
Abstract
Intraoperative hypothermia is very common and harmful in adult patients undergoing laparoscopic surgery. A variety of active warming systems has received close attention and has been researched by related scholars. However, the relative efficacy of these systems and which active warming system is preferred for such patients remain unclear. The aim of this study was to compare and rank six active warming systems regarding intraoperative warming efficacy in adult patients undergoing laparoscopic surgery. Following the PRISMA 2020 guidelines, relevant randomized controlled trials (RCTs) on the efficacy of different active warming systems in warming adult patients undergoing laparoscopic surgery were searched from five English databases and three Chinese databases. The quality of the studies was assessed using the Cochrane Risk of Bias tool (RoB2). The outcome was the final intraoperative core temperature. We estimated direct effects by using pairwise meta-analysis, estimated relative effects and ranking with the consistency model to conduct an NetworkMeta-Analysis (NMA). We used GRADE (Grading of Recommendations Assessment, Development, and Evaluation) to assess the certainty of the evidence. Sensitivity analysis was performed to test the robustness of the results. This study is registered with PROSPERO, with number CRD42022309057. In total, 19 RCTs involving 6 active warming systems and comprising 1364 patients were included in this NMA. The NMA once again confirmed the validity of forced-air warming (FAW) systems compared with other active warming systems, and further showed that underbody FAW was associated with more remarkable warming efficacy in different types of FAW systems. NMA was used to perform an exhaustive comparison of the warming efficacy of six active warming systems and indicated that underbody FAW was most likely to be the most effective warming system in adult patients undergoing laparoscopic surgery; however, considering the sparsity of the network, our results should be cautiously interpreted. Furthermore, a large number of high-quality RCTs comparing the warming efficacy of different competitive active warming systems are needed.
Introduction
Perioperative hypothermia, defined as a core temperature <36°C (Hooper et al., 2009, 2010), is a common complication with adverse effects and has an incidence of 37.5–77.2% during the perioperative period (Constantine et al., 2015; Tsuchida et al., 2016; Emmert et al., 2018). With the development of minimally invasive surgery, laparoscopic surgery is widely used because of its advantages of minimal trauma, quick recovery, few complications, and wide indications (Qin et al., 2020). However, the current literature suggests that the rates of hypothermia are similar in laparoscopic and open surgery (Pu et al., 2014; Chen et al., 2021) and the incidence of hypothermia in laparoscopic surgery is as high as 50–90% (Scott et al., 2015). Even mild hypothermia can cause adverse complications, such as, increased mortality rates (Sessler, 2001; Quiroga et al., 2010), cardiac conduction block and arrhythmia, susceptibility to infection at the surgical site, poor wound healing and postoperative pain (Burns et al., 2009), delayed drug metabolism (Leslie et al., 1995), postoperative shivering (Schmied et al., 1996), and prolonged recovery.
Perioperative heat loss occurs through radiation, conduction, convection, and evaporation (Perlman et al., 2016). During anesthesia and surgery, the effective way to maintain the body temperature of adult patients undergoing laparoscopic surgery is to minimize heat loss by reducing radiation and convection from the skin (Campbell et al., 2015), evaporation from exposed surgical areas and cooling caused by the introduction of cold intravenous fluids, irrigation fluids (Lynch et al., 2010; Simegn et al., 2021), or cold carbon dioxide gases injected into the abdomen (Cumin et al., 2022). Preventing perioperative hypothermia by active warming systems has proven to be an effective temperature management strategy.
Various perioperative warming devices in the existing studies applied to adult patients undergoing laparoscopic surgery are broadly divided into passive insulation that acts to minimize heat loss from the body through increased insulation, such as, cotton blankets (warmed or unwarmed) (Leslie and Sessler, 2003), quilts (Pu et al., 2014), or surgical drapes (Baradaranfard et al., 2019), and active warming systems, including forced-air warming (FAW) (Matsuzaki et al., 2003), carbon-fiber resistive heating (CFRH) (De Witte et al., 2010), radiant warming systems (RWA) (Kadam et al., 2009), circulating-water mattresses (CWM) (Matsuzaki et al., 2003), fluid warming (FW) (Luo et al., 2020), and warmed, humidified CO2 (WHCO2) (Jiang et al., 2019).
Traditional meta-analyses involving, but not limited to, adult laparoscopic surgery patients, have evaluated the effects of various types of active cutaneous warming systems (Galvao et al., 2010; Nieh and Su, 2016; Zhang et al., 2020). In addition, other active warming systems based on distinct mechanisms (such as fluid warmers; WHCO2) were covered in separate reviews and compared with room temperature fluids (Campbell et al., 2015) or cold, dry CO2 (Birch et al., 2016; Balayssac et al., 2017; Dean et al., 2017). These studies all used traditional pairwise meta-analyses, which can only compare a given warming system with another warming system or a nonactive control; such pairwise meta-analyses rely on head-to-head comparison trials between two different competing active warming systems. In the absence of direct randomized evidence, it is difficult to identify with confidence the most effective active warming systems based on only the traditional pairwise meta-analysis method.
With increasingly active warming systems being applied to adult patients undergoing laparoscopic surgery, it is necessary for practitioners to know the relative efficacy and cost-efficacy of these systems to make a scientific decision because if, for some reason, the most effective warming systems may not be available, information on the second- and third-best treatments is also important (Salanti et al., 2011). Network meta-analysis can solve this problem scientifically by combining the direct and adjusted indirect estimates to obtain a comparative efficacy that can be precisely estimated and interpreted (Hoaglin et al., 2011; Tonin et al., 2017). Therefore, this was a pragmatic and clinically valuable study using Network Meta-Analysis (NMA) to evaluate the effect of different active warming systems, which can provide evidence-based guidance and a potential feasible and efficient nursing care protocol for the prevention of intraoperative hypothermia in adult patients undergoing laparoscopic surgery.
Methods
This NMA was conducted in accordance with PRISMA 2020 updated guidance for reporting systematic reviews (Supplementary Appendix SA1). This study is registered with PROSPERO, No. CRD42022309057.
Inclusion and exclusion criteria
Population
Participants older than 18 years of age undergoing laparoscopic surgery under general anesthesia were included in the study. Patients with a body temperature ≥37.5°C or ≤36°C, patients with hypothyroidism, or patients with preoperative hypothermia did not meet the inclusion criteria.
Intervention
Original studies using any kind of active warming system of unlimited types were included, and studies using two or more different types of warming systems in combination were excluded.
Control
Original studies were eligible if the control group received passive insulation (i.e., blanket, quilt, pad, or drapes), or active warming systems differing from that in the intervention group. However, studies in which the control group did not use any insulation measures were not ineligible.
Outcomes
Original studies reporting the primary outcomes (final intraoperative core temperature) were eligible. If the study had multiple measuring points after intervention, effect sizes were primarily calculated with the end of surgery value. The core temperature was obtained by measuring the temperature of the eardrum, distal esophagus, nasopharynx, or rectum. We recorded the core temperature as close to the immediate end of surgery as possible for all analyses. (If no information immediately after the end of the operation was available, we preferred the time closest to the end of the operation.)
Study design
This NMA only included randomized controlled trials (RCTs). We excluded studies reporting insufficient data and duplicate published RCTs.
Search methods
Two authors independently searched the literature in PubMed, Embase, Web of Science, The Cochrane Library, CINAHL Plus with Full Text (EBSCO platform), and three Chinese databases (China National Knowledge Infrastructure, WanFang, and WeiPu) from inception to February 6, 2022, and included all languages. We also reviewed the reference lists of all eligible articles and existing meta-analyses related to this topic and tracked references to the included literature; moreover, we also searched published, unpublished, and ongoing RCTs in international trial registers. The search strategy was personalized for each database. The key search terms of (laparoscopy/“laparoscopic surger*”), (warm*/rewarming/heat*/“forced-air warming”/“carbon fiber”/“resistive warming”/“radiant warm*”/“radiant heaters” “fluid warm*”/“infusions, intravenous”/“intravenous fluid*”/incubator/“circulating water mattress”/“carbon dioxide”/blanket*/quilt/drapes), and RCTs (RCTs/trial) were a combination of medical subject heading terms (MeSH) and entry terms. The search strategy is described in Supplementary Table S1.
Study selection
All the searched records were imported into EndNote X9 to eliminate duplicate studies. Then, the two authors who received formal training in systematic evaluation worked independently to identify RCTs that met the inclusion criteria and then extracted the data individually. To further evaluate the eligibility of potential studies, we obtained the full texts, and two reviewers resolved disagreements by discussion and also involved a third reviewer, if necessary, to reach consensus.
Quality appraisal
Version 2.0 of the Cochrane Collaboration's risk-of-bias tool provides an Excel file with macros to facilitate the author's evaluation. All included studies were assessed independently by two authors involving bias arising from randomization process, bias of deviation from established intervention, bias of missing outcome data, bias of outcome measurement, and bias of selective reporting of results, and the risk of bias for each item was categorized as “low risk,” “some concerns,” or “high risk.” The overall risk of bias generally corresponds to the worst risk of bias in any of the domains (Sterne et al., 2019). Disagreements between the two authors were resolved by other professionals related to the subject matter.
Data extraction
The data to be extracted from each selected RCT included the first author, publication year, country, type of surgery, sample size, interventions (site, duration), outcome indicators, site and time points of the intraoperative temperature measurement, and core temperature results.
Data synthesis and statistical analysis
First, we used STATA software (version 17.0; MP) to perform pairwise meta-analysis when an outcome was reported in two or more studies, and the study provided enough data to allow the calculation of effect sizes. All outcomes of the included studies were continuous variables and were expressed in the same units; thus, network estimates were expressed using mean differences (MD) with a 95% confidence interval (CI). The heterogeneity was evaluated by the I2 test; if the I2 value was >50%, the study was considered to be substantially heterogeneous, and a random-effects model was applied to analyze the data (Higgins et al., 2011).
Second, an NMA was conducted using the “Network” command of STATA software. We drew the network diagram using the “network map” command. Inconsistency was assessed by global inconsistency based on a χ2 test, and local node-splitting analysis when direct evidence came from direct comparisons and multiarm trials (Dias et al., 2010). A value of p ≥ 0.05 was considered to indicate no statistically significant inconsistency, and the consistency model was used (White et al., 2012). The relative warming efficacy of the different warming systems is presented as a league table. We calculated the surface under the cumulative ranking curve (SUCRA) percentages to estimate the relative rankings of each warming system (Salanti et al., 2011). A SUCRA value can range from 0% to 100%; the larger the SUCRA value is, the better the rank of the warming systems. We used a comparison-adjusted funnel plot to evaluate the publication bias, and then we applied Begg's test and Egger's test to assess the asymmetry of the funnel plots (Begg and Mazumdar, 1994; Egger et al., 1997). To assess the robustness of the results, a sensitivity analysis was performed by repeating the NMA excluding high-risk studies.
Evaluation of evidence quality
We assessed the certainty of evidence contributing to network estimates of the main outcomes with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework (Salanti et al., 2014). We used the CINeMA (Confidence in Network Meta-Analysis), which is freely available to evaluate six domains that affect the level of confidence in the NMA results: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence (Nikolakopoulou et al., 2020; Papakonstantinou et al., 2020). Finally, judgments across the domains are summarized into a single confidence rating, the certainty of the evidence of each paired comparison as high, moderate, low, or very low (Puhan et al., 2014; Brignardello-Petersen et al., 2018).
Results
Study outcomes
We comprehensively searched 1788 relevant articles including 1397 from English databases, 390 from Chinese databases, and 1 from references. After removal of duplicates and obviously irrelevant records, we screened 89 full-text studies to further evaluate their eligibility, of which 71 articles were excluded because they did not meet the inclusion criteria. An additional article was identified by manually searching the reference lists of included trials in relevant reviews. Ultimately, a total of 19 included studies (16 studies from English databases and 3 studies from Chinese databases) were included in this NMA involving 6 active warming systems. The PRISMA flowchart for the study search is given in Figure 1.
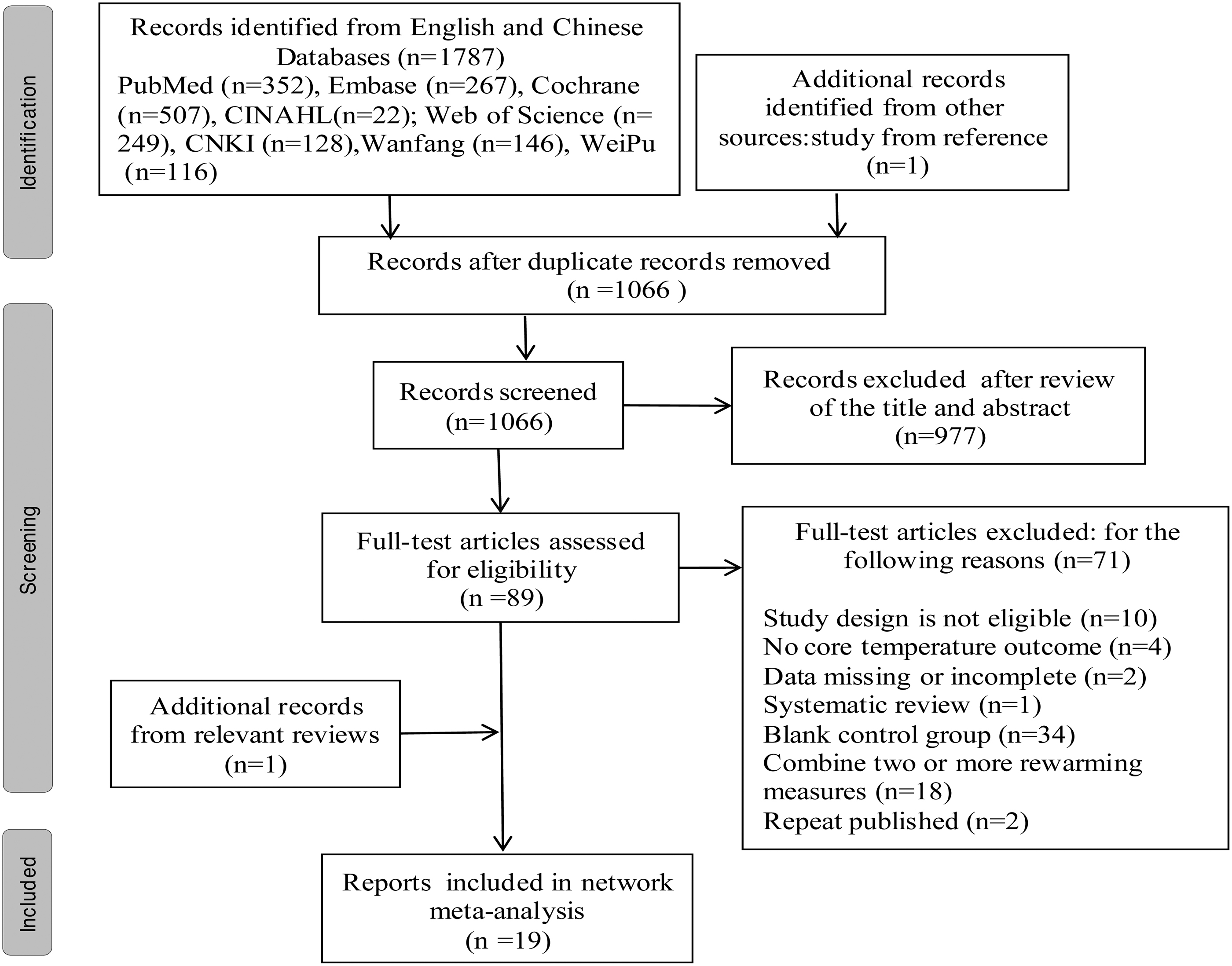
The PRISMA flowchart for the study search.
Characteristics of the included studies
A total of 19 RCTs involving 11 countries and 1364 adult patients undergoing laparoscopic surgery who received 6 types of active warming systems were included.
The specific warming systems are as follows: (1) FAW: there are two types according to the site of action: overbody forced-air warming (OFAW; n = 15), underbody forced-air warming (UnFAW; n = 4); (2) CFRH (n = 2); (3) RWS (n = 2); (4) FW (n = 4); (5) CWM (n = 1); (6) WHCO2 (n = 1); (7) control group (n = 13).
The number of participants ranged from 8 to 467; the site of core temperature measurements was esophageal (n = 9), nasopharyngeal (n = 5), tympanic (n = 4), or rectal (n = 1); the application duration of the warming systems was preoperative, intraoperative, or pre- and intraoperative; and the application temperature of the warming systems ranged from 37°C to 46°C. The detailed information on the included studies are listed in Supplementary Table S2, and references for the included studies is listed in Supplementary Appendix SA2 (Camus et al., 1995; Campos-Suárez et al., 1997; Matsuzaki et al., 2003; Wong et al., 2004; Gu, 2009; Kadam et al., 2009; De Witte et al., 2010; Pu et al., 2014; Hou and Han, 2017; Zou et al., 2017; Su and Nieh, 2018; Boayam et al., 2018; Baradaranfard et al., 2019; Jiang et al., 2019; Lee et al., 2020; Luo et al., 2020; Gulia et al., 2022; Hara et al., 2022; Zhang et al., 2022).
Risk of bias assessment
Overall, 10 studies were judged as having a low risk of bias, 8 studies were judged as having some concerns risk of bias, and 1 study was judged as having a high risk of bias. The study by Gu (2009) was judged as having a high risk of bias because it has some concerns in three domains (the “Randomization process” domain, “Deviations from intended interventions” domain, and “Bias in selection of the reported result” domain). Among the eight studies, four studies had some concerns in the “Randomization process” domain, and the other four studies had some concerns in both the “Bias in selection of the reported result” domain and the “Bias in selection of the reported result” domain. The quality of the included studies is given in Supplementary Figure S1.
Meta-analysis results
Traditional pairwise meta-analysis
Stata17.0 software was used for direct comparative analysis of two or more studies. We adopted a random-effects model because the data were significantly heterogeneous.
The direct comparisons of the different active warming systems and the control are presented in Supplementary Figures S2 to S4. OFAW (n = 9, weighted mean difference (WMD) = 0.38, 95% CI [0.24 to 0.52], I2 = 84.9%), FW (n = 3, WMD = 0.46, 95% CI [−0.14 to 1.06], I2 = 99.1%), UnFAW (n = 2, WMD = 0.98, 95% CI [0.33 to 1.64], I2 = 98.9%), apart from FW, all had statistically significant active effects compared with the control group. The direct comparisons of active warming systems and OFAW are presented in Supplementary Figures S5 to S8. CFRH (n = 2, WMD = −0.14, 95% CI [−0.50 to 0.22], I2 = 54.2%), pooled analysis showed that there was no significant difference compared with OFAW; RWS (n = 2, WMD = 0.24, 95% CI [0.06 to 0.42], I2 = 0%), FW (n = 2, WMD = 0.11, 95% CI [0.03 to 0.20], and I2 = 18.8%), pooled analysis showed that there was a statistically significant difference in favor of OFAW; UnFAW (n = 2, WMD = −0.34, 95% CI [−0.53 to 0.16], I2 = 0%), pooled analysis showed that it was significantly better than OFAW.
Network meta-analysis
Among the 19 included studies, 15 studies were two-arm trials, and 4 studies were three-arm trials. The network diagram is given in Figure 2. Each node represents a warming system and their size is proportional to the number of trials comparing this warming system with any other. The lines link each pair of direct comparisons, and the width of the lines is proportional to the number of trials comparing the two warming systems. The network diagram indicated that the number of trials of control and OFAW were in the top 2, and comparisons containing control and OFAW were frequent. The consistency model was selected for the subsequent NMA because, the results test of consistency showed χ2 = 4.14, p = 0.763 (p > 0.05), and the p-values in the node-splitting analyses were >0.05.
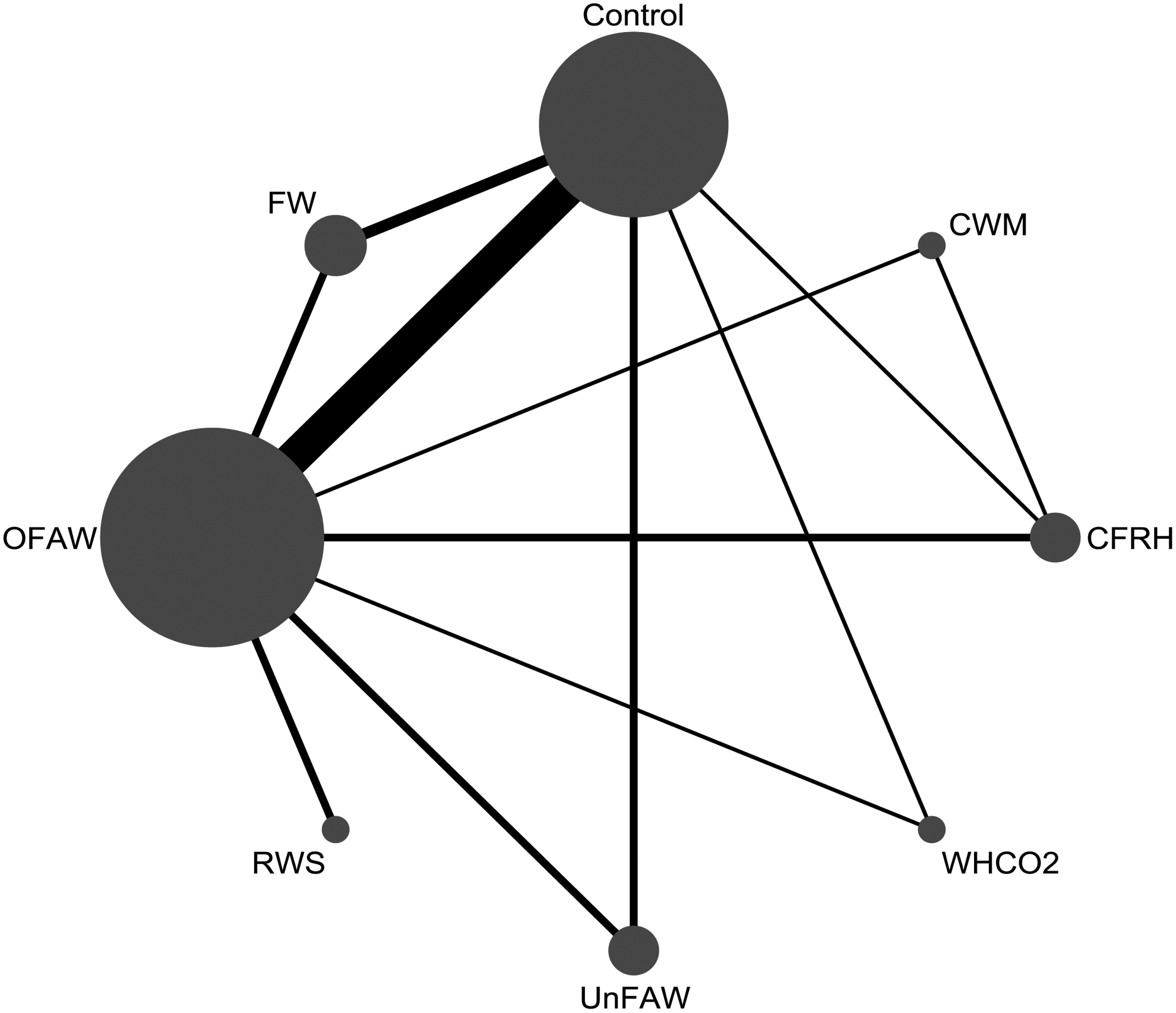
Network diagram for the comparison of different warming systems. CFRH, carbon-fiber resistive heating; CWM, circulating-water mattress; FW, fluid warming; OFAW, overbody forced-air warming; RWS, radiant warming system; UnFAW, underbody forced-air warming; WHCO2, warmed, humidified carbon dioxide.
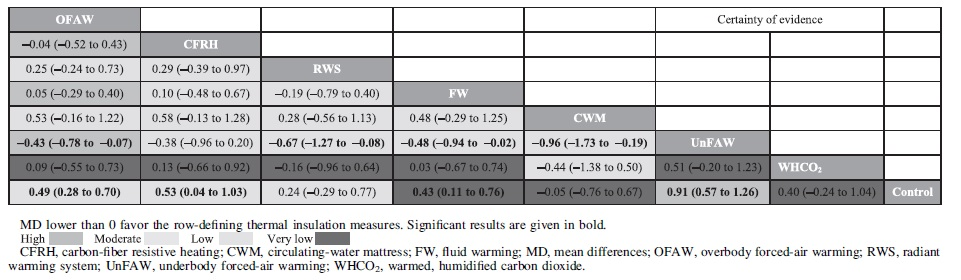
The relative efficacy of the different warming systems is presented as a league table in Table 1. The analysis revealed that UnFAW had statistically significant efficacy in adult patients undergoing laparoscopic surgery relative to OFAW (MD = −0.43, 95% credibility interval (CrI) = −0.78 to −0.07), RWS (MD = −0.67, 95% CrI = −1.27 to −0.08), FW (MD = −0.48, 95% CrI =−0.94 to −0.02), CWM (MD = −0.96, 95% CrI = −1.73 to −0.19), and the control (MD = −0.91, 95% CrI = −1.26 to −0.57). OFAW (MD = 0.49, 95% CrI = 0.28 to 0.70), CFRH (MD = 0.53, 95% CrI = 0.04 to 1.03), FW (MD = 0.43, 95% CrI = 0.11 to 0.76), and UnFAW (MD = 0.91, 95% CrI = 0.57 to 1.26), all had significant effects relative to the control, and there were no significant differences among the other comparisons.
Relative Warming Efficacy of Different Warming Systems
The SUCRA of the warming efficacy of the different warming systems is given in Figure 3. The results indicated that the ranking from best to worst was as follows: UnFAW, most likely to rank as 1 (96.9%); CFRH, rank 2 (66.7%); OFAW, rank 3 (63.6%); FW, rank 4 (56%); WHCO2, rank 5 (51.7%); RWS, rank 6 (36.5%); CWM, rank 7 (16%); and control (blanket, quilt, or drapes), rank 8 (12.6%).
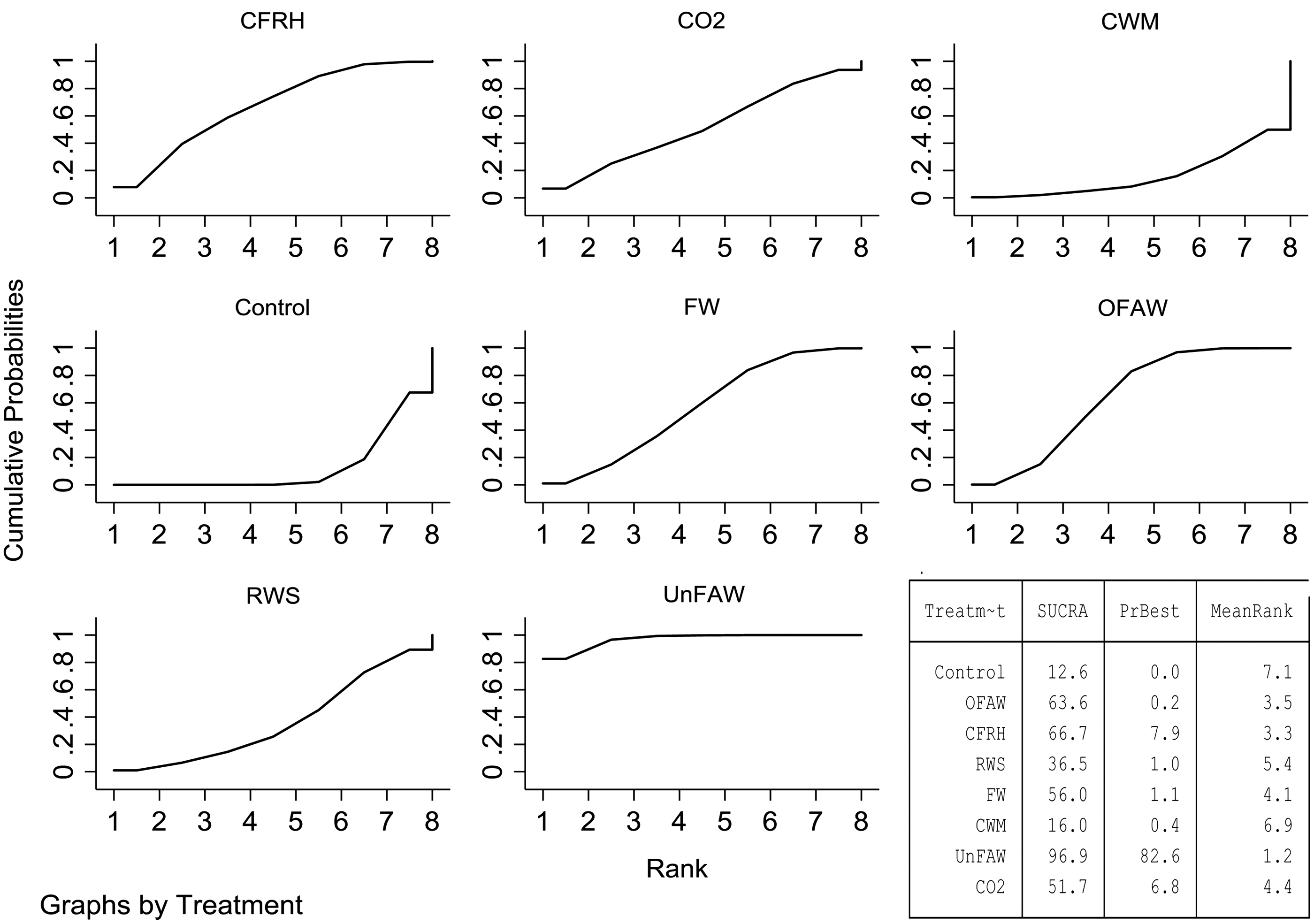
SUCRA of the efficacy of different warming systems. SUCRA, the surface under the cumulative ranking curve.
Publication bias
In general, the comparison-adjusted funnel had a symmetric distribution except for several small studies that were distributed outside the inverted funnel, and all statistical tests of funnel plot asymmetry were statistically insignificant, which indicated that there was no evidence of publication bias. The comparison-adjusted funnel plot is given in Supplementary Figure S9.
Sensitivity analyses
A sensitivity analysis was performed to explore whether these high-risk studies affected the results. We performed a repeat NMA, in which only studies with low to moderate risk were included. The relative efficacy of different active warming systems was similar, suggesting that high-risk studies did not significantly affect our results (Supplementary Table S3).
Evaluation of GRADE evidence quality
We used the CINeMA to assess the certainty of the evidence that showed moderate to very low confidence, essentially owing to indirectness, imprecision, and heterogeneity (Supplementary Table S4).
Discussion
To the best of our knowledge, this is the first NMA incorporating indirect and direct comparisons to comprehensively compare the warming efficacy of six active warming systems in adult patients undergoing laparoscopic surgery. In summary, we combined the NMA results with the results of a direct comparison of traditional meta-analyses, and the evidence of very low to moderate certainty showed that UnFAW was most likely to be the most effective active warming system, followed by CFRH, OFAW, FW, WHCO2, and CWM.
Our results confirmed the efficacy of FAW in adult patients undergoing laparoscopic surgery. Similarly, FAW application in major surgeries is now recommended by guidelines (NICE, 2016) and some meta-analyses also suggested that FAW was more effective than other active warming systems (Galvao et al., 2010; Nieh and Su, 2016; Zhang et al., 2020). Furthermore, we found that in two different types of FAW blankets currently, UnFAW, which warms the patient from below, had the highest possibility of being the most effective active warming system, and that OFAW, which warms the patient from above, was most likely to rank third. The mechanism of FAW heat transfer is based on radiation and conduction.
Hot air is generated by a motor and delivered to the single-use forced-air blanket through a hose and yields a circulating flow on the part of the body it covers (Bräuer et al., 2002; Kabbara et al., 2002), thus increasing the total body heat to compensate for the body temperature decrease owing to heat dissipation (Simegn et al., 2021); surprisingly, this may completely eliminate heat loss from the skin surface and convert the heat loss to heat gain (Brauer et al., 2009). The reason why UnFAW was superior to conventional OFAW and was the most likely effective active warming system in adult patients undergoing laparoscopic surgery is that the efficacy of active cutaneous warming systems depends upon the size of the surface area covered by the patient's body. In laparoscopic surgeries, almost the whole abdomen will be exposed because of surgical procedures. UnFAW can cover the entire body and provide continuous heat in patients, but some heat is lost because the abdominal surgical area cannot be covered, leading to relative reduction in the insulation effect of OFAW. Our finding was consistent with the results of retrospective study of Miyazaki et al. (2017).
UnFAW is also safe because a modest heat intensity is evenly distributed over a large surface area, and the shunt of hot air never warms dependent surfaces in the supine position, thus avoiding the dangerous combination of heat and pressure (Sessler, 2016). Although FAW is by far the most commonly employed system, presumably because it is effective, safe, and easy to use (Sessler, 2016), in the German 2017 updated guidelines for avoiding perioperative hypothermia pointed out that some attention should be given in clinical practice, such as, avoiding directly blowing warm air onto a patient without a blanket; avoiding heating areas with poor circulation; using blankets that match the manufacturer (Torossian et al., 2019); and using two layers of cotton drapes or a blanket cover between the patient and warming blanket to avoid direct contact caused burns (Pham and Ravanfar, 2014). In addition, the cost of use should be considered because blankets are disposable.
The SUCRA of the efficacy indicated that carbon-fiber resistive heating (CFRH) was most likely to rank second (66.7%) among the six different active warming systems. CFRH is a device that converts electrical energy into heat energy through a semiconductor carbon-fiber fabric by using a 15-V direct current (John et al., 2014). The mechanism is patient surface contact heat conduction and an advantage of CFRH over other active warming systems is that a warm pad under the patient's body is used in combination with a heating blanket over the patient to provide stereoscopic thermal insulation. Both the pad and the blanket can be adjusted independently and flexibly to cover large amounts of surface area in almost any surgical position and heat numerous cover segments (Fanelli et al., 2009); as a result, more total heat at a given heat transfer rate will be transferred to patients (Negishi et al., 2003).
Furthermore, CFRH is likely to prove considerably less expensive than forced air in routine use because the blanket is reusable by washing or sterilizing (Hofer et al., 2005); however, it directly contacts the patient's skin, which may leads to burns (Dewar et al., 2004). It is worth noting that for CFRH, in the RCTs of Matsuzaki et al. (2003) (n = 8), and the RCTs of De Witte et al. (2010) (n = 9), there were no significant differences between CFRH and OFAW. Similarly, some meta-analyses also confirmed that this concluded efficacy of CFRH is comparable with that of OFAW (Galvao et al., 2010; Nieh and Su, 2016).
However, NMA showed that the rank of CFRH may be superior to that of OFAW, probably because for the NMA, data were pooled and compared after adjustment; that is to say, the conclusions of direct comparison and indirect comparison are integrated, and there were slight mutual influences among various warming systems. Nevertheless, this finding was based only on 2 RCTs and 17 sample sizes, and there are limited data on the use of CFRH in adult patients undergoing laparoscopic surgery; therefore, this result should be interpreted with caution. In the future, more high-quality RCTs are needed to confirm this conclusion.
Cooled intravenous fluid administration may constrict blood vessels and can be a significant source of convective heat loss, especially when large volumes are infused (Forstot, 1995). FW supplies heat by inserting the infusion catheter into the package type heating fixture, which can heat up the liquid to near human body temperature. However, the traditional meta-analysis of this study showed no statistically significant differences between the fluid warmer system and the control group and exhibited high heterogeneity (Supplementary Fig. S2); this finding consistent with a review in The Lancet (Sessler, 2016). A possible reason is that the ability of fluid warming to prevent intraoperative hypothermia is mainly dependent on the volume infused (Barthel and Pierce, 2012).
A previous study showed no preventive effect of intraoperative intravenous fluid warming on intraoperative hypothermia in patients given intravenous fluid volumes of <1 L (Andrzejowski et al., 2010). This may also explain the high heterogeneity of traditional meta-analyses (Baradaranfard et al., 2019; volume infused ∼0.9 L; Zou et al., 2017; volume infused ∼1.6 L; Luo et al., 2020; volume infused ∼2 L). Therefore, following NICE guidelines and considering both the warming efficacy and potential economic savings, we suggest that for patients with a short operation time and <1 L infusion volume, a warming cabinet can be routinely used to preheat the fluid; otherwise, a commercial real-time fluid warmer system should be recommended for use during the operation.
In laparoscopic surgery, the diffusion of CO2 gas may be responsible for peritoneal desiccation injuries and cooling that may lead to intraoperative hypothermia (Xu et al., 2021). Consequently, WHCO2 has been considered to reduce the occurrence of intraoperative hypothermia. However, controversy still exists regarding the efficacy of the warming effect of humidified and warmed CO2 compared with cold, dry CO2 in a number of meta-analyses to date (Birch et al., 2016; Hakeem et al., 2016; Balayssac et al., 2017; Dean et al., 2017). Meanwhile, in this study, the result of warmed and humidified CO2 was based on only one RCT and needs to be interpreted with caution because this limited sample might have exaggerated the effect. As such, more high-quality RCTs comparing this system with other competitive active heating systems are needed to validate the efficacy.
The RWS is a system that acts directly on the rich arteriovenous anastomosis area (i.e., face, hands or feet) and utilizes infrared B energy to warm the patient (Lee et al., 2004) The mechanism of action is that these anastomoses can dilate in response to local heating and allow applied heat energy to be transferred directly to the core via the circulation (Bergersen et al., 1995). Traditional meta-analysis of this study showed that the RWS is significantly less effective than OFAW for thermal insulation in laparoscopic surgery and there is no heterogeneity, probably related to the fact that RWS only heats a limited area and heat transfer may be reduced as the position is raised (Wong et al., 2004).
Thus, studies have suggested that the RWS could be used as an alternative or adjunct to FAW with savings in terms of disposable costs for some minor surgeries that are short in duration (Torrie et al., 2005), and one fact that must be admitted is that the RWS is especially applicable to plastic, orthopedic, or burn surgeries where infection control is of paramount concern because the system does not produce unnecessary air flow and can reduce radiant heat losses (Lee et al., 2004). However, it may not be suitable for some patients with poor perfusion because it is difficult to heat as the reduced blood flow over the heated site means that less heat can be transferred back to the core (Wong et al., 2004).
A CWM exchanges heat by conduction underneath the patient through a nondisposable heated mattress connected to a circulating pump, and the mattress maintains temperature using hot water circulation (Nieh and Su, 2016). However, its heat transfer may be limited by the relatively low water temperature that avoids causing “burns” and poor perfusion in dependent areas (Gendron, 1980), which is also probably why it ranks last in terms of warming efficacy. However, the conclusions of the network analysis of CWM were derived from only one 3-arm study comparing OFAW, CFRH, and CWM, and the comparison with other active warming systems is indirect evidence, which is obviously not convincing enough. As such, more high-quality RCTs compared with other competitive active heating systems are needed to validate the efficacy.
There were some strengths in our NMA: (1) We performed an exhaustive comparison of the efficacy of six different competitive active warming systems in adult patients undergoing laparoscopic surgery by the evidence currently available, and the differences among them were distinguished according to the rank probability; (2) Only RCTs comparing single warming systems with different heating mechanisms were included, which implies that the included studies had a rigorous study design and could accurately identify the efficacy of each active warming system; (3) The evidence body was evaluated by GRADE, which can help the clinical decision maker make an informed judgment about how to use the findings.
Admittedly, several limitations should be recognized in our NMA: (1) Although we have carefully searched all the warming systems used on adult patients undergoing laparoscopic surgery, the number of RCTs is still limited, and we judged the network to be sparse to some extent, which may cause hesitation in the conclusions. (2) There were some other active warming systems, such as the thermal suit, which were not included in our study owing to the lack of data on core temperatures.
It is a challenging task to take active and effective measures to prevent hypothermia during surgery. Our NMA compared and ranked the efficacy of different active warming systems for intraoperative warming in adult patients undergoing laparoscopic surgery, and indicated that underbody FAW systems was most likely to be the most effective warming system. The results might provide evidence-based information to inform medical decision-making. However, some active warming systems were evaluated in few studies or small sample sizes. For example, there was only one three-arm RCT examining the efficacy of WHCO2 (Jiang et al., 2019) and CWM (Matsuzaki et al., 2003). The sample sizes used in the existing studies for the efficacy of CFRH were both <10 (Matsuzaki et al., 2003; De Witte et al., 2010). Therefore, many rigorously designed RCTs with larger sample sizes are still needed to compensate for the defects of indirect comparisons. Meanwhile, the initial and ongoing costs of these active warming systems, as well as their affordability to patients and to Medicare, also require further in-depth analysis in the future.
Conclusion
Our NMA compared the warming efficacy of six different active warming systems in adult patients undergoing laparoscopic surgery. The results showed that FAW is still the preferred and effective active warming system, and in two different types of FAW blankets, UnFAW had the highest possibility of being the most effective active warming system, followed by CFRH, OFAW, FW, WHCO2, the RWS, and the CWM. Therefore, surgical team professionals should be encouraged to apply active warming devices with the highest ranking first. Moreover, considering the sparsity of the network, our results should be cautiously interpreted, and a large number of high-quality RCTs comparing the efficacy of different competitive active warming systems are needed.
Footnotes
Authors' Contributions
Y.-N.T. and Z.-W.W. conceived and designed the study and take responsibility for the integrity of the data and accuracy of the data analysis. Y.-N.T. and W.-Y.G. contributed to data extraction, quality evaluation, certainty of evidence and the writing of the article. Y.-N.T. contributed to the statistical analysis. X.-R.T. and Z.-W.W. supervised the data analyses and contributed to the critical review of the intellectual content of the article. All authors contributed to data collection, data analysis, and data interpretation and reviewed and approved the final version.
Data Sharing
The analytic dataset is available on request by contacting the corresponding author.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.