
Abstract
The present study aimed to evaluate the structure of the rabbit retina after vitreoretinal surgery using prolonged irrigation with solutions of different temperatures. Thirty-six rabbits (72 eyes) were included in this study and randomly divided into 3 equal groups according to the temperature of the intraocular irrigating fluid they received during vitrectomy. Vitreoretinal surgery was performed with a 5°C irrigation solution in group 1 (12 rabbits, 24 eyes), a 22°C irrigation solution in group 2 (12 rabbits, 24 eyes), and a 36°C irrigation solution in group 3 (12 rabbits, 24 eyes). In each group of animals, the mean irrigation/aspiration time was 30 minutes for left eyes and 60 minutes for right eyes. Histological examination of the retina was performed 1, 7, and 30 days after surgery. During surgery, the temperature in the vitreous cavity of the eyes of rabbits of groups 1, 2, and 3 dropped by 26.0°C, 11.2°C (deep hypothermia), and 1.0°C (mild hypothermia), respectively. The highest rewarming rate was detected in group 1 (0.9°C/min) compared with group 2 (0.7°C/min) and group 3 (0.2°C/min). After 60 minutes of irrigation, retinal structural changes were detected in the animals of groups 1 and 2 (in contrast to the animals of group 3). After surgery with irrigation lasting 30 minutes, no retinal structural changes were observed. This study showed that temperature management, avoidance of intraoperative deep hypothermia, and prevention of rapid uncontrolled rewarming may protect the retinal morphology and increase the safety of prolonged vitreoretinal surgery.
Introduction
Thermoregulation is one of the most important aspects of maintaining homeostasis in mammals (Markota et al, 2022). Body temperature is carefully regulated and fluctuates in very narrow ranges (Tan and Knight, 2018). The constancy of the internal temperature is necessary for the normal course of metabolic reactions in humans and animals (Refinetti, 2020).
Changes in the optimal internal temperature can lead to disruption of the normal cellular function in the organs and tissues of the body (Cheshire, 2016). The damaging effect of deep hypothermia as well as severe hyperthermia on the structure of the nervous tissue (including the nervous tissue of the retina) of experimental animals has been proven in several studies (Daló et al, 2007; Watanabe et al, 1982; White et al, 2007; Zilis et al, 1990). At the same time, mild hypothermia has a beneficial effect on brain neurons during ischemia modeling, whereas mild hyperthermia potentiates brain damage, producing effects similar to those observed with an increase in the duration of ischemia (Busto et al, 1987; Minamisawa et al, 1990; White et al, 2007).
Controlled changes in body temperature can lead to a therapeutic effect due to neuroprotection (Jackson and Kochanek, 2019). In the practice of intensive care for emergency conditions, mild therapeutic hypothermia is considered to be an effective method of neuroprotection, affecting the level of survival and the quality of patients' neurological recovery (The Hypothermia After Cardiac Arrest Group, 2002), in contrast to mild hyperthermia (Lundbye, 2012). Mild therapeutic hypothermia is successfully used in some emergencies (stroke, traumatic brain injury, intracranial pressure elevation, subarachnoid hemorrhage, spinal cord injury, hepatic encephalopathy, and neonatal encephalopathy) to reduce neurological damage (Andrews et al, 2018; Sun et al, 2019).
Interestingly, an ultra-mild shift in temperature of only 1–2°C can also cause beneficial or harmful reactions in neurons in vitro (Jackson et al, 2015) and in patients. Specifically, in unconscious adult survivors of out-of-hospital cardiac arrest, small 1–2°C temperature reductions were shown to be equally effective in terms of neurological outcomes and mortality compared with traditional mild hypothermia (Nielsen et al, 2013). On the contrary, increases in 1°C body temperature in the posthypoxic ischemic period is associated with an increase in the odds of poor outcome in newborns (Laptook et al, 2008). Previously, it was found that under conditions of ischemia, ultra-mild hyperthermia is dangerous not only for the brain's nerve cells but also for the retina (Tamai et al 1997).
Currently, the concept of targeted temperature management (TTM) is widely used in intensive care medicine (Cariou et al, 2017; The Hypothermia After Cardiac Arrest Group, 2002). TTM is used in critical care units to protect brain cells under unfavorable ischemic conditions (Cariou et al, 2017). This technique actively achieves and maintains the patient's target body temperature at all treatment stages to reduce secondary neurological injury (Jackson and Kochanek, 2019; Nielsen et al, 2013; Saigal et al, 2015). TTM includes medical procedures to cool the human body, safely rewarm after the cooling phase, and maintain normothermia or prevent fever (Nunnally et al, 2011; Polderman and Herold, 2009).
There are also emergency conditions in ophthalmic practice, such as penetrating injuries of the eyeball, and retinal detachment, which require immediate treatment (Feltgen and Walter, 2014; Pokhrel and Loftus, 2007). Vitreoretinal surgery is considered the gold standard for the management of such patients (Aylward, 2014; Rani et al, 2020). Despite the successful long-term history of vitreoretinal surgery in ophthalmic practice, several unresolved issues in this field remain that reduce the effectiveness of treatment. For example, ischemic damage to the retina during vitreoretinal surgery is known, which is due to an intraoperative drop in ocular perfusion pressure (Rossi et al, 2014). In addition, intraoperative phototoxic damage to the retina, retinal toxicity of dyes used to gently remove intraocular membranes, and mechanical damage to the inner layers of the retina during vitrectomy by air infusion are dangerous in vitreoretinal surgery (Farah et al, 2009; Hasumura et al, 2000; Postel et al, 1998). There is a risk of various complications after surgery (inflammation, edema of the macula) (Romano et al, 2013).
Currently, undeservedly little attention is paid to temperature control during vitreoretinal surgery. Only a few studies are devoted to the assessment of various temperature conditions for safe vitreoretinal surgery (Tamai et al, 1997; Zilis et al, 1990). For vitreoretinal surgery, irrigation solutions are used, the temperature of which is much lower than the temperature of intraocular media (Anatychuk et al, 2021). The intraocular temperature or the temperature of irrigation solutions, as a rule, is not monitored. Typically, the irrigation fluid temperature corresponds to the operating room temperature. Therefore, vitreoretinal surgery is performed under conditions of artificial, uncontrolled local ocular hypothermia. Often, the surgery lasts long (120 minutes or more) (Cheng et al, 2001). The issue of how long and at what temperature it is advisable to use irrigation solutions during vitreoretinal surgery remains insufficiently investigated.
Previously, it was found that vitreoretinal surgery with room temperature irrigation fluid is accompanied by uncontrolled deep hypothermia followed by rapid rewarming, which can be dangerous for the nervous tissue of the retina. (Anatychuk et al, 2021). Based on the experience of using therapeutic hypothermia in various fields of medicine, we hypothesized that mild or ultra-mild hypothermia would avoid possible cold damage to the neural retinal tissue and preserve the benefits of cooling in vitreoretinal surgery. Thus, the present study aimed to investigate the structure of the rabbit retina after vitreoretinal surgery using prolonged irrigation with solutions of different temperatures.
Methods
Animals
Thirty-six adult male rabbits (72 eyes; 6 months old) weighing 2.5–3.5 kg were included in this study and randomly divided into three equal experimental groups according to the temperature of the intraocular irrigating fluid they received during vitrectomy. Vitreoretinal surgery was performed with a 5°C irrigation solution in group 1 (12 rabbits, 24 eyes), a 22°C irrigation solution in group 2 (12 rabbits, 24 eyes), and a 36°C irrigation solution in group 3 (12 rabbits, 24 eyes). Experimental animals were housed and bred conventionally. Rabbits with any ocular pathology at the baseline examination were excluded. Each animal underwent biomicroscopy and ophthalmoscopy at baseline, immediately after surgery, and then daily until euthanasia.
The study was approved by the local Bioethics Committee of the State Institution “The Filatov Institute of Eye Diseases and Tissue Therapy of the National Academy of Medical Sciences of Ukraine” (approval No. 6). All experiments were conducted in accordance with the NIH Guide for the Care and Use of Laboratory Animals.
Surgery and temperature measurements
Before surgery, anesthesia was used in the form of intramuscular injections of 10% thiopental sodium at a dose of 1.0 mL/kg of animal weight. The pupils were dilated with atropine sulfate 1% solution.
The Accurus 400VS surgical system (Alcon Laboratories, Fort Worth, TX) was used for vitreoretinal surgery. The surgical area was prepared with an antiseptic solution, and an epibulbar anesthetic (ophthalmic 0.5% proxymetacaine hydrochloride) was administered. With a 23 G instrument and standard three-port access, vitrectomy of the central and peripheral parts of the vitreous body was performed through a flat part of the ciliary body (cut frequency: 1500–1800/min, aspiration: 150 mm Hg, infusion pressure: 20 mm Hg). The vitrectomy time averaged 4 minutes. At the second stage, prolonged continuous irrigation of the vitreous cavity was carried out. Irrigation of the vitreous cavity was accompanied by continuous aspiration of the fluid. In each group of animals, the mean irrigation/aspiration time was 30 minutes for left eyes and 60 minutes for right eyes.
For irrigation, a balanced Ringer's lactate solution was used. Gel heat accumulators were used to cool or heat the irrigation fluid to the required temperature. The solution's cooling or heating took place in an irrigation tube in close proximity to the surgical site. The temperature of the irrigation solution (22°C) was created by placing the bottle with the solution in the operating room several hours before surgery.
A multichannel thermoelectric device was used to measure the temperature in the vitreous cavity and the temperature of the irrigation solution (Anatychuk et al, 2021). Following the installation of a lid speculum and epibulbar anesthesia, and after the establishment of surgical access, a measurement probe was introduced into the vitreous through a standard port in the projection of the flat part of the ciliary body. Before surgery and at different surgery time points, the temperature in the vitreous cavity was measured. The intraocular temperature was measured after cessation of irrigation until its initial level was restored to assess the duration of rewarming. The temperature of the irrigation fluid entering the eye was constantly monitored during surgery. In all cases, the rectal temperature of the rabbit and the indoor temperature were also registered. The ambient operating room temperature ranged between 22°C and 24°C.
After surgery, rabbits were instilled with sulfacyl sodium 20% and ofloxacin 0.3% four times a day during the observation period of 1–10 days to prevent postoperative infection.
Histology
For histological examination of the retina, animals from each group were euthanized 1, 7, and 30 days after surgery (n = 4 animals per group for each time point). Enucleated eyes were fixed in 10% formaldehyde for 24 hours before being embedded in paraffin and sectioned. Hematoxylin–Eosin (H&E)-stained sections were examined by light microscopy. We studied samples in the same place of the eyeballs (about 3 mm inferior to the optic nerve head) in different groups. Six different sections from each eye were randomly selected and each section was examined at three different points. The specimens were evaluated by two experienced histopathologists using the same criteria. They determined the final consensus decision for each case.
Our microscopic analysis revealed the following changes: vacuolization, edema, subretinal serous fluid accumulation, loss of photoreceptors, disorganization of photoreceptors, loss of ganglion cells, disorganization of inner retinal layers, macrophage infiltration, retinal pigment epithelium proliferation, hemorrhage, necrosis, neuron degeneration, and thinning of the retina.
Areas with normal histology did not contain the above changes or had sporadic areas of vacuolization in the retina. Edema, subretinal serous fluid accumulation, loss of photoreceptors, disorganization of photoreceptors, loss of ganglion cells, disorganization of inner retinal layers, macrophage infiltration, retinal pigment epithelium proliferation, hemorrhage, necrosis, neuron degeneration, or thinning of the retina were always considered pathological.
Statistical analysis
The experimental temperature data were expressed as mean ± standard deviations. The paired Student's t-test was used to compare the temperature in the vitreous cavity before and after surgery. Categorical data (number of the examined areas displaying normal and pathological histology) were shown as percentages and frequencies, % (n). Categorical data were analyzed using a chi-square test. Statistical significance was set at p < 0.05. Statistical analysis was performed using Statistica 10.0 (StatSoft, Tulsa, OK) software.
Results
The body temperature of experimental animals was recorded to be an average of 38.2°C ± 0.7°C in group 1, 38.0°C ± 0.7°C in group 2, and 38.3°C ± 0.3°C in group 3 and did not significantly differ between the studied groups (p < 0.05). The body temperature of animals corresponded to normothermic values for rabbits in all groups. The temperature dynamics in the vitreous cavity, recorded in the experiment, are presented in Table 1.
Temperature Dynamics of the Vitreous Cavity After Vitrectomy
The table shows average values and their SDs (mean ± SD).
Significant difference (p < 0.05) in temperature compared with group 1.
Significant difference (p < 0.05) in temperature compared with group 2.
SD, standard deviation.
The duration of recovery of intraocular temperature to the initial level after cessation of irrigation averaged 30.5 ± 4.9 minutes in group 1, 15.3 ± 3.3 minutes in group 2, and 4.7 ± 1.5 minutes in group 3.
During the surgery, no changes in the cornea were observed, and the lens clarity was maintained. In two cases, in animals of the first and second groups, hemorrhage into the vitreous cavity occurred intraoperatively but was eliminated during surgery.
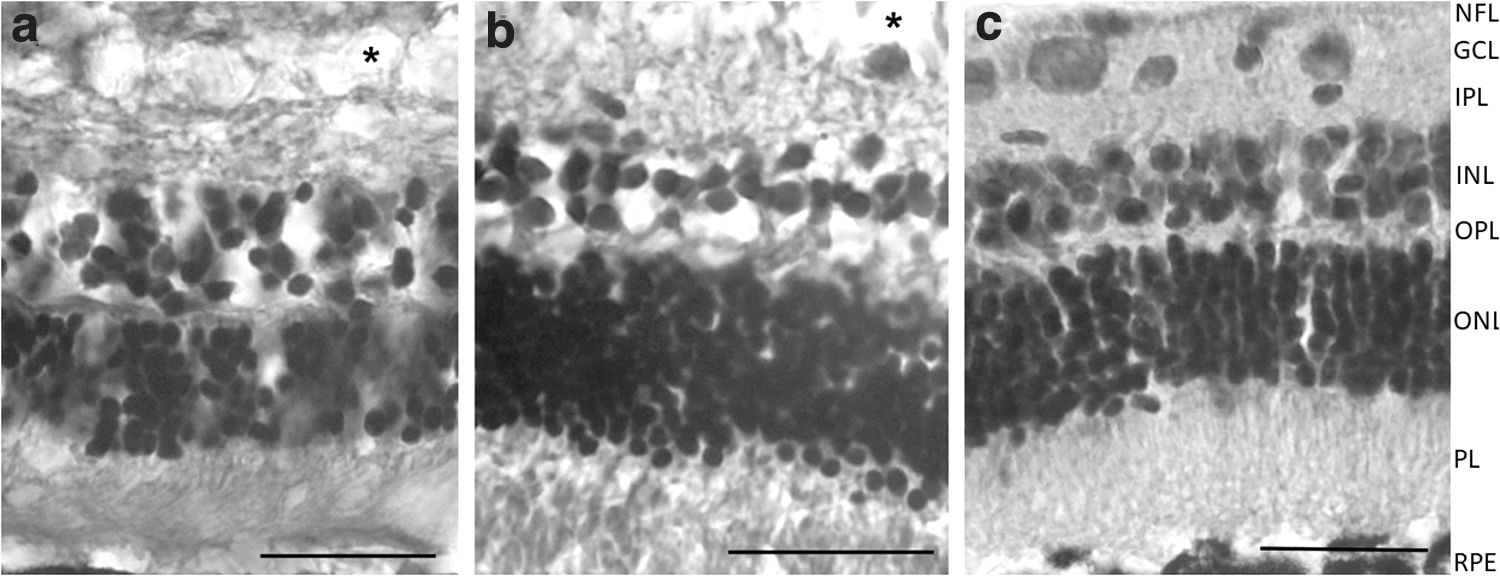
Histological examination revealed that 1 day after 30-minute irrigation of the vitreous cavity with a solution cooled to 5°C, all retinal layers retained a normal structure. In a small number of examined areas (n = 7, 10%) of the histological sections, vacuolization foci were found mainly in the ganglion cell layer. No other pathological changes were observed. Seven days (Fig. 1a) and 30 days after surgery, it was observed that retinal ganglion cells were sparsely located in some samples. After 30 minutes of cooling, the vitreous cavity with a 22°C and 36°C fluid, the retina retained its normal layered structure (Fig. 1b, c). Histological changes of the retina after 30-minute irrigation of the vitreous cavity, recorded in the experiment, are presented in Table 2.

Histological Changes of the Retina After 30-Minute Irrigation of the Vitreous Cavity
Significant difference (p < 0.05) in histological changes compared with histology 1 day after surgery.
On day 1 after surgery with a 5°C fluid and a cooling time of 60 minutes, pronounced edema was observed in the inner layers of the retina (from the ganglion cell layer to the inner nuclear layer). Vacuolization of the retina was found in 61% (n = 44) of the examined areas. The structure of the retina located under the medullary ray was normal. After 7 days, the retina retained signs of pronounced edema in its inner layers (Fig. 2a). In some portions of the retina, signs of edema could also be observed in the layer of photoreceptors. Retinal ganglion cells were absent or sparsely located in some of the points. Thirty days after surgery, in some retinal sections, limited areas of vacuolization, as well as other changes in the usual structure of the retina, were observed (i.e., thinning of the retina with a decrease in the number of rows of neurons in the nuclear layers, loss of ganglion cells, scattering of cells in the inner nuclear layer) (Fig. 3a).
Histological sections of rabbit retina after vitrectomy with 60-minute irrigation.

Histological sections of rabbit retina after vitrectomy with 60-minute irrigation.
One day after 60 minutes of irrigation of the vitreous cavity with a 22°C fluid, the tissues of the posterior part of the eyeball looked slightly changed. No pronounced edema was observed in the layers of the retina, including its peripheral area. Nonetheless, in 44% (n = 32) of the examined areas, fluid accumulation was found in the inner layers of the retina and, in particular, in the layer of ganglion cells. After 7 days, signs of edema were observed in the inner layers of the retina, including in the inner nuclear layer and the layer of ganglion cells. Retinal ganglion cells were sparsely located in some portions of the retina. Although in the histological sections, the arrangement of neurons of the inner nuclear layer usually corresponded to the normal retina, there were also developments such as disarrangement and loss of the cells of this retinal layer (Fig. 2b). Along with the afore-described phenomena, there were sections of the retina that retained a normal structure. Thirty days after surgery, it was noted that the retina had a normal layered structure. No retinal vacuolization was observed (Fig. 3b).
On day 1 after surgery using 60-minute irrigation with a 36°C solution under light microscopy in some retinal sections, single swollen cavities were observed (22% [n = 16] of the examined areas), particularly in the layer of ganglion cells. On the 7th day, it was noted that the retinal structures corresponded to similar structures of intact animals (Fig. 2c). Thirty days after surgery, the histology of the retina was normal (Fig. 3c).
Histological changes in the retina after 60-minute irrigation of the vitreous cavity are presented in Table 3.
Histological Changes of the Retina After 60-Minute Irrigation of the Vitreous Cavity
Significant difference (p < 0.05) in histology compared with group 1.
Significant difference (p < 0.05) in histology compared with group 2.
Significant difference (p < 0.05) in histological changes compared with histology 1 day after surgery.
Discussion
In this study, three levels of irrigation fluid cooling were used for surgery. Irrigation fluid temperature corresponding to room temperature (group 2) was chosen to simulate the conditions of standard vitreoretinal surgery. The extremely low temperature of the irrigation fluid (group 1) was chosen to increase the likelihood of detecting pathological changes in the retina due to deep hypothermia. Against this background, one could detect the less obvious consequences of cooling the retina with irrigation fluid at room temperature. Finally, we used the third level of cooling of the irrigation fluid in our study (group 3), taking into account the previously discovered and successfully used in medicine beneficial effects of mild and ultra-mild hypothermia.
During vitreoretinal surgery using irrigation fluid at room or lower temperatures, a significant decrease in the intraocular temperature of the rabbit occurs. In our work, after the vitrectomy, the temperature in the vitreous cavity of the eyes of rabbits in groups 1 and 2, compared with the initial temperatures, decreased by 26.0°C and 11.2°C, respectively. Such fluctuations in temperature likely lead to disruption of the normal cellular function of the retina. In group 3, the intraocular temperature decreased by only 1.0°C, which, in our opinion, is less dangerous for retinal cells and may provide a neuroprotective effect. According to the available classifications of hypothermia levels, vitreoretinal surgery was performed in groups 1 and 2 under conditions of deep hypothermia and in group 3 under conditions of ultra-mild hypothermia (Jackson et al, 2015; Silverstein and Hopper, 2009).
In the present study, after 60 minutes of irrigation, microscopic changes in the retina of group 3 animals were notable for the absence of edema and ganglion cell loss compared with that in the eyes of group 1 and 2 animals. Based on this finding, we hypothesized that the observed changes in the retina and the temperature of irrigation fluid are related. In all cases, the irrigation fluids used had the same composition and differed only in temperature.
Relevant reports of other authors about damage to the nervous tissue of experimental animals against the background of deep hypothermia confirm the correlation of the microscopic changes in the retina that we found with the level of intraoperative cooling (Daló et al, 2007; Molina et al, 1984; Watanabe et al, 1982). Evaluation of neuronal death in organotypic cultures of the rat hippocampus after cerebral ischemia showed that deep hypothermia increased cell death even when after only hypoxia (Gregersen et al, 2013). Daló et al (2007) observed severe neuronal cell damage characterized by swelling, and vacuolated cytoplasm with distended neuronal bodies in amphibians in the presence of deep hypothermia. Studies of brain changes during induced deep hypothermia in dogs have revealed microscopic cellular damage in the form of vacuolization, edema, hemorrhage, microinfarctions, necrosis, neuron degeneration, and other changes (Molina et al, 1984). In addition, deep hypothermia is known to be associated with neurological damage in patients (Khaladj et al, 2008; Levin et al, 2005).
On the other hand, there are reports of the beneficial effect of mild hypothermia on the state of brain neurons in modeling ischemia (Minamisawa et al, 1990). Mild hypothermia can reduce the degree of damage to the blood–brain barrier, thereby decreasing the risk of developing cerebral edema under ischemic conditions (Yenari and Han, 2012). Furthermore, mild hypothermia reduces the inflammatory response of brain tissues (Deng et al, 2003), and leads to the inhibition of the apoptosis process (Saito et al, 2010). Taking into account the results obtained and the numerous literature data, our preclinical findings suggest that irrigation solutions that produce deep hypothermia in vitreoretinal surgery may not be optimal. We believe that avoiding deep hypothermia and aiming for mild or ultra-mild intraoperative hypothermia may be beneficial to retinal neural tissue.
At the same time, changes in the retina found after vitrectomy may be due to the rapid rewarming of the retina after the cooling phase. Previous laboratory and clinical data demonstrate that slow rewarming optimizes the protective effects of hypothermia, while rapid posthypothermic rewarming in both damaged and healthy brains can lead to adverse effects, even exacerbating brain pathology and dysfunction (Povlishock and Wei, 2009).
The recovery of intraocular temperature after cooling in all three groups was much faster than the recommendations used in the practice of emergency care (Nunnally et al, 2011; Polderman and Herold, 2009; Saigal et al, 2015). The longest duration of the intraocular temperature recovery phase was in animals of group 1, compared with groups 2 and 3. At the same time, the highest rewarming rate was detected in group 1 (0.9°C/min) compared with group 2 (0.7°C/min) and group 3 (0.2°C/min). This may also explain the more pronounced changes found in the retina of the animals of group 1. Thus, the effect of different duration and rates of rewarming on the morphology and function of the retina will require additional studies.
The detected retinal changes were likely to be partially reversible in animals of the second group since in animals euthanized 30 days after 60-minute surgery, structural changes in the retina were weak or not detected. According to our observations, the restoration of the layered structure of the retina occurred mainly due to the regression of edema in the layers of the retina. However, some changes persisted by day 30 in group 2, such as the loss of ganglion cells. In animals in group 1, despite the regression of edema, degenerative changes in the retina (thinning of the retina, disorganization and thinning of retinal layers, loss of ganglion cells, disarrangement of cells in the inner nuclear layer) persisted at long-term follow-up.
In our study, 30-minute irrigation of the vitreous cavity did not lead to similar changes in the structure of the retina in any of the studied groups. It can be assumed that damage to the normal cellular function of the retina and the appearance of a large number of vacuoles in the layers of the retina after surgery is an obvious consequence of prolonged low-temperature exposure.
This preliminary study has a number of limitations though. First, quantitative analysis of ganglion cells could improve the evaluation of the effect of the level of hypothermia on the retina. Second, the study of morphological changes in retinal vessels and the functioning of the blood–ophthalmic barrier will improve the assessment of the effect of hypothermia on retinal vessels and possible fluid leakage. Finally, the evaluation of the effects of hypothermia is very limited to light microscopy of the samples. Apoptotic degeneration of retinal ganglion cells can be confirmed by methods such as the TUNEL (Terminal deoxynucleotidyl transferase dUTP Nick-End Labeling) assay (Mirzayans and Murray, 2020).
In subsequent studies, it is advisable to study not only the effect of ultra-mild hypothermia but also mild hypothermia of various levels on the structure of the retina to select the optimal conditions for vitreoretinal surgery.
In addition, it is not clear whether there are advantages to ultra-mild hypothermia over normothermia in vitreoretinal surgery. For example, early studies in adults showed that therapeutic hypothermia improved neurologic outcomes in comatose survivors after out-of-hospital cardiac arrest (Bernard et al, 2002; The Hypothermia After Cardiac Arrest Group, 2002). Subsequently, another study in such adult patients showed that therapeutic hypothermia, as compared with actively maintained therapeutic normothermia, did not improve outcomes (Nielsen et al, 2013).
It was previously noted that standard vitreoretinal surgery with room temperature irrigation fluid is performed under conditions of uncontrolled ocular hypothermia with rapid uncontrolled rewarming of the vitreous cavity after cooling, and ocular hyperthermia in the postoperative period (Anatychuk et al, 2021). We believe that to improve the safety of vitreoretinal surgery, it is necessary to introduce TTM technology, which involves not only intraoperative management of the temperature of the irrigation fluid but also the management of the rewarming of the vitreous cavity and control of the ocular temperature in the postoperative period. Thus, confirmation of the benefits of TTM in vitreoretinal surgery and the introduction of this technique into surgical practice requires further targeted research.
Conclusions
Our findings suggest that temperature management of irrigation fluid, avoidance of intraoperative deep hypothermia, and prevention of rapid uncontrolled rewarming may protect the retinal morphology and increase the safety of prolonged vitreoretinal surgery. These findings should be more fully explored in additional preclinical studies in our experimental model.
Footnotes
Acknowledgment
The authors thank professor Valeriy V. Vit for his assistance in evaluating the results of the study.
Authors' Contributions
The authors confirm contribution to the article as follows: conception and design of the study: L.A. and N.P.; data collection: O.Z. and R.N.; analysis and interpretation of results: O.Z., R.K., V.N., and E.M.; drafting the article: O.Z. O.Z., E.M., R.N., M.U., T.K., I.N., and A.K. contributed to the experimental studies. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.