
Abstract
This study compared the pregnancy and neonatal outcomes between fresh embryo transfer and frozen-thawed embryo transfer (FET). These patients were split into two groups: the fresh embryo transfer group and the FET group. The general conditions, pregnancy outcomes, and neonatal outcomes between these groups were compared. The influencing factors of fetal macrosomia occurrence were explored as well. Compared with the fresh embryo transfer group, the FET group had a significantly higher mean age (32.59 ± 4.77 vs. 31.90 ± 4.71, p < 0.05) and lower multiple pregnancy rate (21.2% vs. 26.9%, p < 0.05). There was no significant difference in the incidence of congenital anomalies of neonates between the two groups (1.32% vs. 0.37%, p > 0.05). In the FET group, compared with the fresh embryo transfer group, the mean birth weight of singleton live births, the cesarean section rate, and the incidence of fetal macrosomia were significantly increased, while the incidence of low birth weight was significantly decreased. The logistic analysis showed that the occurrence of fetal macrosomia was primarily associated with the embryo transfer protocol (odds ratio [OR] = 2.769, 95% confidence interval [CI]: 1.246–6.154, p < 0.05), endometrial thickness (OR = 1.144, 95% CI: 1.043–1.256, p < 0.05), and gestational age (OR = 1.710, 95% CI: 1.338–2.184, p < 0.05). Macrosomia (OR = 2.938, 95% CI: 1.436–6.010, p = 0.003) and multiple pregnancy (OR = 3.574, 95% CI: 2.616–4.882, p < 0.001) significantly increased the cesarean section rate. The risk of fetal macrosomia and congenital anomalies in the offspring of the fresh embryo transfer group was lower than that in the offspring of the FET group, we preferred to fresh embryo transfer for patients with assisted reproductive technologies. FET should be used as supplementary therapeutic strategy with strengthened pregnancy management and screening to reduce the occurrence of birth defects in newborns.
Background
Since the birth of the world's first test-tube baby in 1978, over eight million newborns have been born via in vitro fertilization (IVF) embryo transfer or other assisted reproductive technologies (ARTs) worldwide (Crawford and Ledger, 2019; Zegers-Hochschild et al., 2017). In the process of ART treatment, the remaining available embryos after fresh embryo transfer are usually frozen for later thawing transfer, which can effectively avoid repeating the expensive IVF process. In addition, when severe Ovarian Hyperstimulation Syndrome (OHSS) may occur and Preimplantation Genetic Testing (PGT) is required, when fresh embryo transfer is not suitable for special conditions, or in special circumstances such as intimal-embryo dyssynchrony that are not suitable for fresh embryo transfer, “freeze-all protocol” is an optimal alternative (Blockeel et al., 2016).
In recent years, with the popularization of the application of frozen-thawed embryo transfer (FET), FET has become more and more popular and even a trend due to its higher pregnancy rate, live birth rate, and pregnancy safety compared with fresh-embryo transfer. At present, the number of newborns born with FET treatment is increasing, and the effect of embryo freezing technology on pregnancy outcomes and newborns has been paid more and more attention. In this study, the pregnancy and neonatal outcomes between fresh embryo transfer and FET are compared and analyzed to evaluate the impact of these transfer protocols on the outcomes to provide a basis for clinical transfer protocol selection.
Materials and Methods
Subjects
A retrospective analysis was conducted on the data of patients who received treatment with IVF embryo transfer and its expanded technologies (with a total of 4771 cycles) in the Department of Reproductive Medicine of the First Affiliated Hospital of Shantou University Medical College from January 2016 to December 2020. Based on the embryo transfer protocol, these patients were divided into two groups: the fresh embryo transfer group (n = 1163) and FET group (n = 3608). The inclusion criteria were as follows: patients who had male infertility factors or the factors of fallopian tube in the female pelvis, ovulatory dysfunction, or endometriosis and received treatment via IVF/intracytoplasmic single-sperm injection (ICSI) after ovarian hyperstimulation.
Methods
Assisted reproductive treatment process
For the patients with IVF/ICSI indications, the examination before the commencement of the assisted reproduction procedure was performed after contraindications were excluded. Different ovarian hyperstimulation protocols were selected according to the patients' conditions. When two to three leading ovarian follicles reached 18 mm in diameter and the average estradiol (E2) level per mature follicle varied between 200 and 300 pg/mL, transvaginal oocyte retrieval was scheduled 34–38 hours after the injection of recombinant human chorionic gonadotropin (rhCG) 250 μg ± hCG (human chorionic gonadotropin) 1000–2000 IU. For the patients at risk of OHSS, the hCG dosage was decreased (4000 IU).
For patients using an antagonist who were at high risk for OHSS, GnRH-a (0.1–0.2 mg) trigger was used. Conventional IVF or ICSI was performed according to the semen conditions on the day of oocyte retrieval. The formation of pronucleus was observed on day 1 after fertilization, and the development of embryos was observed on days 3 and 5. Priority was given to one to two high-quality embryos for fresh embryo transfer.
Vitrification was performed with the patients' informed consent for the remaining usable embryos or the embryos that could not be subject to fresh embryo transfer in the cycle due to high OHSS risk, a progesterone level >1.5 ng/mL on the trigger day, hydrosalpinx or endometrial factors, ovarian hyperstimulation during the luteal phase, or use of microstimulation as the ovarian hyperstimulation protocol. An appropriate endometrial preparation protocol was selected according to each patient's infertility factors and ovulation at the second menstruation cycle after oocyte retrieval. The frozen embryo was thawed the morning of the transfer, and B-ultrasound–guided FET was performed.
On day 14 after embryo transfer (i.e., day 12 after blastocyst transfer), a β-hCG blood test was performed to judge whether the patient was pregnant, and B-mode ultrasonography was conducted around 4–5 weeks after embryo transfer. If the gestational sac was detected, clinical pregnancy was confirmed.
Outcome measures
The case data of all patients were collected. The follow-up was conducted until delivery, and the mean age, mean number of embryos transferred, clinical pregnancy rate, first-trimester abortion rate, ectopic pregnancy rate, live birth rate, preterm birth rate, sex ratio at birth, and incidence of congenital anomalies between fresh embryo transfer group and FET group were compared. All pregnant patients were divided into the singleton pregnancy group and multiple pregnancy group. The mean neonate birth weight, cesarean section rate, percentage of very low birth weight (VLBW) infants, percentage of low birth weight (LBW) infants, percentage of normal birth weight infants, and percentage of fetal macrosomia between the fresh embryo transfer and FET protocols were compared between the groups.
Judgment criteria of neonatal outcomes
The judgment criteria were as follows: premature infant: an infant born before 37 completed weeks of gestation; VLBW infant: an infant born weighing <1500 g; LBW infant: an infant born weighing <2500 g but ≥1500 g; normal weight infant: an infant born weighing <4000 g but ≥2500 g; and fetal macrosomia: an infant born weighing 4000 g or more.
Ethics
This study was approved by the Reproductive Ethics Committee of the hospital, while the Informed consent was obtained from the patients via the relevant informed consent form.
Statistical analysis
The software SPSS 22.0 was used for the statistical analysis. The measurement data conforming to the normal distribution were statistically described as the mean ± standard deviation, and the enumeration data were statistically described as percentages (%). A t-test was used for intergroup comparisons of measurement data; a chi-square test was adopted for intergroup comparisons of enumeration data. Logistic regression analysis was used to explore the factors influencing the occurrence of fetal macrosomia. A p-value <0.05 indicated that there was a statistically significant difference.
Results
It can be seen from Table 1 that there were statistically significant differences (p < 0.05) in the mean age and multiple pregnancy rate between the fresh embryo transfer group and the FET group but no statistically significant differences in the mean number of embryos transferred, clinical pregnancy rate, first-trimester abortion rate, or ectopic pregnancy rate (p > 0.05). Moreover, there were no statistically significant differences in the live birth rate, preterm birth rate, or sex ratio at birth (p > 0.05). The incidence of congenital anomalies of neonates in the FET group was also higher than that in the fresh embryo transfer group but with no statistically significant difference (p > 0.05).
Comparison of General Clinical Parameters, Pregnancy, and Neonatal Outcomes Between the Fresh Embryo Transfer Group and Frozen-Thawed Embryo Transfer
p < 0.05.
FET, frozen-thawed embryo transfer.
As shown in Table 2, in the singleton pregnancy group, the mean birth weight, cesarean section rate, and incidence of fetal macrosomia of newborns conceived by FET were significantly increased (all p < 0.05), while the incidence of LBW was significantly decreased (p < 0.05). In the multiple pregnancy group, there was no statistically significant difference in the mean birth weight, cesarean section rate, incidence of VLBW infants, LBW infants, or normal birth weight infants, or incidence of fetal macrosomia between the fresh embryo transfer group and FET group (p > 0.05).
Comparison of Neonatal Parameters of Single and Multiple Pregnancy Between the Fresh Embryo Transfer Group and Frozen-Thawed Embryo Transfer
p < 0.05.
LBW, low birth weight; VLBW, very low birth weight.
Binary logistic regression was used to further analyze the influencing factors of the occurrence of fetal macrosomia, and the results are shown in Figure 1. The embryo transfer protocol, endometrial thickness, and gestational age were associated with fetal macrosomia. Moreover, the occurrence of fetal macrosomia (odds ratio [OR] = 2.938, 95% confidence interval [CI]: 1.436–6.010, p = 0.003) and multiple birth (OR = 3.574, 95% CI: 2.616–4.882, p = 0.000) significantly increased the cesarean section rate.
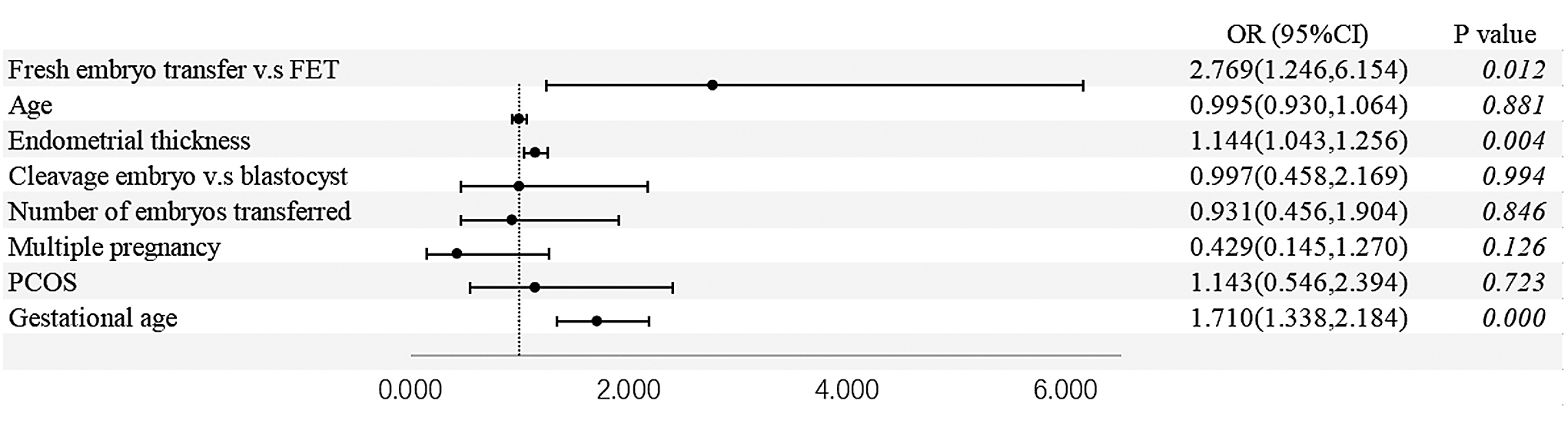
Logistic regression analysis of the influence factors of macrosomia.
The results of this study showed that the congenital anomalies caused by the assisted reproductive technology included cleft lip/cleft palate, ear anomalies, chromosomal abnormalities, central nervous system abnormalities, circulatory system abnormalities, digestive system abnormalities, urinary system abnormalities, and musculoskeletal system abnormalities. Of these, cleft lip/cleft palate accounted for the highest proportion at 23.08% of all congenital anomalies (Fig. 2).
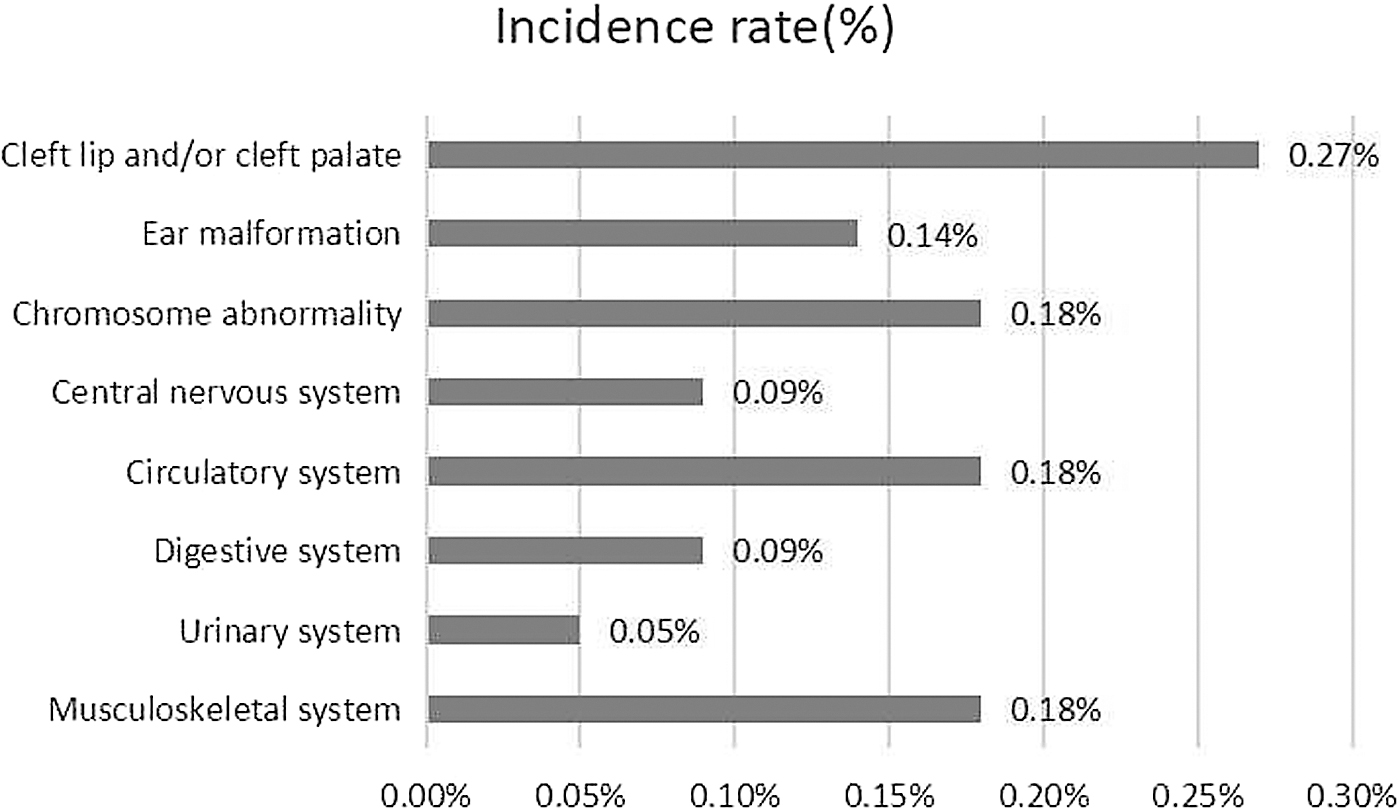
The incidence rates of congenial abnormality from 2016 to 2020.
Discussion
As IVF technology improves, attention should be focused on both IVF pregnancy outcomes and the safety of offspring. The advantage of fresh embryo transfer is that it shortens the treatment time of IVF, but it also increases the risk of OHSS because of Gn use and high estrogen level. As an important ART, FET has the advantages of a reduced incidence of OHSS and an increased cumulative pregnancy rate due to estrogen status and endometrial receptivity improvements. With the combination of PGT and FET, the occurrence of FET in ART treatment is also gradually increasing.
However, FET greatly prolongs the treatment time, and then prolongs the time to live birth. It may increase the cost and workload of treatment and requires additional embryo manipulation. Although frozen-thawed preservation technology has been effectively improved, it is still inevitable to cause embryo freezing damage. In addition, the potential impact of cryopreservation on offspring has always been controversial. Due to the advantages and disadvantages of FET and fresh embryo transfer, further research is still needed. This study analyzed the impact of FET on neonatal outcomes through comparing the pregnancy and neonatal outcomes between fresh embryo transfer and FET.
Relationship between fresh embryo transfer versus FET and the birth weight of newborns
The results of this study showed that the incidence of LBW in singleton pregnancy was significantly lower in the FET group than in the fresh embryo transfer group. Several studies (Sullivan-Pyke et al., 2017) have suggested that IVF embryo transfer technology has led to an increase in the risk of LBW in newborns. In Pelinck et al.'s study (2010), the mean birth weight of IVF newborns in the ovarian hyperstimulation group was decreased by 134 g compared with that in the natural cycle group. Sunkara et al.'s study (2016) indicated that the risk of LBW in newborns in the ovarian stimulation cycle was increased by 58% (95% CI: 0.96–2.58) compared with that in the nonstimulation cycle. These results suggest that ovarian hyperstimulation treatment might be associated with a reduction in neonate birth weight.
Furthermore, there is clinical evidence (Cai et al., 2019; Liu et al., 2017) that the mechanism of LBW in offspring is positively associated with maternal high-estrogen exposure during early pregnancy. A study by Zhang et al. (2019) suggested that there is a threshold effect of the E2 peak on LBW on the day of hCG treatment. If the E2 level is lower than the threshold level (2185 pg/mL), the incidence of LBW increases with the E2 on the day of hCG treatment, and if the level continues to rise to 6136 pg/mL or above, the incidence of LBW decreases by 10% with each 100 pg/mL increase. Animal experiment results have suggested that abnormal glucose metabolism of mice placental tissue induced by ovarian hyperstimulation, and maternal imprinted gene expression disorders play important roles in the molecular mechanism causing LBW.
To sum up, maternal hypoestrogenism exposure is one of the main causes of LBW in offspring. Controlled ovarian hyperstimulation is not required in FET, and the estrogen level in FET is significantly lower than that in fresh embryo transfer on the day of transfer. Thus, maternal hypoestrogenism can be corrected so that the incidence of LBW is significantly decreased.
In addition, this study found that the incidence of fetal macrosomia in the FET group was significantly higher than that in the fresh embryo transfer group in the case of singleton pregnancy and that the occurrence of fetal macrosomia further contributed to an increase in the cesarean section rate. Zhou et al. (2017) compared the conditions of newborns in singleton live births between fresh embryo transfer and FET, discovering that the incidence of fetal macrosomia in the latter was significantly higher than that in the former. Litzky et al. (2018) included 180,184 full-term single-birth infants in their study to compare the impact of FET and fresh embryo transfer on the neonates' birth weight; the results indicated that the mean birth weight of the newborns conceived by FET was 142 g higher than that of the newborns conceived by fresh embryo transfer.
Moreover, the risk of occurrence of fetal macrosomia via FET was 1.7 times as high as that of fetal macrosomia via fresh embryo transfer (95% CI: 1.64–1.76), further supporting the results of the current study. However, there is no consistent explanation for this phenomenon. Several scholars believe that compared with fresh embryo transfer, FET shows better synchronization of endometrium and embryo development, simulates a maternal environment closer to that of reality, and is more conducive to embryo implantation and development. However, Somigliana et al. (2018) believed that epigenetic changes in the process of early embryo development caused by embryo freezing and thawing may affect the late stages of growth and development.
Conventional clinical embryo freezing at the cleavage and blastula stages is an important period of embryonic genome activation and the “erase-and-rebuild” stage of epigenetics, so genetic and epigenetic changes may occur if embryos are thawed at this time. Jahangiri et al. (2018) thawed frozen two-cell mouse embryos and continued to culture them until blastocysts were formed; they found that the expression level of Igf2 was significantly increased, the expression level of Oct4 was significantly decreased, and changes in the level of histone H3K9 methylation and acetylation in the corresponding gene regulation region occurred simultaneously. Through analysis of a DNA methylation group of umbilical cord blood and parental peripheral blood samples, Chen et al. (2020) found that H3K4me3 was the histone modification most seriously affected by freezing and thawing, offering an epigenetic basis for the potential long-term health risks of ART offspring.
Overall, these research works suggest that the impact of FET on neonate weight may be associated with cryogenic freezing and the epigenetic changes of embryos by refrigerants. However, the specific mechanism must be further studied and verified. In the case of multiple pregnancy, there is no significant difference in the weight of newborns between fresh embryo transfer and FET, possibly indicating that pregnancy outcomes are greatly affected by the occurrence of multiple pregnancy. However, this might be associated with the data bias caused by a small number of multiple pregnancy cases.
Relationship between fresh embryo transfer versus FET and congenital anomalies
Based on the current study's results, the congenital anomalies caused by assisted reproductive technology include cleft lip/cleft palate, ear anomalies, and chromosomal, CNS, circulatory system, digestive system, urinary system, and musculoskeletal system abnormalities, consistent with the literature.
The results of a meta-analysis (Liang et al., 2017) indicated that the incidence of cleft palate in offspring in the IVF/ICSI group increased by 34% (95% CI: 1.07–1.69), that of other head and neck abnormalities increased by 20% (95% CI: 1.04–1.39), that of chromosomal abnormalities increased by 23% (95% CI: 1.07–1.40), that of respiratory system abnormalities increased by 28% (95% CI: 1.01–1.64), that of digestive system abnormalities increased by 46% (95% CI: 1.29–1.65), that of musculoskeletal system abnormalities increased by 47% (95% CI: 1.25–1.72), that of urinary system abnormalities increased by 43% (95% CI: 1.18–1.72), and that of circulatory system abnormalities increased by 39% (95% CI: 1.23–1.58). Luke et al. (2021) found that compared with natural conception, ART primarily enhances the risk of single-pregnancy nonchromosomal birth defects, cardiovascular defects, and other birth defects in addition to twin-pregnancy chromosomal defects.
At present, whether FET increases the risk of congenital anomalies in offspring remains unclear. The majority of scholars currently believe that FET does not enhance the risk of birth defects in newborns compared with fresh embryo transfer. For instance, Kato et al. (2012) included 6623 single-birth ART offspring in their study and found that the incidence of birth defects of those conceived by fresh embryo transfer and FET was 1.9% and 2.4%, respectively, with no statistically significant difference. In the current study, the incidence of congenital anomalies in the fresh embryo transfer and FET groups was 0.37% and 1.32%, respectively (p = 0.08), with no statistically significant difference.
However, many clinically related influencing factors were observed. If the significance level had been relaxed to 0.1, there would have been a statistically significant difference in the incidence of congenital anomalies between the groups. Bai et al.'s (2016) study showed that the risk of the occurrence of birth defects in newborns in the frozen embryo group was increased. Thus, whether FET enhances the birth defects of offspring and relevant mechanisms is worthy of research. Further analysis finds that the incidence of cleft lip/cleft palate is the highest of the congenital anomalies caused by assisted reproductive technology, possibly due to the impacts of the embryo freezing and thawing process and cryoprotectants on the epigenetics of the embryos. However, as this was a single-center retrospective cohort study, data bias might exist to some extent. A multicenter, large-sample randomized controlled trial study is required for further validation.
Conclusion
Although studies have suggested the effect of embryo cryopreservation on embryo epigenetic inheritance, the short-term and long-term impacts of embryo cryopreservation technology on fetal genes and phenotypes remain unclear. Our study revealed the incidence of fetal macrosomia and congenital anomalies in the offspring conceived via FET was higher than that via fresh-embryo transfer. In addition, embryo cryopreservation increases patients' treatment expenses, time cost, and economic and psychological pressure, consequently, we preferred to fresh embryo transfer for patients with ARTs. FET should be used as supplementary therapeutic strategy with strengthened pregnancy management and screening to reduce the occurrence of birth defects in newborns.
Footnotes
Authors' Contributions
Conception and design of the research: M.C. and Y.W.; acquisition of data: Y.W. and R.X.; analysis and interpretation of the data: M.C. and H.L.; statistical analysis: M.C. and R.X.; writing of the article: M.C. and Y.W.; critical revision of the article for intellectual content: H.L. and Z.L. All authors read and approved the final draft.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.