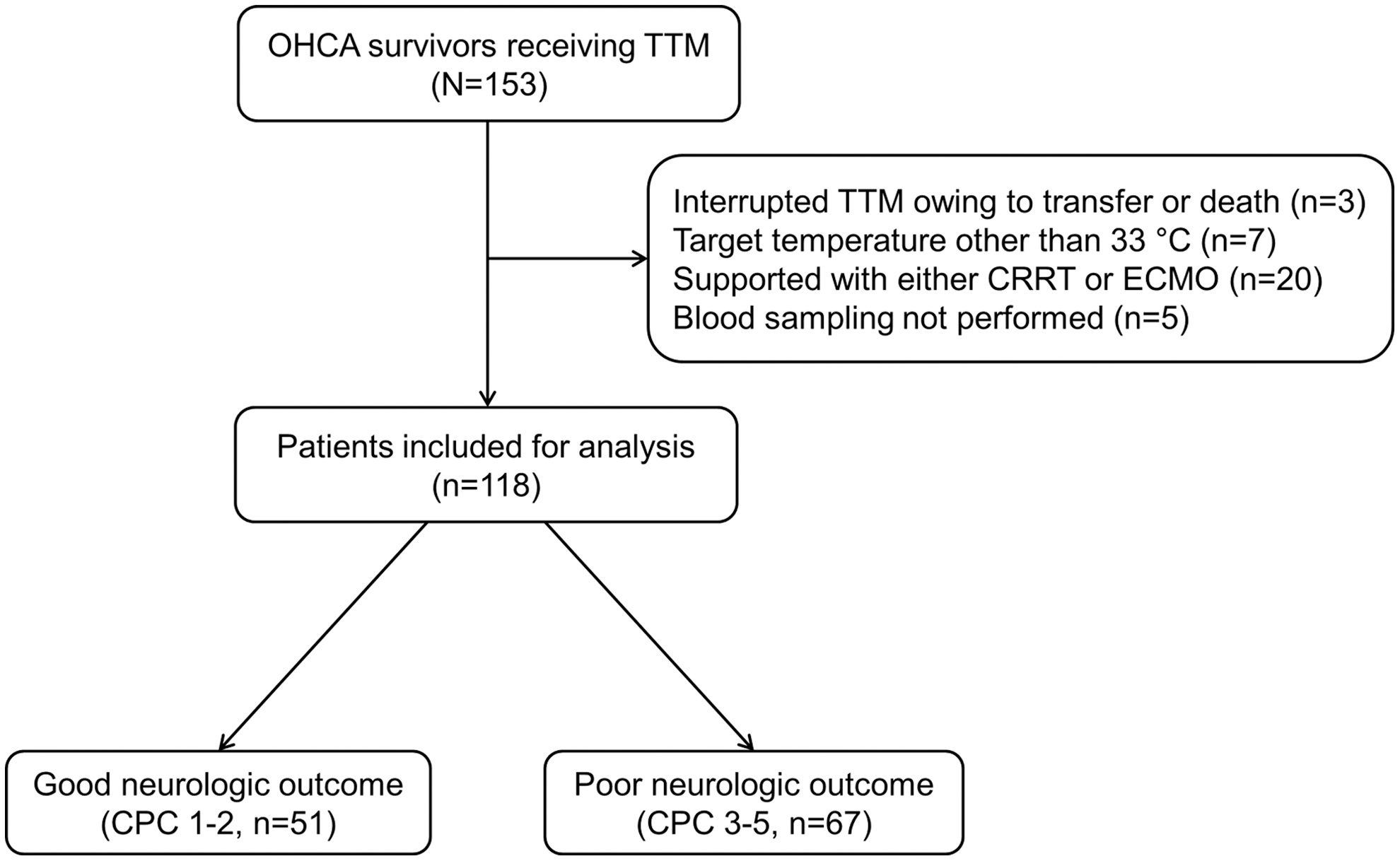
Flow diagram of patient inclusion. CPC, cerebral performance category; CRRT, continuous renal replacement therapy; ECMO, extracorporeal membrane oxygenation; OHCA, out-of-hospital cardiac arrest; TTM, target temperature management.
Comparisons of Baseline Characteristics According to Neurological Outcomes at 6 Months
CPR, cardiopulmonary resuscitation; ROSC, restoration of spontaneous circulation; PaCO2, partial pressure of carbon dioxide; PaO2, partial pressure of oxygen; SOFA, Sequential Organ Failure Assessment.
Clinical characteristics stratified by neurological outcomes
Patients with poor outcomes were older and had lower body mass index; higher incidence of diabetes; lower incidence of witnessed collapse, shockable rhythm, and cardiac etiology; and longer time to ROSC than those with good neurological outcomes. After achieving ROSC, patients with poor outcomes had increased levels of lactate, PO2, and PCO2 and higher SOFA scores than those with good outcomes (Table 1). CRP and PCT levels at admission showed significant differences between those with good and poor outcomes. Moreover, CRP and PCT levels at 24, 48, and 72 hours after CA were higher in patients with poor outcomes than in those with good outcomes (Table 2).
Comparisons of C-Reactive Protein and Procalcitonin Levels According to Neurological Outcomes at 6 Months
CA, cardiac arrest; CRP, C-reactive protein; PCT, procalcitonin.
Association between temperature variables and neurological outcomes
After adjusting for confounders, CRP (adjusted OR [aOR], 1.130; 95% CI, 1.027–1.244) and PCT levels (aOR 1.241; 95% CI, 1.059–1.455) at 72 hours after CA were independently associated with poor neurological outcomes (Table 3). Furthermore, CRP and PCT levels at admission and 24 and 48 hours after CA were not associated with poor neurological outcomes.
Multivariate Logistic Regression Analysis of C-Reactive Protein and Procalcitonin Levels for Poor Neurological Outcomes at 6 Months
Each variable was individually entered into the final model and separately analyzed.
Adjusted for age, shockable rhythm, and time from collapse to return of spontaneous circulation.
CI, confidence interval; OR, odds ratio.
Prognostic performance of PCT levels for poor neurological outcomes at 6 months
In the AUC analysis, PCT levels at 48 hours (0.81; 95% CI, 0.72–0.87) and 72 hours (0.82; 95% CI, 0.74–0.89) after CA showed good performance for predicting 6-month neurological outcomes (Table 4). Among CRP and PCT levels at each point, the PCT level at 72 hours after CA had the highest AUC value for predicting 6-month neurological outcomes.
Area Under the Receiver Operating Characteristic Curve Analysis of C-Reactive Protein and Procalcitonin Levels for Poor Neurological Outcomes at 6 Months
AUC, area under the receiver operating characteristic curve.
CRP and PCT levels for early-onset infections after CA
A total of 50 patients (42.4%) were diagnosed with early-onset (within 7 days) infections. CRP levels at admission and 24, 48, and 72 hours after CA did not differ significantly between patients with and without infections. Similarly, PCT levels at admission and 24, 48, and 72 hours after CA were not associated with early-onset infections (Table 5).
Comparisons of C-Reactive Protein and Procalcitonin Levels According to Early-Onset Infections
Association between PCT levels and poor neurological outcomes in the cardiac etiology group at 6 months
In a subgroup analysis of the cardiac etiology group, PCT levels (aOR, 1.323; 95% CI, 1.075–1.628) at 72 hours after CA were independently associated with poor neurological outcomes (Supplementary Table S2). In the AUC analysis, PCT levels at 48 hours (0.81; 95% CI, 0.70–0.89) and 72 hours (0.83; 95% CI, 0.73–0.91) after CA showed good performance for predicting 6-month neurological outcomes (Supplementary Table S3).
Discussion
Factors that can determine neurological prognosis after CA include findings of brain computed tomography, magnetic resonance imaging, and electroencephalogram; NSE levels, and S-100B levels. Nevertheless, as evidenced by many studies, neurological prognosis after CA cannot be explained by a single factor, and comprehensive explanations of multiple factors can help predict prognosis (Sandroni et al., 2020; Kang et al., 2021). In our multivariate analysis, CRP and PCT levels at 72 hours after CA were associated with 6-month neurological outcomes in OHCA survivors. In the AUC analysis, PCT levels at 72 hours after CA showed good performance and had the highest AUC value for predicting 6-month neurological outcomes.
PCT, a precursor of calcitonin, is released by thyroid C cells at low levels in the plasma under normal physiological conditions. However, in pathological conditions such as bacterial infection, the PCT level considerably increases (Tamaki et al., 2008). Nonthyroid tissues such as the lungs and intestines also produce PCT. As shown in many studies, the PCT level increased even after severe trauma or cerebral infarction, even without bacterial infection (Meisner et al., 2006; Katan et al., 2016). In one study, PCT was identified as an independent risk factor for death owing to cerebral herniation in massive cerebral infarction (Zhang et al., 2018). Similarly, herniation may occur because of cerebral edema after CA, and PCT is considered to be helpful in explaining poor prognosis.
Several studies showed that early serum PCT levels could be used as a diagnostic or prognostic biomarker in patients with PCAS who underwent TTM (Annborn et al., 2013; Engel et al., 2013; Shin et al., 2019). In a systematic review, elevated serum PCT levels at 0–48 hours after CA were associated with poor neurological outcomes (Shin et al., 2019). However, PCT levels at 72 hours after CA were not included in this study. In a prospective study on TTM, PCT levels at 48 hours after CA were significantly higher in patients with poor outcomes than in those with good outcomes (1.69 vs. 0.25 ng/mL) (Annborn et al., 2013).
Although the difference between the two patient groups was similar to that in this study, the PCT level in patients with poor outcomes in this study was higher than that in patients in the previous study. The proportion of shockable rhythm in the previous study was 67.9%, whereas that in this study was 44.1%, which is considered to be a significant difference (Annborn et al., 2013). PCT can be elevated by hypoxic tissue damage, and nonshockable rhythm is considered to have more ischemic insult than shockable rhythm; therefore, it is believed to be related to hypoxia (Preas et al., 2001; Oconnor et al., 2004; Meisner et al., 2006).
In a prospective cohort study where PCT levels were measured at 0, 24, 48, and 72 hours after CA, the PCT level at 24 hours had the highest predictive value (Jang et al., 2019), which is different from the results of our study. The patients included in that study had visited the hospital between 2010 and 2014, and the overall postresuscitation care, including the TTM protocol, was based on the 2010 guideline instead of the 2015 guideline (Jang et al., 2019). Furthermore, in that study, the proportion of bystander CPR was lower than that of witnesses, time for ROSC was longer than that in this study, and neurological outcome was lower than that in recent studies. These various factors may have caused the difference from our study, despite the measuring of PCT level at 72 hours in that study (Jang et al., 2019).
Sepsis is a leading cause of death in patients with PCAS; thus, it is important to identify reliable diagnostic biomarkers to determine the relationship between PCAS and early infection. As TTM regulates temperature, fever during and immediately after TTM is unreliable to confirm the presence of infection. Bacterial culturing also takes time and relies on laboratory tests. Representative laboratory tests related to infection include CRP and PCT. In a multicenter randomized trial (Dankiewicz et al., 2017), CRP and PCT levels at 24, 48, and 72 hours after CA were significantly higher in patients with infections than in those without infections, which differs from the results of this study. In this study, we examined early-onset infection within 7 days after CA, whereas in the previous study, all infections during the entire hospitalization period were investigated (Dankiewicz et al., 2017).
Patients with good neurological outcomes can wean from mechanical ventilation more quickly and can be less exposed to the risk of hematological infection than those with poor neurological outcomes. In other words, elevations in PCT and CRP levels in the early stages of infection may be related to neurological prognosis rather than the effect of infection, and patients with poor neurological outcomes can be inevitably vulnerable to infections during long-term hospitalization. In a study on CRP and PCT in patients with PCAS, CRP and PCT levels were not associated with early-onset infection, consistent with the results of this study (Engel et al., 2013). In another study, PCT levels had limited diagnostic value in early-onset pneumonia after CA and TTM (Stammet et al., 2017). The fact that PCT levels were not associated with infection in the early stages may prove to be reliable in predicting prognosis.
In the multivariate analysis of this study, CRP and PCT levels at 72 hours after CA were associated with poor neurological outcomes, and CRP and PCT levels at admission and 24 and 48 hours after CA were not associated with poor neurological outcomes. This can be explained by the anti-inflammatory effect of TTM. Moderate hypothermia during TTM can blunt inflammatory response by stabilizing cytokines and chemokines and inhibiting complement activation (Bisschops et al., 2014). From the rewarming phase after TTM completion, the inflammatory response is activated and progresses to brain swelling. Thus, inflammatory markers, including CRP and PCT, at 72 hours after CA can be related to neurological outcomes.
This study has some limitations. First, it was a retrospective study performed at a single center; thus, its findings are not immediately generalizable to the overall population. Further multicenter studies with larger samples and prospective designs are necessary to substantiate our findings. Second, because we examined biomarker levels within 72 hours after CA in our study, we could not analyze the relationship between biomarkers beyond 72 hours and neurological prognoses. In the TTM setting in our study, the maintenance period of TTM was 24 hours and the target temperature was 33°C. Thus, the relationship between inflammatory biomarkers and prognosis in other settings could not be analyzed.
Conclusion
The PCT level at 72 hours after CA can be helpful for predicting prognosis of patients with PCAS. In addition, the PCT level at 72 hours after CA did not correlate with early-onset infections.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.