
Abstract
The members of the International Liaison Committee on Resuscitation (ILCOR) Advanced Life Support Task Force have written a comprehensive summary of trials of the effectiveness of induced hypothermia (IH) or targeted temperature management (TTM) in comatose patients after cardiac arrest (CA). However, in-depth analysis of these studies is incomplete, especially since there was no significant difference in primary outcome between hypothermia versus normothermia in the recently reported TTM2 trial. We critically appraise trials of IH/TTM versus normothermia to characterize reasons for the lack of treatment effect, based on a previously published framework for what to consider when the primary outcome fails. We found a strong biologic rationale and external clinical evidence that IH treatment is beneficial. Recent TTM trials mainly included unselected patients with a high rate of bystander cardiopulmonary resuscitation. The treatment was not applied as intended, which led to a large delay in achievement of target temperature. While receiving intensive care, sedative drugs were likely used that might have led to increased neurologic damage as were antiplatelet drugs that could be associated with increased acute stent thrombosis in hypothermic patients. It is reasonable to still use or evaluate IH treatment in patients who are comatose after CA as there are multiple plausible reasons why IH compared to normothermia did not significantly improve neurologic outcome in the TTM trials.
Introduction
The members of the International Liaison Committee on Resuscitation (ILCOR) Advanced Life Support Task Force recently published a summary of trials which evaluated the effectiveness of induced hypothermia (IH) or targeted temperature management (TTM) in comatose patients after resuscitation from cardiac arrest (CA) (Granfeldt et al, 2021). However, in-depth analysis of these studies is incomplete, especially as the pooled estimate of the effect of IH on the primary outcome in these studies showed no significant difference between hypothermia versus normothermia.
In 2016, Pocock and Stone published a framework for considering trial results when a significant difference in the primary outcome between treatment groups was not observed (Pocock and Stone, 2016). Below, we use a modification of this method to comment on the ILCOR systematic review. Although initial trials (Bernard et al, 2002; Hypothermia after Cardiac Arrest Study Group, 2002) and a recent large French trial reported that TTM improves outcomes in patients resuscitated from CA, the clinical community seems to have preferentially weighted the lack of benefit observed in the TTM (Nielsen et al, 2013) and TTM2 (Dankiewicz et al, 2021) trials. Therefore, we focus our observations on the latter two trials.
Is There A Strong Biologic Rationale That Favors Treatment?
Restoration of flow (called reperfusion) causes the release of circulating inflammatory molecules that lead to cellular injury (Madathil et al, 2016; Yellon and Hausenloy, 2007). In the brain after CA, cell injury is associated with activation of N-methyl-D-aspartate receptors; opening of mitochondrial permeability transition pores (MPTPs); impaired oxygen and glucose metabolism; release of free radicals, reactive oxygen species (ROS) and cytokines; and seizures (Allan and Rothwell, 2001; Barone and Parsons, 2000; Chan, 2001; Green and Shuaib, 2006; Love, 1999; Matsuo et al, 1995). In the heart after CA, cell injury is associated with activation of glutamate receptors; opening of MPTPs; impaired oxygen and glucose metabolism; microvascular obstruction; myocardial dysfunction; and arrhythmia (Yellon and Hausenloy, 2007).
This cell injury includes rapid release of ROS, cytokines, adhesion molecules, and leukocytes, (Adrie et al, 2004; Bisschops 2004; Adrie et al, 2002; Bottiger et al, 2002; Gando et al, 1999; Niemann et al, 2009; Shyu et al, 1997) upregulation of DNA, activation of protein kinases, and endothelial dysfunction (Adrie et al, 2002; Bottiger et al, 1995; Gando et al, 1997; Laurent et al, 2005). The latter plays a key role in myocardial necrosis (Miura and Tanno, 2012; Peart and Headrick, 2009). During ischemia and reperfusion, ROS lead to oxidative injury to fatty acids and cell membranes, lipid peroxidation, and damage to proteins (Becker, 2004). Cell injury begins within seconds and peaks within 15 minutes of reperfusion (Ambrosio and Tritto, 1999; Khalid and Ashraf, 1993; Zweier et al, 1987).
IH reduces global reperfusion injury in the brain and heart via a variety of protective mechanisms (Sun et al, 2019). The neuroprotective effect is attributed to reduced metabolic rate, reduced formation of free radicals, reduced inflammation, inhibition of excitotoxicity and reduction in apoptosis. Multiple studies in small and large animal models of CA demonstrate that hypothermia to a target temperature of 34°C or less improves outcome compared to normothermia (Arrich et al, 2021; Che et al, 2011; Chen et al, 2013; Gong et al, 2015a; Gong et al, 2015b; Hu et al, 2011; Kuboyama et al, 1993; Leonov et al, 1990; Li et al, 2012; Safar et al, 1996; Sterz et al, 1991; Tadler et al, 1998; Weinrauch et al, 1992; Zhao et al, 2015).
Also, multiple studies in small and large animal models of CA demonstrate that rapid hypothermia improved outcome compared to delayed hypothermia (Arrich et al, 2021; Che et al, 2011; Kim et al, 2016; Kuboyama et al, 1993; Yuan et al, 2017). In humans resuscitated from CA, briefer time from restoration of spontaneous circulation (ROSC) to target temperature is associated with significantly reduced likelihood of death or neurologic impairment (Lee et al, 2017; Nagao et al, 2010; Schock et al, 2016; Uribarri et al, 2015). Collectively, these data demonstrate that there is a strong biologic rationale that favors treatment with rapid IH to 34°C or less to reduce morbidity and mortality after resuscitation from CA.
Is There Some Indication of Potential Benefit?
A key difference among trials of IH or TTM in patients resuscitated from CA is time to each trial's intended target temperature. Holzer and Sterz reported time from ROSC versus core temperature (Fig. 1): (Hypothermia after Cardiac Arrest Study Group, 2002) in the intervention group, this was ∼8 hours to 34°C. Generally, subsequent trials have reported time from randomization to target temperature rather than time from ROSC. This difference is important, as there is a large variation in the estimated time from ROSC to target temperature in each trial (Table 1). Note that the TTM2 investigators stated in their methods article that “rapid cooling in the hypothermia group will be achieved by means of cold fluids and cooling devices” (Dankiewicz et al, 2019).
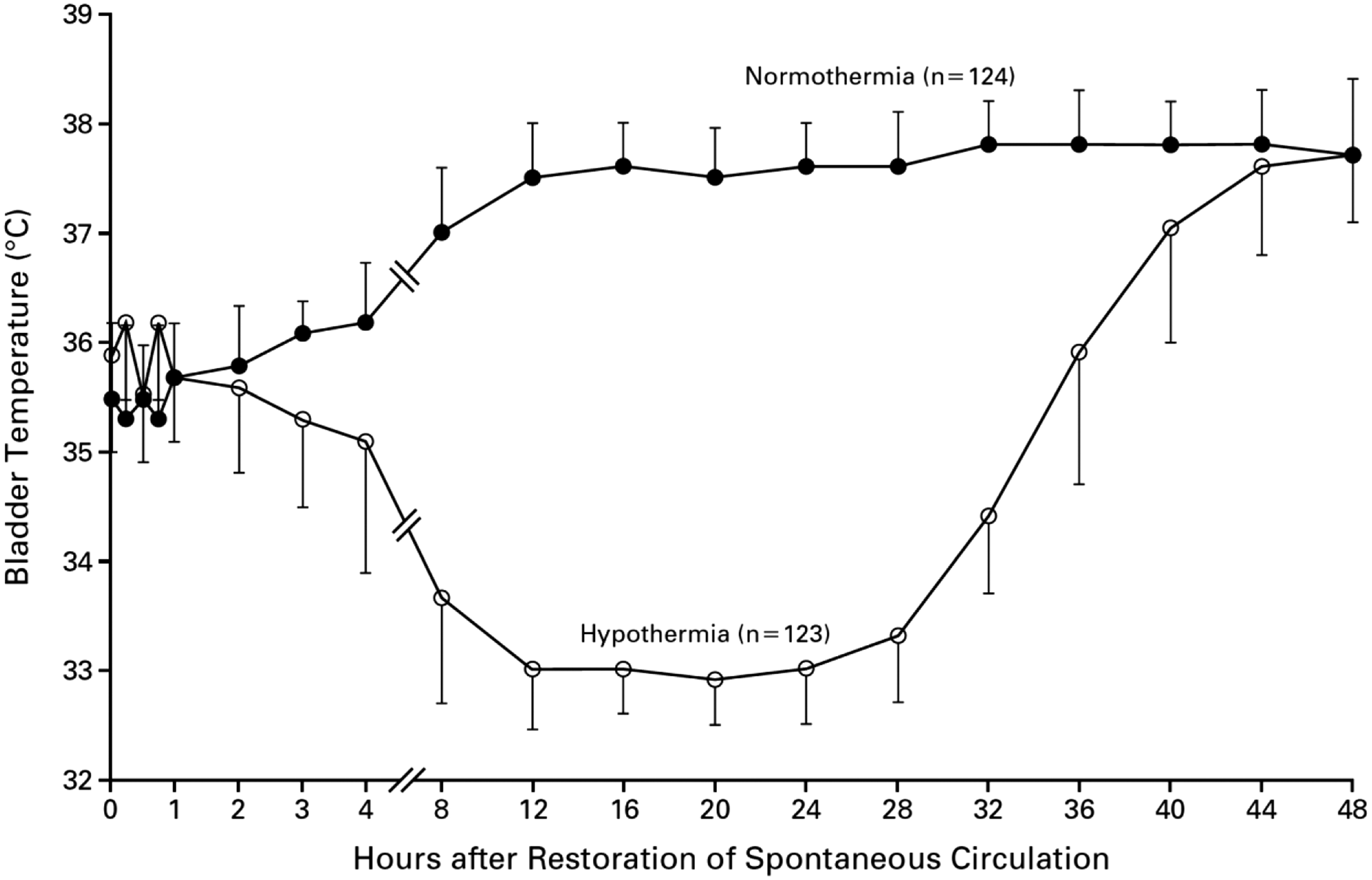
Temperature versus Time from Restoration of Spontaneous Circulation in HACA Trial (Hypothermia after Cardiac Arrest Study Group, 2002).
Characteristics of Randomized Trials of Hypothermia Versus Normothermia in Patients Resuscitated from Cardiac Arrest
Primary outcome was favorable neurologic outcome within 6 months, defined as a Pittsburgh cerebral-performance category of 1 (good recovery) or 2 (moderate disability) on a five-category scale.
Primary outcome was good neurologic outcome, defined as discharge home or to a rehabilitation facility.
Primary outcome was mortality at end of study follow-up. Patients followed for mean 256 days.
Primary outcome was survival with a favorable neurologic outcome 90 days after randomization.
Primary outcome was death at 6 months.
n/a, not applicable.
Excluded from the TTM2 trial were patients with greater than 180 minutes from ROSC to eligibility screening. In their primary report of the results, (Dankiewicz et al, 2021) the TTM2 investigators emphasized the time from randomization to target temperature, rather than from ROSC. Despite their stated goal of applying rapid cooling, they reported a similar time to their intended target temperature in TTM2 as they achieved in the original TTM trial (Nielsen et al, 2013).
A lead investigator of the TTM2 trial stated that patients enrolled in the trial were cooled as fast as is feasible using contemporary medical devices (https://web.archive.org/web/*/https://twitter.com/DogICUma/status/1405348094594621444). However, the recent TTM24vs48 trial (Kirkegaard et al, 2017) achieved a faster time to target temperature than that in TTM2: (281 [IQR, 217–360] minutes in the 48 hours group versus 320 [IQR 241–410] minutes in the 24 hours group [p = 0.01]). Importantly, the mean core temperature did not achieve the intended target in the intervention group in either TTM or TTM2 (i.e., mean temperature did not cross 33°C). Collectively, these data suggest that the relative benefit of IH was attenuated versus the control group in the TTM and TTM2 trials because the intervention was neither delivered as intended nor as quickly as feasible.
The planned primary outcome of TTM2 was all-cause mortality at 6 months (Dankiewicz et al, 2021). Other outcomes were assessed at 30 days, 6 months, and 24 months after randomization. Although there was no significant difference in mortality between the intervention and control group at 6 months, it appears that the intervention was associated with increased early mortality as the survival curves have wider separation around 30 days but come together later (Fig. 2). A plausible interpretation of this is that hypothermia in the TTM2 trial was associated with increased early mortality.
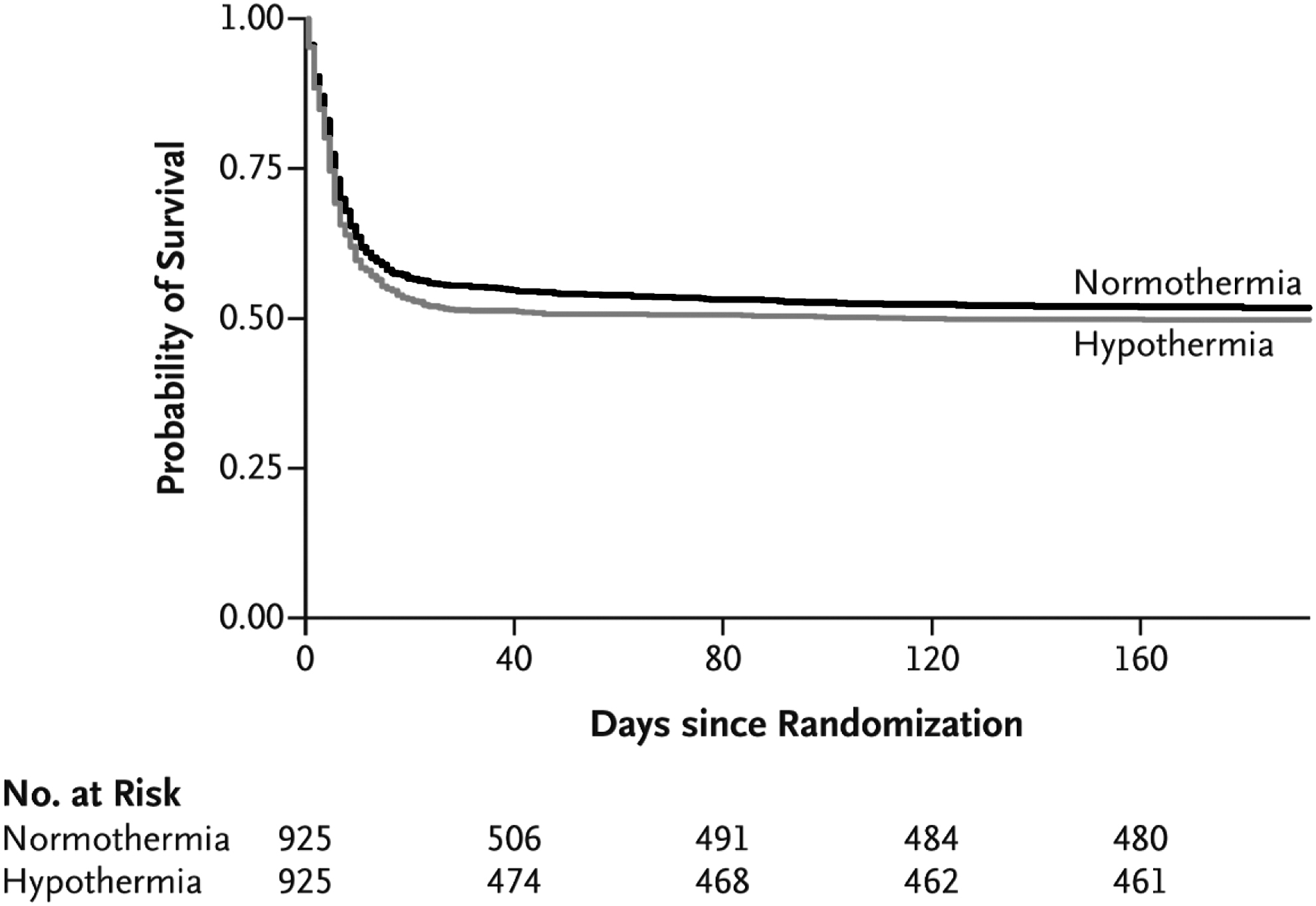
Survival with Hypothermia versus Normothermia Over Time in TTM2 Trial (Dankiewicz et al, 2021).
In the TTM2 trial, hypothermia was initiated with chilled intravenous (IV) saline (Dankiewicz et al, 2019; Jakobsen et al, 2020). In humans resuscitated from CA, chilled IV saline to initiate hypothermia was associated with no survival benefit and possibly increased adverse events (Bernard et al, 2012; Kim et al, 2014). Collectively, these data suggest that the use of chilled IV saline to initiate TTM could have contributed to the apparent increased early mortality in the intervention group versus the control group in the TTM2 trial.
Was The Treatment Regimen Appropriate?
Limited information is available about the quality of postresuscitation care that patients enrolled in the TTM2 trial received. A prior retrospective analysis of observational data demonstrated that the quality of postresuscitation care, including how TTM is initiated and maintained, is associated with outcome after resuscitation from CA (Stub et al, 2015). Note that the TTM2 investigators stated in their methods article that “General intensive care management [was] according to standard practice at participating hospitals (Dankiewicz et al, 2019).” But limited information is available about the quality of postresuscitation care that patients enrolled in the TTM2 trial received. Below, we describe why the quality of concurrent care is relevant to interpretation of the TTM2 trial.
Cooling method
The majority of patients enrolled in the TTM2 trial had hypothermia induced and maintained with surface cooling methods (SCM) as opposed to intravascular temperature management (IVTM). But SCM cools at slower rates than IVTM (Sonder et al, 2018). Multiple systematic reviews show that use of SCM is associated with worse outcomes than IVTM (Bartlett et al, 2020; Calabro et al, 2019). Collectively, these data suggest that it is plausible that preferential use of SCM rather than IVTM attenuated the benefit of moderate cooling in the TTM2 trial.
Propofol
The intervention group received significantly more propofol than the control group in the TTM2 trial: median (interquartile range) 8,768 (3,683, 13,365) mg versus 7,744 (3,183, 12,595) mg (p value not stated). (Dankiewicz et al, 2021) Similarly, a substudy from a hospital that enrolled a large number of patients in the TTM trial reported that the moderate hypothermia group received significantly more propofol than the mild hypothermia group (Bro-Jeppesen et al, 2014). Propofol was not available for clinical use in early trials of IH in patients with OHCA (Bernard et al, 2002; Hypothermia after Cardiac Arrest Study Group, 2002). Note that propofol has dose-dependent effects on mitochondria. At low doses, it reduces ROS (Branca et al, 1995). At higher doses, it reduces adenosine triphosphate synthesis (Branca et al, 1995; Branca et al, 1991a; Branca et al, 1991b; Rigoulet et al, 1996; Sztark et al, 1995).
Small observational and randomized studies of the use of propofol for sedation in patients with CA have not demonstrated consistent effect (Bjelland et al, 2012; Paul et al, 2018; Staudacher et al, 2018). But in a systematic review of volatile anesthetics versus propofol in patients undergoing cardiac surgery with cardiopulmonary bypass (N = 42 trials, n = 8,197 patients), (Bonanni et al, 2020) volatile anesthetics had lower 1-year mortality (5.5% vs. 6.8%; odds ratio, 0.76 [95% confidence interval [CI]: 0.60–0.96]; p = 0.023) and less myocardial infarction (odds ratio, 0.60 [95% CI: 0.39–0.92]; p = 0.023).
Propofol has also been compared to other methods of sedation in patients requiring intensive care. In a systematic review of use of volatile agents versus IV sedation, including propofol in patients receiving critical care (N = 13 trials, n = 1,027 patients), (Kim et al, 2017) volatile agents had less myocardial injury as measured by serum troponin levels 6 hours after ICU admission than patients who received IV sedation (p < 0.05). Collectively, these clinical data suggest that it is plausible that the frequent use and higher dose of propofol in the hypothermia group could have attenuated the relative benefit of hypothermia compared to normothermia in the TTM2 trial.
Antiplatelet therapy during revascularization
Information about which TTM2 patients received which of P2Y12 inhibitor or experienced stent thrombosis or reinfarction is not available. Overall, about 40% of patients had ST-segment myocardial infarction (STEMI); 38% of patients underwent percutaneous coronary intervention (PCI) (Dankiewicz et al, 2021). Evidence-based practice guidelines strongly recommend administration of P2Y12 inhibitors as early as possible to reduce the risk of stent thrombosis (O'Gara et al, 2013). Currently available oral (clopidogrel, prasugrel, ticagrelor) or parenteral (cangrelor) P2Y12 inhibitors are acceptable in normothermic patients.
But in a trial enrolling patients with STEMI undergoing PCI (Nichol et al, 2015), clopidogrel significantly increased acute stent thrombosis in the setting of intraperitoneal hypothermia. The ability of oral P2Y12 inhibitors to achieve timely and adequate platelet inhibition in hypothermic patients is limited (Bednar et al, 2016; Bjelland et al, 2010; Flierl et al, 2016; Steblovnik et al, 2016). Patients resuscitated from CA who received IH and oral P2Y12 inhibitors did not achieve satisfactory platelet inhibition (Bjelland et al, 2010; Buchtele et al, 2020; Ibrahim et al, 2014). In contrast, cangrelor inhibit platelets when given concurrent with hypothermia (Pruller et al, 2018).
It seems plausible that most patients who underwent PCI in the TTM2 trial did not receive cangrelor, as 99% of patients were enrolled outside the United States, where health care costs are more constrained. If a significant proportion of hypothermic patients received oral P2Y12 inhibitors, as seems likely, they would be at risk of stent thrombosis and worse outcomes. This could have contributed to the apparent short-term increase in mortality observed in the moderate hypothermia group in the TTM2 trial.
Implantable defibrillator
Overall, 16% of patients enrolled in the TTM2 trial received an implantable cardioverter defibrillator (ICD) during follow-up. Evidence-based practice guidelines strongly recommend implantation of ICDs in survivors of ventricular fibrillation without a completely reversible cause, as it is associated with a significant and important mortality benefit (Al-Khatib et al, 2018). In contrast to the low rate of ICD use in the TTM2 trial, 42% of a national US sample of patients admitted to hospital after resuscitation from CA in 2002/2003 underwent ICD insertion (Birnie et al, 2007). The large divergence in ICD implantation rates between the TTM2 trial and usual practice could have been associated with reduced survival, attenuating differences in outcome between the control and intervention group.
Neuroprognostication
Modern neuroprognostication guidelines such as those used in the TTM2 trial attempt to predict poor functional outcomes. But these neuroprognostication guidelines lack high diagnostic accuracy (Pouplet et al, 2022). Despite efforts to standardize neuroprognostication in the TTM2 trial (Dankiewicz et al, 2021), a high proportion of patients had withdrawal of life-sustaining therapies (WLST) at 96 hours. Moreover, a high proportion of patients had WLST for reasons other than poor neurologic prognosis (Supplementary Fig. S3 in in Dankiewicz NEJM 2021 Supplement).
Possible accumulation of sedative drugs in hypothermic patients (Bjelland et al, 2013) may have contributed to premature decisions to withdraw therapy in patients with ongoing sedation as opposed to severe brain injury. In a prospective cohort of patients who did not have early WLST, 49% of those who survived to sedation withdrawal after 72 hours were still unconscious (Nakstad et al, 2020). In this study, the time frame arrest to awakening was mean (SD) 6.1 (4.0) days among those discharged with favourable neurologic outcome. Of these, 32% eventually obtained good neurologic outcome. It seems plausible that the high early rate of WLST could have attenuated the effect of IH/TTM.
Do Secondary Outcomes Elicit Reveal Positive Findings?
The TTM2 trial reported a significant increase in the rate of bradycardia requiring pacing in the intervention group compared to the control group (Dankiewicz et al, 2021). It is unclear whether the site investigators were given specific guidance on when pacing was required in the TTM2 trial protocol (Dankiewicz et al, 2019). Bradycardia is commonly observed during application of hypothermia. But such bradycardia is associated with increased cardiac output due to increased stroke volume (Forkmann et al, 2015).
The TTM investigators and others previously reported that early bradycardia is associated with improved survival and neurologic outcome after CA (Staer-Jensen et al, 2014; Thomsen et al, 2016). The TTM2 trial reported that although total arrhythmias did not differ between the two randomized groups, arrhythmias with hemodynamic compromise were more common in the hypothermia group (HR, 1.45 [95% CI: 1.21–1.75] p < 0.00). Possible reasons posited for an apparent higher arrhythmia risk in the hypothermia group are electrolyte disturbances (e.g., hypokalemia) or a direct effect of hypothermia.
In the TTM2 trial, the authors reported that hypokalemia was more frequent in the 33°C compared to the 36°C group (19% vs. 13%). The incidence of VT/VF was similar between randomized groups.
In contrast to the observations of TTM2, significant differences in rates of arrhythmia were not reported in other recent trials of IH in patients with CA (Lascarrou et al, 2019; Le May et al, 2021). In a prospective observational study (Adler et al, 2020), hypokalemia and malignant arrhythmias (VT/VF) were associated with a more rapid time to target temperature. VT/VF occurred in 20% of patients. Additional predictors of VT/VF were a higher number of shocks during resuscitation and higher intensive care use of epinephrine.
Collectively, these data suggest that the clinical significance of the arrhythmia reported in the TTM2 is incompletely defined.
Can Alternative Analyses Help?
The systematic review of the effectiveness of IH or TTM in patients resuscitated from CA reports significant or near significant statistical heterogeneity among the study results. Statistical heterogeneity in a systematic review implies that the observed intervention effects are more different from each other than one would expect due to random error (i.e., chance) alone. The Cochrane Collaboration Handbook on Systematic Reviews states (Granfeldt et al, 2021) as follows:
“Meta-analysis should only be considered when a group of studies is sufficiently homogeneous in terms of participants, interventions, and outcomes to provide a meaningful summary.”
Following from this, (Salcido et al, 2021) clinicians should be cautious about concluding whether TTM does or does not improve outcomes in patients resuscitated from CA based upon this meta-analysis.
Post hoc analyses of the TTM2 trial data could provide further insights. Such analyses might include examining the interaction of mode of cooling, time to cooling from ROSC, enrollment site, and concurrent care (e.g., type of P2Y12 inhibitor; sedation without propofol; insertion of an ICD) (Dankiewicz et al, 2019; Jakobsen et al, 2020). These analyses would generate hypotheses about how to optimize postresuscitation care and inform the design of further trials.
Does More Positive External Evidence Exist?
Evidence external to that of the TTM2 trial suggests that hypothermia improves outcomes compared to normothermia. The HYPERION trial demonstrated that in patients with a first-recorded rhythm that is nonshockable, 10.2% of patients in the hypothermia group were alive with a CPC score of 1 or 2 at 90 days, compared to 5.7% in the normothermia group (difference, 4.5 percentage points; 95% CI: 0.1–8.9; p = 0.04) (Lascarrou et al, 2019). Also, there was no significant difference in adverse events between the hypothermia and normothermia group.
One of the main mechanisms of benefit of IH/TTM is posited to be attenuation of hypoxic brain injuries (HIBI) (Sun et al, 2019). Such HIBI can lead to brain death or permanent alteration of brain function. To be effective, IH needs to be applied to those at risk of moderate to high level of HIBI. A high level of HIBI would contribute to a high level of dependency, that is, higher proportion of patient with poor functional outcome (Taccone et al, 2021). Regarding recent trials, HYPERION is the only one with a proportion of poor functional outcome higher than 10% in the control group (Lascarrou et al, 2019).
When the original TTM trial was published, postresuscitation practices changed at many hospitals to favor use of a target temperature of 36°C as opposed to 33°C. Several large multicenter before and after studies conducted outside the United States have demonstrated that this change in practice was associated with increased mortality (Nolan et al, 2021; Salter et al, 2018).
Multiple retrospective analyses of data from the United States demonstrate that there is a significant relationship between the duration of ischemia and the effect of IH in patients with CA (Reynolds et al, 2016; Sawyer et al, 2020). It seems unlikely that if there is truly no benefit to IH, that such a dose-response relationship would have been observed.
Collectively, these data suggest that it is plausible that, notwithstanding the results of the ILCOR systematic review and TTM2 trial, hypothermia may improve outcomes compared to normothermia in patients resuscitated from CA.
Conclusion
It is reasonable to still use or evaluate IH treatment in patients who are comatose after CA. There are multiple plausible reasons why IH compared to normothermia did not significantly improve neurologic outcome in the TTM trials.
Footnotes
Author Disclosure Statement
Graham Nichol is a consultant to ZOLL Circulation (San Jose, CA), which manufactures and markets devices for IVTM. He is also a consultant to Heartbeam, Inc. (Santa Clara, CA), Invero Health LLC. (Montvale, NJ), and Orixha, Inc. (Saint Cyr Au Mont d'Or, France). He has research funding from ZOLL Medical (Chelmsford, MA), Vapotherm, Inc. (Exeter, NH), and Abiomed, Inc. (Danvers, MA) and is a member of the steering committee of the PRINCESS 2 Trial of Ultrafast Hypothermia after cardiac arrest. Michael Holzer received honoraria for lectures and consulting from C.R. Bard, Inc. (Murray Hill, NJ), which manufactures and markets devices for surface temperature management, and Zoll Medical (Chelmsford, MA) and is a member of the steering committee of the PRINCESS 2 Trial of Ultrafast Hypothermia after cardiac arrest.
Jeanne E. Poole and Ken Fujise have no relevant conflicts related to this article. Jean-Baptiste Lascarrou received lecture fees from C.R. Bard, Inc. (Murray Hill, NJ), and Zoll Medical (Chelmsford, MA). None of these companies or their representatives subsidized preparation of this work, or reviewed it before publication.
Funding Information
No funding was received in support of this article.