
Abstract
Hypothermia affects coagulation, but the effect of hypothermia on fibrinolysis is not clarified. Imbalance in the fibrinolytic system may lead to increased risk of bleeding or thrombosis. Our aim was to investigate if resuscitated cardiac arrest patients treated with hypothermia had an unbalanced fibrinolysis. A prospective cohort study, including 82 patients were treated with hypothermia at 33°C ± 1°C after out-of-hospital cardiac arrest. Blood samples were collected at 24 hours (hypothermia) and at 72 hours (normothermia). Samples were analyzed for fibrin D-dimer, tissue plasminogen activator (tPA), plasminogen, plasminogen activator Inhibitor-1 (PAI-1), thrombin-activatable fibrinolysis inhibitor (TAFI), and an in-house dynamic fibrin clot formation and lysis assay.Compared with normothermia, hypothermia significantly increased plasminogen activity (mean difference = 10.4%, 95% confidence interval [CI] 7.9–12.9), p < 0.001), PAI-1 levels (mean difference = 275 ng/mL, 95% CI 203–348, p < 0.001), and tPA levels (mean difference = 1.0 ng/mL, 95% CI 0.2–1.7, p = 0.01). No differences between hypothermia and normothermia were found in TAFI activity (p = 0.59) or in the fibrin D-dimer levels (p = 0.08). The fibrin clot lysis curves showed three different patterns: normal-, flat-, or resistant clot lysis curve. At hypothermia 45 (55%) patients had a resistant clot lysis curve and 33 (44%) patients had a resistant clot lysis curve at normothermia (p = 0.047). Comatose, resuscitated, cardiac arrest patients treated with hypothermia express an inhibited fibrinolysis even after rewarming. This could potentially increase the thromboembolic risk. ClinicalTrials.gov ID: NCT02258360.
Introduction
Patients who have suffered from cardiac arrest have a high morbidity and mortality (Grasner et al, 2021). To reduce the mortality, it has been recommended to treat comatose survivors after cardiac arrest with hypothermia (Nolan et al, 2021). However, recently the landmark study, “Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest,” demonstrated that treatment with hypothermia did not lead to a lower mortality than patients treated with normothermia (Dankiewicz et al, 2021). Subsequently, the current International Liaison Committee on Resuscitation (ILCOR) guidelines recommend preventing hyperthermia, but remarks that it remains uncertain whether subpopulations may benefit from treatment with hypothermia (Granfeldt et al, 2021). Furthermore, the guidelines notice that comatose cardiac arrest patients who are hypothermic should not be actively rewarmed (Granfeldt et al, 2021).
The hemostatic and fibrinolytic system sustains an essential balance between clot formation and lysis in the healthy individual (Chapin and Hajjar, 2015). Previous studies investigating fibrinolysis in cardiac arrest patients indicate that during the cardiac arrest a hyperfibrinolysis develops with endogenous excessive clot breakdown (Duvekot et al, 2015; Gando and Wada, 2019; Gando et al, 1997; Viersen et al, 2012; Wada et al, 2013), but this might be followed by hypofibrinolysis postcardiac arrest (Duvekot et al, 2015; Viersen et al, 2012). Several studies state that low temperature inhibits coagulation activity (Dirkmann et al, 2008; Kettner et al, 2003; Whelihan et al, 2014; Wolberg et al, 2004), but the effect of low temperature on fibrinolysis has not been clarified. This knowledge is important since imbalance in the fibrinolytic system may lead to hyperfibrinolysis or fibrinolytic shutdown, conditions that potentially increase the risk of bleeding or thrombosis (Adelborg et al, 2021).
The aim of the present study was to investigate if resuscitated cardiac arrest patients treated with hypothermia at 33°C ± 1°C had an unbalanced fibrinolysis.
Methods
The present posthoc study recruited patients from the randomized controlled trial entitled “Targeted Temperature Management for 48 vs 24 Hours and Neurologic Outcome After Out-Of-Hospital Cardiac Arrest: A Randomized Clinical Trial” (Kirkegaard et al, 2017). From February 2013 through May 2015, 82 patients were enrolled at the Intensive Care Unit, Aarhus University Hospital, Denmark, and randomized to either 24 or 48 hours of hypothermia. The inclusion criteria were sustained return of spontaneous circulation (ROSC) after out-of-hospital cardiac arrest with a presumed cardiac cause, Glasgow Coma Score below 8 and age ≥18 years. The main exclusion criteria were unwitnessed asystole, >4 hours from cardiac arrest to initiation of treatment with hypothermia, severe persistent cardiogenic shock, baseline cerebral performance category 3–4, terminal illness, pregnancy, and a known pre-existing coagulopathy. A complete list of exclusion criteria can be seen in the protocol article (Kirkegaard et al, 2016).
This trial treated comatose survivors of out-of-hospital cardiac arrest with either 24 hours (42 patients) or 48 hours (40 patients) of hypothermia at 33°C ± 1°C. Hypothermia was applied by surface or intravascular feedback cooling systems and the subsequently rewarming was conducted at a rate of maximum 0.5°C/h. Until normothermia was achieved, patients were sedated, intubated, and mechanically ventilated.
Written informed consent was obtained from next of kin and general practitioner and from the patients themselves, if they became capable of giving informed consent. The study was approved by the Central Denmark Region Committees on Health Research Ethics (20110022) and the Danish Data Protection Agency. The cohort and data in Tables 1 and 2 have previously been described in detail by Jeppesen et al (2017).
Baseline Characteristics of the 82 Out-of-Hospital Cardiac Arrest Patients
Time from cardiac arrest to ROSC.
ROSC, return of spontaneous circulation; SAPS II, Simplified Acute Physiology Score II.
Laboratory Investigations and Medications in the 82 Out-of-Hospital Cardiac Arrest Patients Treated with Hypothermia at 33°C ± 1°C
The reference interval applies to both male and female patients.
Upon admission to the Intensive Care Unit.
Heparin was given prehospital or upon admission.
Usage of bivalirudin ended 16–20 hours before obtaining the 24-hour sample.
ADP, adenosine diphosphate receptor; APTT, activated partial thromboplastin time; CRP, C-reactive protein; INR, International Normalized Ratio; Q, quartile.
Blood samples
This study included blood samples that were collected at admission (admission sample) and subsequently 24 hours (hypothermia) and 72 hours (normothermia) after target temperature was reached. Only standard but no research blood samples were obtained at the admission, due to the need for obtaining informed consent. The 3.2% citrate anticoagulation tubes were centrifuged at 20°C at 3300 g for 25 min within 30 min of sample collection, and the plasma was immediately separated and stored at −80°C until further analysis.
International normalized ratio (INR), activated partial thromboplastin time (APTT), thrombin time, fibrinogen (functional, Claus's method), plasminogen (activity), and fibrin D-dimer were analyzed using CS2100i (Sysmex, Kobe, Japan), blood lactate employing ABL800 FLEX (Radiometer, Brønshøj, Denmark) and C-reactive protein using Cobas 6000 (Roche, Mannheim, Germany). The following ELISA Kits were applied: tissue plasminogen activator (tPA) (TECHNOZYM t-PA EDTA ELISA Kit; Technoclone GmbH, Vienna, Austria), plasminogen activator Inhibitor-1 (PAI-1) (TECHNO-ZYM PAI-1 Antigen ELISA Kit; Technoclone GmbH), and thrombin-activatable fibrinolysis inhibitor (TAFI) (IMUCLONE Total TAFI ELISA; Sekisui Diagnostics, LLC, Lexington, MA, USA). All samples were analyzed in duplicate and reanalysed if the coefficient of variation were above 10%. Each sample was analyzed according to the manufacturer's instructions at 37°C.
Fibrin clot formation and lysis were determined in duplicate employing an in-house assay using tissue factor (diluted 1:5000) and tPA (concentration 116 ng/mL) as previously described. (Neergaard-Petersen et al, 2018) The following parameters were calculated: lag phase (seconds), peak (maximum absorbance, arbitrary unit), time to peak (seconds), 50% clot lysis time (seconds), and area under the curve (AUC). The clot lysis curves were categorized as flat if the AUC were less than 50 (more than 80% below the lowest normal reference value). The clot lysis curves were categorized as resistant if the clot were formed but no lysis was observed within the running time of 80 minutes.
The manufacturer's reference interval was used as a reference interval for tPA, plasminogen, PAI-1, and TAFI. Reference interval for the fibrin clot formation and lysis assay was established by Neergaard-Petersen et al (2018).
Statistics
Descriptive data are presented as median with lower and upper quartile (Q1–Q3). Dichotomized data are presented as number and proportions (%). The normal distribution was checked using Q–Q plots. The data were log transformed if it made a better model fit. The paired or nonpaired t-test were used if the data were normally distributed, otherwise the Wilcoxon signed-rank test was used for paired nonparametric data. Statistical significance was defined as p < 0.05. All statistical analyses were performed using STATA® version 16 (Stata Corp LP, College Station TX, USA). Graphics are performed using STATA or GraphPad PRISM® 6.0 (GraphPad Software, Inc., San Diego, CA, USA).
Results
In total, 82 cardiac arrest patients were included. In seven patients the 72-hour sample was not collected due to death before the 72-hour blood sample or due to logistic challenges.
The median age was 60 years (range: 18–79 years) and the majority were male (87%). The most frequent comorbidity was hypertension. The majority received bystander cardiopulmonary resuscitation and had a primary shockable rhythm (Table 1). After the cardiac arrest, the main part of the patients received aspirin and low-molecular-weight heparin (LMWH), and approximately half of the patients received adenosine diphosphate receptor inhibitors (Table 2). The main part of the cohort had a coronary angiography performed upon arrival to hospital (98%) and 37 patients (45%) were treated with percutaneous coronary intervention (Table 1). No patients had severe bleeding complications during the admission at the Intensive Care Unit.
Fibrinolysis
Upon admission, before the target temperature was reached, patients had a substantially increased fibrin D-dimer (Fig. 1).
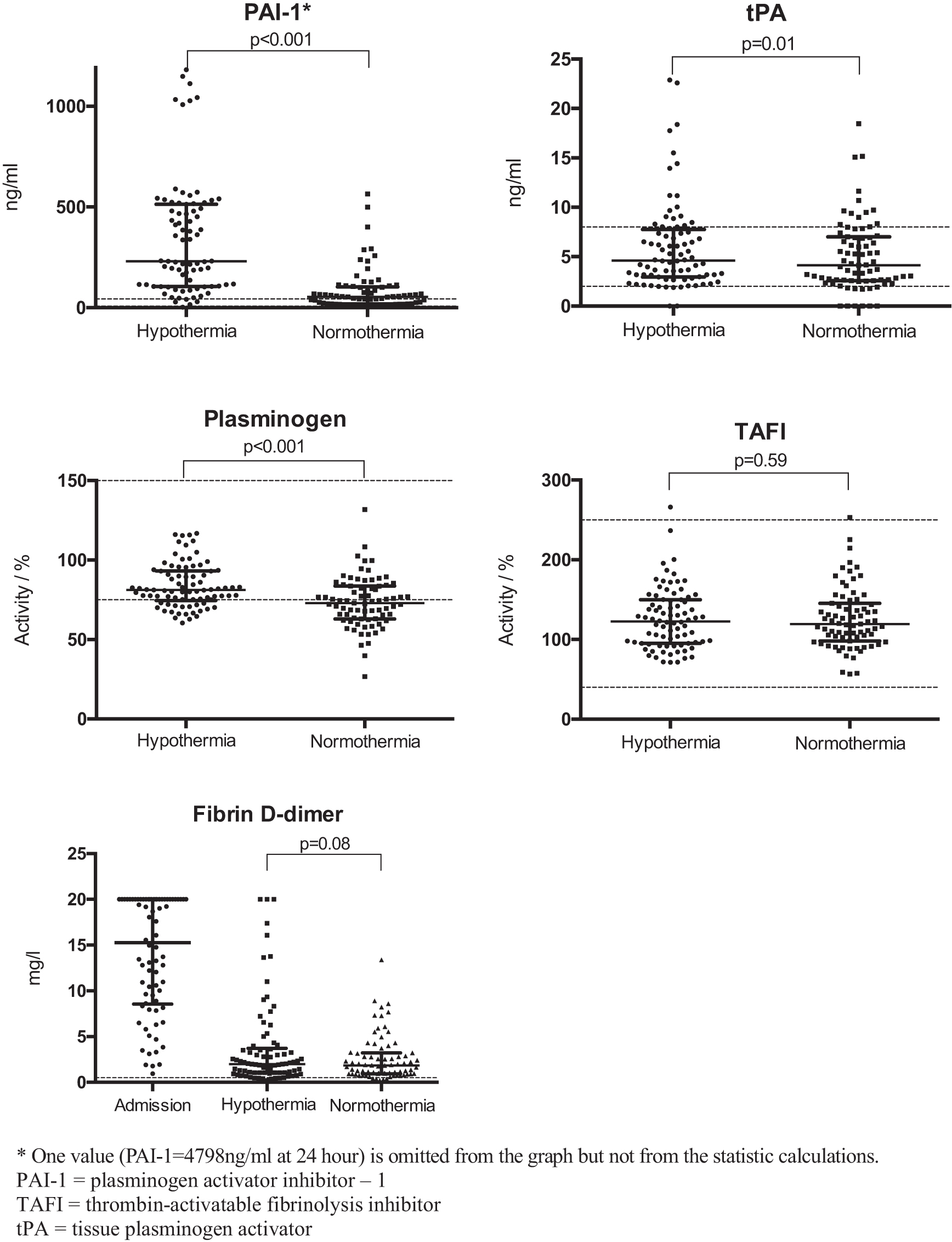
Fibrinolytic variables at hypothermia at 33°C ± 1°C (24 hours) and normothermia (72 hours). The black line is the median with interquartile range and the dotted line is the reference interval.
The patients were treated with hypothermia for either 24 or 48 hours after the cardiac arrest. Thus, when the 24-hour sample was obtained, the duration of hypothermia had been the same in all patients. At normothermia, in the 72-hour sample, no difference was found in plasminogen activity, t-PA level, PAI-1 level, TAFI activity, or fibrin D-dimer level (all p-values ≥0.16) between patients treated with 24 or 48 hours of hypothermia. Since the different durations of hypothermia did not seem to influence the patients at normothermia, data obtained from the 72-hour sample were pooled.
Compared with normothermia, hypothermia significantly increased plasminogen activity (mean difference = 10.4%, 95% confidence interval [CI] 7.9–12.9, p < 0.001), PAI-1 levels (mean difference = 275 ng/mL, 95% CI 203–348, p < 0.001), and tPA levels (mean difference = 1.0 ng/mL, 95% CI 0.2–1.7, p = 0.01), Figure 1. No differences were found in TAFI activity (p = 0.59) or in the fibrin D-dimer level (p = 0.08) between hypothermia and normothermia (Fig. 1).
Fibrin clot lysis
The clot lysis curves showed three different patterns: normal clot lysis curve, flat clot lysis curve, or resistant clot lysis curve. At hypothermia (24-hour sample), a normal clot lysis curve was observed in 19 patients (23%), a flat clot lysis curve in 18 patients (22%), and a resistant clot lysis curve in 45 patients (55%). At normothermia (72-hour sample), a normal clot lysis curve was observed in 31 patients (41%), a flat clot lysis curve in 11 patients (15%), and a resistant clot lysis curve in 33 patients (44%). Fibrin clot lysis data are presented in Table 3.
Fibrin Clot Lysis in 82 Patients Treated with Hypothermia at 33°C ± 1°C After Cardiac Arrest
Chi-square-test for no association, p = 0.04.
Reference interval established in 66 individuals >40 years, published by Neergaard-Petersen et al (2018).
AU, arbitrary unit; AUC, area under the curve.
During hypothermia, patients with a flat clot lysis curve had a statistically significant increased INR (p = 0.01) and APTT (p = 0.01) compared with patients with a normal clot lysis curve. However, there was no difference in thrombin time, fibrinogen, or platelet count between patients with a flat clot lysis curve and patients with a normal clot lysis curve (all p-values >0.44). No differences were found in platelet count, fibrinogen, APTT, INR, or thrombin time between patients with a resistant clot lysis curve and patients with a normal clot lysis curve (all p-values >0.10). Fibrinolysis markers in relation to the pattern of the clot lysis curves are presented in Figure 2.

Fibrinolysis variables in relation to the clot lysis curves in 82 patients 24 hours postcardiac arrest. The clot lysis curves are categorized as either flat, resistant, or normal. The black line is the median with interquartile range and the dotted line is the reference interval.
No patients received tranexamic acid before, during, or after the cardiac arrest. Approximately half the patients received unfractionated heparin (UFH) prehospital or upon admission to hospital, and the main part of the patients received LMWH at a prophylactic dose once a day. During hypothermia, nine of the 82 patients (11%) had prolonged thrombin time (above upper reference limit at 21 seconds) indicating the presence of heparin, however seven out of these patients had a thrombin time just between 21 and 25 seconds (Fig. 2). Of these nine patients with a prolonged thrombin time, three patients had a flat clot lysis curve. The 30-day mortality was 30% (25 patients out of 82 patients included). During hypothermia, 17 (68%) of the dying patients had a resistant clot lysis curve, whereas 4 (16%) patients had a flat clot lysis curve and 4 (16%) patients had a normal clot lysis curve.
Discussion
We investigated the effect of hypothermia on fibrinolysis in resuscitated out-of-hospital cardiac arrest patients. Generally seen, we found evidence of hypofibrinolysis during hypothermia, demonstrated by a substantially increased PAI-1, a high number of patients with resistant clot lysis, and the clot lysis curves persisted being resistant in 44% of the cardiac arrest patients after rewarming.
No studies have previously investigated fibrinolysis during hypothermia in humans following cardiac arrest. Gong et al (2013) investigated fibrinolysis in 16 pigs resuscitated after cardiac arrest. The pigs were randomized to either normothermia or 12 hours of hypothermia at 33°C. Contrary to our findings, they found that treatment with hypothermia reduced the tPA and PAI-1 levels compared with normothermia (Gong et al, 2013). However, even though pigs and humans have many similarities, the knowledge from pigs may be problematic to transfer to humans.
Only few studies have investigated the effect of low temperature on fibrinolysis. Watts et al examined hypothermic (33–36.9°C) versus normothermic trauma patients using thromboelastography (TEG), and found no differences in the fibrinolysis index (Watts et al, 1998). However, TEG is not sensitive for fibrinolysis (Larsen and Hvas, 2021), thus they might have overlooked an effect. Nielsen and George (2011) investigated the effect of low temperature by the use of an in-house-modified thromboelastography assay using plasma from six healthy individuals. They reported that the velocity of lysis was significantly reduced when the analyses were performed at 27°C compared with 37°C, but demonstrated no significant difference between 33°C and 37°C (Nielsen and George, 2011). Thus, this is contrary to the present study, which demonstrated that hypothermia even at 33°C may inhibit fibrinolysis.
Few studies have investigated fibrinolysis in cardiac arrest patients not treated with hypothermia. Viersen et al (2012) reported that about half of the cardiac arrest patients developed hyperfibrinolysis measured by standard thromboelastometry (ROTEM) (Viersen et al, 2012). Likewise, Duvekot et al (2015) found hyperfibrinolysis measured by ROTEM, tPA, PAI-1, and TAFI in cardiac arrest patients. Both studies examined the cardiac arrest patients during the cardiac arrest or shortly after ROSC. In the present study, we were not able to collect research samples upon admission due to the missing consent from next of kin, but we found evidence for a high fibrin D-dimer upon admission, as could be consistent with hyperfibrinolysis.
We found evidence that following cardiac arrest some survivors develop a hypofibrinolytic condition. Gando et al compared samples from cardiac arrest patients upon admission with samples obtained after 24 hours. They reported a high tPA level upon arrival but a low level after 24 hours, whereas PAI-1 levels were significantly higher 24 hours after the cardiac arrest than at admission (Gando et al, 1997). Their findings are in accordance with our findings, where tPA levels were within the reference interval and PAI-1 levels were above the reference interval 24 hours postcardiac arrest. Wada et al (2013) studied the fibrinolytic system during the postcardiac arrest syndrome. They measured fibrinolytic markers in 52 resuscitated out-of-hospital cardiac arrest patients and compared with 15 healthy controls (Wada et al, 2013). The cardiac arrest patients exhibited similar levels of TAFI but higher levels of alfa2 plasmin inhibitor complex levels and PAI-1 than healthy individuals, indicating that the postcardiac arrest syndrome inhibits fibrinolysis (Wada et al, 2013).
Hence, previous studies state that some patients develop hyperfibrinolysis during the cardiac arrest, but postcardiac arrest during the ischemia and reperfusion injury [also termed “the postcardiac arrest syndrome” (Gando and Wada, 2019)], some patients seem to develop hypofibrinolysis. Thus, both the postcardiac arrest syndrome as well as hypothermia might inhibit fibrinolysis. Further studies are needed to be able to clarify whether this impairment of the fibrinolytic system leads to an increased risk of thrombosis.
Using the clot lysis assay, we observed that the clot lysis curves showed three different patterns: a flat, a normal, or a resistant clot lysis curve. It is likely that the use of UFH and LMWH might cause flat clot lysis curves. In the present study, approximately half the patients received UFH prehospital or upon admission to hospital, thus, a time frame of roughly 24 hours from UFH administration to the 24-hour sampling. Hence, the main part of the UFH has been eliminated at the time of sampling. LMWH at a prophylactic dose was used in the main part of the patients and often administered in the late afternoon or evening. Blood samples were collected at a given time frame after the target temperature was reached, thus some of the samples may have been collected shortly after the administration of LMWH. However, only few patients had prolonged thrombin time, thus, we do not have an explanation for the remaining 83% of patients with a flat clot lysis curve in the 24-hour sample. Tranexamic acid leads to resistant clot lysis curves (Modrau et al, 2020), but no patients in the present study received tranexamic acid.
Previously, Larsen et al (2021) have described flat or resistant clot lysis curves in patients with sepsis. They reported an association between the curve pattern and APTT. These findings are in concordance with the present study, where a flat clot lysis curve was associated with significantly longer APTT and INR. Furthermore, we found that patients with flat or resistant curve patten had significantly higher PAI-1 levels than those with normal clot lysis curves. These findings expand the findings in the sepsis study by Larsen et al that reported a high PAI-1 level in the lysis-resistant curves (Larsen et al, 2021).
The strength of the present study is that it compared paired blood samples drawn from hypothermic and normothermic patients, and this study thereby contributes to reveal the impact of temperature on fibrinolysis.
Some limitations have to be considered. Due to the time frame between sampling, there is a risk that the impact on fibrinolysis caused by postcardiac arrest syndrome has changed over time. If the fibrinolysis was enhanced in the normothermic samples compared with the hypothermic samples, due to a decreasing impact of the postcardiac arrest syndrome, we might overestimate the inhibitory effect of hypothermia on fibrinolysis. Due to lack of consent at admission, no fibrinolytic parameters were measured at the admission sample. Thus, it is possible that anticoagulation drugs or other treatments during or shortly after the cardiac arrest might have affected the results. Furthermore, this study included out-of-hospital cardiac arrest patients with a presumed cardiac origin only. Thus, it is uncertain if these results would apply to other hypothermic patients. Moreover, all analyses were performed at 37°C, even though the 24-hour samples were drawn during hypothermia.
Conclusion
Out-of-hospital cardiac arrest patients treated with hypothermia at 33°C exhibit a hypofibrinolytic state that may persist after rewarming. This hypofibrinolysis might contribute to an increased risk of thromboembolic complications.
Footnotes
Acknowledgments
The present study was investigator initiated. The authors specially thank research bioanalysts Vivi Bo Mogensen and Mai Stenulm Therkelsen for performing the analyses.
Authors' Contributions
A.N.J., C.D., H.K., A.M.G., and A.-M.H. conceived and designed the study and A.N.J. collected the data. A.N.J. and A.-M.H. directed the analyses and A.N.J. preformed the statistical analyses. A.N.J. produced a draft of the article, and C.D., H.K., A.M.G., and A.-M.H. revised it. All authors have approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was financially supported by the following: Doctor Sofus Carl Emil Friis and wife Olga Doris Friis' Grant, The Danish Heart Foundation, Aase and Ejnar Danielsen's Foundation, Kathrine and Vigo Skovgaard's Foundation, The A.P. Møller Foundation for the Advancement of Medical Science and Torben and Alice Frimodt's Foundation. The foundations had no role in the design, the conduct of the study or the decision to submit the article for publication.