
Abstract
Cervical spinal cord injury (SCI) usually results in severe, long-term disability. Early therapeutic hypothermia (33–34°C) has been used to improve outcomes in preclinical studies, but previous clinical studies have commenced cooling after arrival at hospital. The objective of the study is to determine the feasibility and safety of early therapeutic hypothermia initiated by paramedics and maintained for up to 24 hours in hospital in patients with SCI. This is a pilot clinical study. The study was undertaken at Ambulance Victoria and The Alfred Hospital, Victoria, Australia. A total of 17 consecutive patients with suspected acute traumatic cervical SCI were enrolled. Patients with suspected cervical SCI were administered a bolus (up to 20 mL/kg) intravenous (IV) cold (4°C) normal saline in the prehospital phase of care. After hospital admission and spinal imaging, further cooling used IV catheter temperature control or surface cooling. Major complications and long-term outcomes were compared with historical controls admitted to the same center before the study. A decrease in core temperature of 1.1°C was achieved during prehospital care and the target temperature was achieved in 6 hours with mechanical temperature management devices in the hospital. There were no major safety concerns. Patients with motor complete SCI who underwent early decompressive surgery had a favorable rate of partial spinal cord recovery compared with historical controls. Therapeutic hypothermia induced using bolus, large-volume, ice-cold saline prehospital and maintained for 24 hours using mechanical devices appears to be feasible and safe in patients with SCI. Larger trials need to be undertaken to determine whether prehospital cooling combined with early decompressive surgery improves outcomes in patients with complete cervical SCI.
Australian and New Zealand Clinical Trials Registry (ACTRN12616001086459).
Introduction
Cervical spinal cord injury (SCI) is an uncommon but devastating injury following trauma. In patients with cervical spinal column fracture with dislocation, pressure on the spinal cord and complete motor loss below the level of injury, decompressive surgery within 24 hours appears to be of benefit (Ter Wengel et al., 2019).
One treatment proposed to improve outcomes is the induction of early therapeutic hypothermia (33–34°C) before early decompressive surgery (Batchelor et al., 2010). Preclinical studies in animals with spinal cord compression demonstrated that early hypothermia followed by early decompression significantly improved outcomes in the hypothermia group (Batchelor et al., 2010; Ransom et al., 2022).
There have been two clinical trials reporting the use of systemic therapeutic hypothermia in patients with cervical SCI (Dididze et al., 2013; Vedantam et al., 2022). The first observational study used an intravenous (IV) catheter temperature control device in a total of 35 patients with SCI with a mean time to initiation of cooling of 7.1 hours (Dididze et al., 2013). In a randomized trial of 27 patients who underwent hypothermia compared with 23 control patients who remained normothermic after SCI, the time to reach target temperature is not reported, although this study also used an IV catheter temperature control device, which was inserted after arrival at hospital (Vedantam et al., 2022).
Given the strongly supportive data in preclinical studies that early induction of hypothermia results in greater protection of the spinal cord, cooling commenced during prehospital care could significantly shorten the time to target temperature. However, there have been no previous studies of therapeutic hypothermia induced during prehospital care in patients with SCI.
One approach to prehospital cooling is the rapid IV infusion of large-volume (20 mL/kg), ice-cold saline. This has been previously used in clinical trials to induce prehospital therapeutic hypothermia following resuscitation from out-of-hospital cardiac arrest (Bernard et al., 2010, 2016) and traumatic brain injury (Cooper et al., 2018).
In this study, we undertook a pilot clinical trial of a rapid IV infusion of large-volume (up to 20/mL/kg), ice-cold saline (4°C) during prehospital care or immediately after arrival at the Emergency Department (ED) to induce early therapeutic hypothermia in patients with SCI. Hypothermia was then maintained using an IV catheter temperature control device or surface cooling for 24 hours. Patients with complete SCI and significant spinal cord compression on computed tomography (CT)/magnetic resonance imaging (MRI) also underwent early (<12 hours) spinal decompression surgery.
Methods
Study design
This prospective study was undertaken in Victoria, Australia over 24 months, ending May 2019. Consecutive patients with suspected traumatic cervical SCI were recruited. The planned enrollment target was 18 patients; 9 patients with motor complete cervical SCI and 9 patients with motor incomplete cervical SCI. Historical controls consisted of patients with cervical SCI in a previous SCI study undertaken in Victoria over the 5 years preceding this trial (Agostinello et al., 2019).
Ethics
The research protocol was approved by The Alfred Hospital Human Research Ethics Committee and the study was registered on the Australian and New Zealand Clinical Trials Registry. Patients or their medical treatment decision maker were contacted within 72 hours following injury and provided with a detailed explanation of the nature of their injury and study procedures. At that stage, consent for ongoing study participation was affirmed. No patients subsequently withdrew from the study.
Recruitment
Patients were screened by the attending paramedics using a brief neurological assessment to estimate the level and severity of spinal injury (The SPEED assessment) (Battistuzzo et al., 2016). Patients were enrolled into the study if 18–65 years of age, they had an isolated motor complete cervical SCI (no lower limb movement together with weak or absent hand grip) or if they had an isolated motor incomplete SCI (altered lower limb movement and sensation together with weak or absent hand grip). Patients were excluded if they had a significant head injury (Glasgow coma score <13), suspected drug intoxication, multitrauma with suspected major internal blood loss, or pre-existing major neurological deficits.
Procedures and interventions
Patients enrolled underwent induction of hypothermia by IV 500 mL bolus of ice-cold (4°C) normal saline administered during patient transport over 10 minutes, with repeated boluses permitted until the patient's core temperature reached 33–34°C or a maximum of 20 mL/kg of body weight had been administered. The temperature was measured using a tympanic temperature thermometer.
Following arrival at hospital, a neurological examination was performed, the American Spinal Injury Association (ASIA) grade of injury established, and CT and MRI cervical spine imaging performed. Patients with C3–T1 vertebral fracture/dislocation injuries and ≥25% canal narrowing evident on imaging were prioritized for emergency decompression. Ongoing therapeutic hypothermia (33–34°C) was achieved using either an IV temperature control catheter (Alsius Icy™ CoolGuard catheter, Zoll Circulation, Inc.) inserted into the patient's inferior vena cava through the femoral vein or through surface cooling blankets (Medi-therm III™, Gaymar Industries, Inc.) set to maintain the target temperature at 33–34°C.
Patients who did not have a C3–T1 vertebral column injury or where a clear diagnosis of SCI could not be determined clinically or radiologically were rewarmed to normal temperature and managed as per standard hospital protocols.
The trial protocol recommended that in addition to cooling, motor-complete patients with spinal cord compression as a result of C3–T1 vertebral fracture/dislocation injuries be taken to theater for decompression and fixation within 8 hours of injury. The trial protocol also recommended that motor-incomplete patients with cord compression as a result of C3–T1 central cord or vertebral fracture/dislocation injuries be taken to theater for open decompression and fixation within 18 hours of injury. The time to decompression was calculated as the time from injury to the midpoint of surgery.
Patients were maintained at 33–34°C until 24 hours postinitiation of cooling and then slowly rewarmed at 0.15°C/hour to 36°C. Patients then underwent controlled temperature management to maintain a core temperature between 36°C and 37°C for a further 72 hours. Mean arterial pressure was maintained at a target of 80 mmHg throughout using noradrenaline as needed.
Following discharge from the Intensive Care Unit (ICU) or at two weeks, patients were transferred to a specialist spinal injury unit for further management. Therefore, the complications developed during this study were limited to those that occurred within the first 14 days after injury.
Feasibility, safety, and clinical outcome measures
Feasibility outcome measures included the time from injury to initiation of prehospital cooling by paramedics, the volume of fluid infused during prehospital cooling, the temperature reduction achieved by paramedics and the time taken for core temperature to reach the target temperature 33–34°C.
The safety of the cooling was evaluated by assessment of the incidence and severity of health complications observed or reported within the first 14 days following injury. The incidence of shivering, the length of intubation, and the ICU length of stay were also evaluated.
Study participants underwent an Abbreviated Injury Scale (AIS) grade assessment six (± one) months following injury to evaluate clinical outcome.
Statistical analyses
Baseline variables and data were summarized using descriptive statistics. The temperatures, timing of decompressive surgery, incidence of health complications, and clinical outcomes measured in the study cohort were compared with historical cervical SCI patients. The incidence of health complications was compared with historical patients with isolated cervical SCI as reported in the study by Agostinello et al. (2019). The timing of decompressive surgery and clinical outcomes in the motor complete study cohort were compared with the group of patients with isolated motor complete injuries included in the study by Battistuzzo et al. (2016). To control for initial injury severity, the historical patients were those who were assessed as SPEED = 0 at the accident scene and AIS grade A on arrival in hospital. Fisher's exact test was used to detect differences in the proportion of patients experiencing respiratory and other complications and for evaluating clinical outcome. Significance for all analyses was set at p < 0.05.
Results
Recruitment
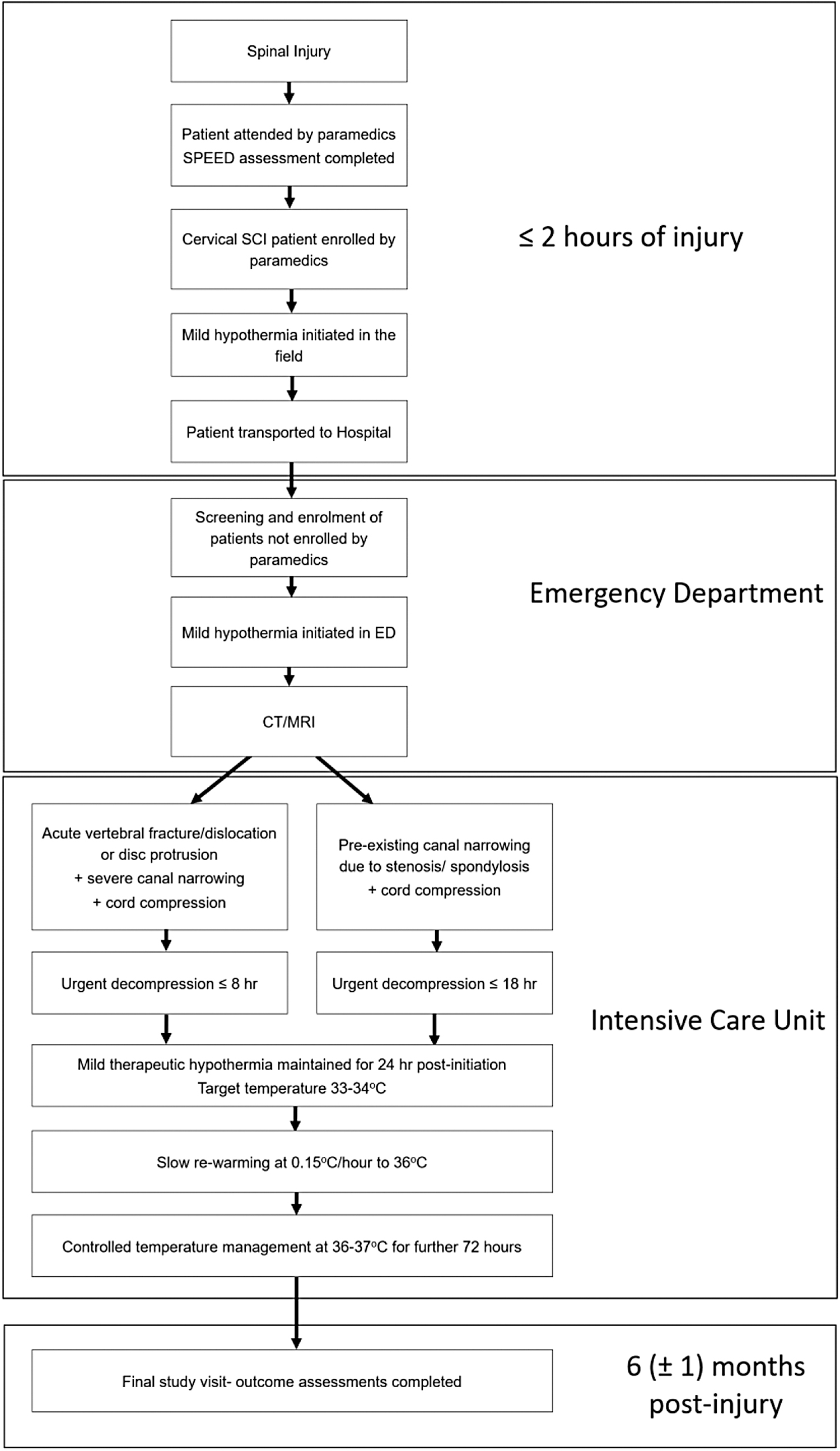
Over the 2-year recruitment period, 17 patients with traumatic cervical SCI were enrolled. Fifteen patients were enrolled by paramedics and two further patients were enrolled immediately on arrival at the ED. Seven patients presented with motor complete cervical SCI (six ASIA grade A, one ASIA grade B) and radiological investigation demonstrated that all these patients had fracture and/or dislocation injuries. Ten patients presented with motor incomplete SCI and radiological investigation demonstrated that 2/10 patients had fracture or dislocation injuries, 3/10 patients had central cord injuries, while the remaining 5/10 had transient neurological deficits with no radiologically identified cord injury. The enrollments are shown in a Consort Diagram (Fig. 1) and the process of care is shown in Figure 2.
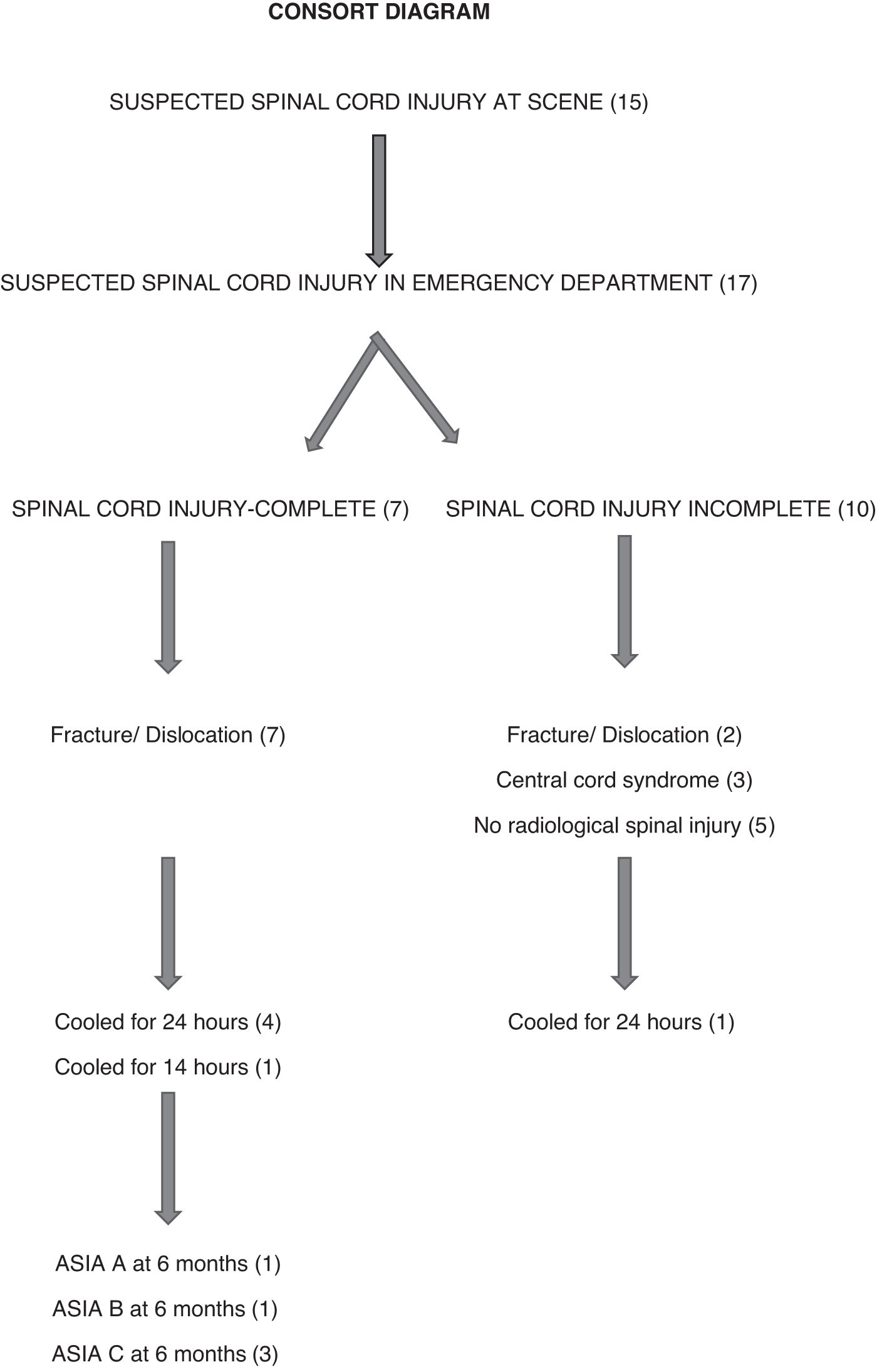
Consort diagram.
Patient Progress over Time.
The average age of enrolled patients was 39 years and 94% were male. The majority of accidents occurred in rural locations. The mechanism of injury was head-strike when diving into water (29%) and motor vehicle accidents and high falls (both 18%) (Table 1).
Patient Demographics: All Enrolled
Early after enrolment, 5 out of 10 patients with motor incomplete injuries had a rapid resolution of deficits without cord compression evident on imaging and did not require surgical intervention. These patients were then rewarmed. To ensure recruitment of patients suitable for treatment as per protocol, prehospital and hospital inclusion criteria were modified mid recruitment so that only patients with complete loss of motor function in the lower limbs, together with weak or no hand function were enrolled.
Feasibility outcomes
Five of the seven patients presenting with motor complete SCI underwent prehospital cooling and early decompression with surgical treatment times close to the target of 8 hours as set in the study protocol. One patient with motor complete SCI received only 10 minutes of cooling before being withdrawn from the study following identification of a splenic bleed on CT scan. A further patient (with an ASIA B injury) was withdrawn after being enrolled by paramedics but inadvertently actively rewarmed after arrival at hospital.
The mean times for key steps in the process of care spanning the period from paramedic assessment to cooling and then decompressive surgery are shown in Figure 1. In the motor complete cohort (five patients) who underwent prolonged cooling, the mean time to paramedic initiation of hypothermia following injury was 1.6 hours and on average 1.4 L of cold saline was infused during transport. Paramedics were able to achieve a mean reduction of 1.1°C in tympanic temperature. Data on the timing of interventions is shown in Table 2. A temperature of ≤35°C was achieved a mean of 2.9 hours postinjury and the mean time taken to reach the target hypothermic temperature (33–34°C) following injury was 6.0 hours. The average temperatures before and after ice-cold saline is shown in Figure 3.
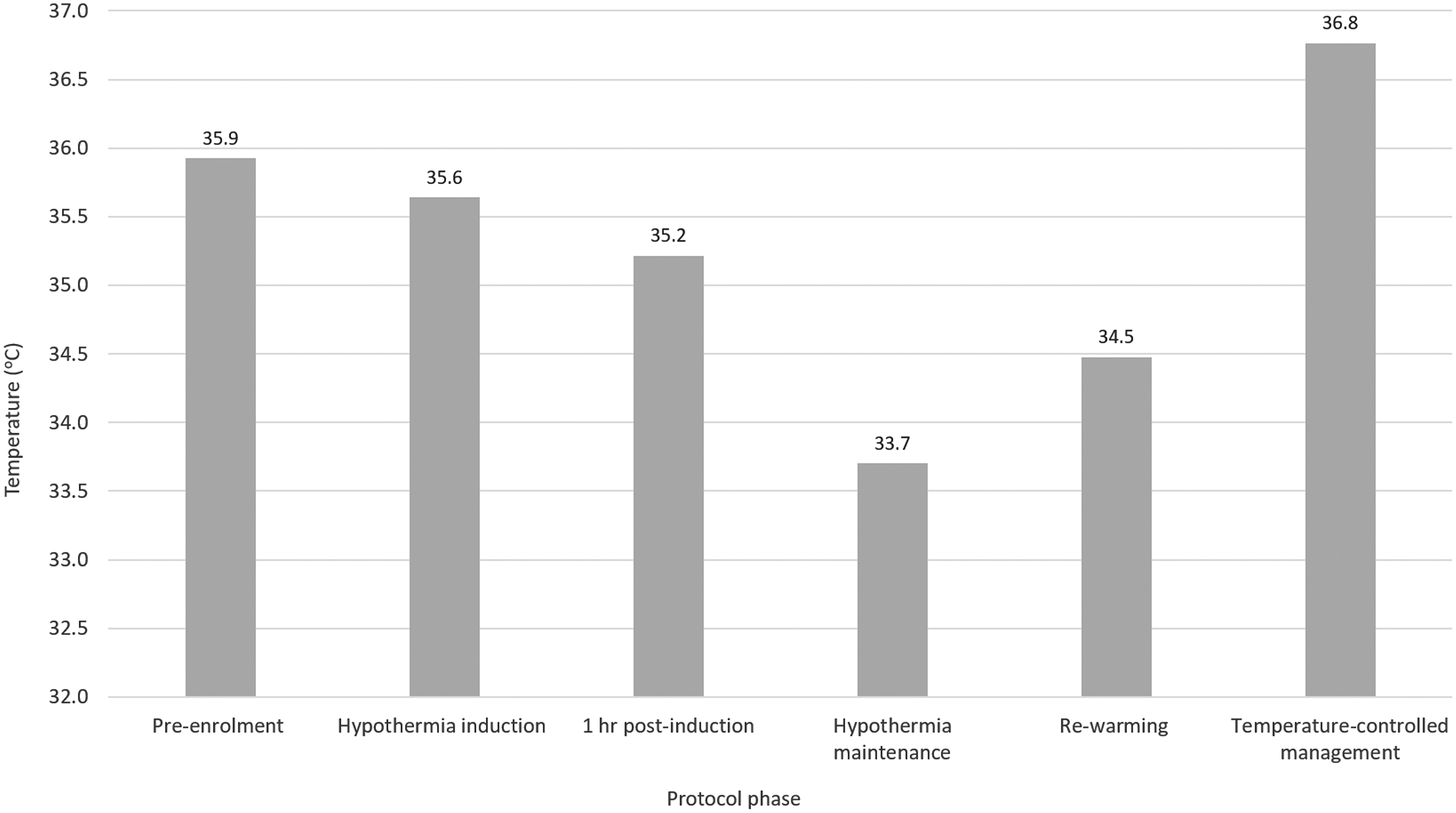
Temperature over time.
Evaluation of Feasibility of Therapeutic Interventions Data
Data presented as group mean ± standard deviation unless otherwise stated.
One motor complete and nine motor incomplete patients.
Data for N = 4 patients because of lack of early temperature data for the remaining patient.
Data for N = 3 patients; remaining patients did not receive cooling of sufficient duration to achieve these temperatures before being withdrawn.
Paramedic cooling data for N = 4 motor complete patients, N = 9 withdrawn patients.
Intra-operative temperature data for N = 2 withdrawn patients, no active cooling at the time of surgery.
Cooling was continued for 24 hours in four of the motor complete patients and the mean time to decompression following injury in this cohort was 8.1 hours. The fifth patient was found to have minimal cord compression on imaging and underwent delayed stabilization surgery; this patient was rewarmed at 14.5 hours of cooling.
In the cohort with motor incomplete SCI (10 patients), paramedics were able to commence cooling in all patients in a mean of 1.4 hours. However, only one patient had cooling continued for 24 hours, the target set in the study protocol, with all other patients being withdrawn. Five patients were withdrawn because of early substantial recovery of motor function, two patients were withdrawn because their injury was minimal, and two patients were withdrawn because they did not meet the revised enrollment criteria mandating only complete injuries. Three of the 10 patients with motor incomplete injuries also underwent surgery, 2 patients with fracture/dislocation injuries and 1 patient with a central cord mechanism of injury. The mean time to decompression in this group was 7.0 hours. One case with a central cord mechanism of injury was surgically decompressed 7.9 hours postinjury.
Safety outcomes
Complications were evaluated over the first 14 days postinjury. One patient with a motor complete injury following near drowning was diagnosed with aspiration pneumonia in the first 24 hours and went on to develop a ventilator-associated pneumonia (VAP) of moderate severity. Another two motor complete SCI patients were also diagnosed with VAP of moderate severity and a fourth patient was diagnosed with severe VAP requiring inotropic support to maintain hemodynamic stability (Table 3). Hemodynamic complications, including hypotension and bradycardia were also observed in the majority of motor complete SCI patients (100% and 80%, respectively).
Complications for Therapeutic Hypothermia and Emergency Decompression
Motor complete patients N = 5. Motor incomplete patients N = 1. Withdrawn patients N = 10 (one motor complete and nine motor incomplete).
Data from one withdrawn patient who only received 10 minutes of cooling has been excluded.
Only one patient had the onset of hypotension postcooling, others had the onset before commencement of cooling.
The incidence of complications in the protocol cohort was compared with an historical control cohort of normothermic patients with cervical SCI (Agostinello et al., 2019). The proportion of motor complete hypothermic patients with pneumonia was similar to that of the historical control cohort (80% and 75%, respectively, p = 0.65). A smaller proportion of patients in the current study developed atelectasis compared with the historical control cohort (40% and 71%, respectively), however, this difference was not statistically significant (p = 0.08). There was also no significant difference in the incidence of the bradycardia or neurogenic shock compared with the historical cohort.
A serious adverse event was observed where a thrombus in the inferior vena cava was identified in a patient who was cooled using an intravascular cooling temperature catheter. Following removal of the catheter, an inferior vena cava (IVC) filter was placed and the patient continued in the study with no further serious adverse events. Due to IVC thrombus developing in other patients in the ICU outside this study with this device, use of the intravascular cooling temperature device was discontinued at the hospital. The study protocol was modified to specify use of the external surface cooling pads for subsequently enrolled patients.
No perioperative bleeding complications were noted in those patients who underwent decompression surgery at the target temperature (33–34°C).
Patients were admitted to the ICU for the duration of the therapeutic hypothermia and rewarming phases. The mean length of intubation was 7.5 days and overall mean ICU length of stay was 16.8 days in the motor complete cohort. Five patients required antishivering measures, including additional sedation and three required administration of a neuromuscular blocking agent to suppress shivering. Following rewarming, three patients had temperatures >38°C. Two of these patients had VAP while the third patient had no clear infection causing fever.
Clinical outcome
Neurological recovery was determined by comparing the initial ASIA grade with the ASIA grade 6 months postinjury. All motor complete patients with ongoing enrollment were initially evaluated as ASIA grade A in hospital after having been assessed as having a SPEED motor and sensory score of 0 by paramedics at the accident scene. Of the five motor complete patients, one remained ASIA A, one recovered to ASIA B, and three recovered to ASIA C by 6 months postinjury.
In a previous study of early paramedic neurological assessment of patients with suspected SCI (10), there were 34 patients who were evaluated as SPEED = 0 at the accident scene and ASIA grade A on arrival in hospital and thus were initially the same severity as the population of motor complete patients in the current study. Four (12%) of these patients improved by two grades (average time to decompression 25 hours). Using Fishers exact test, the proportion of patients in our study (60%) demonstrating a two-grade recovery in the current study was significantly higher than in this retrospective control group (p = 0.03). However, we do not have complete data on the baseline demographics of this control group to allow a statistical comparison.
Discussion
This preliminary clinical study demonstrates the safety and feasibility of initiating therapeutic hypothermia in the prehospital setting in patients with cervical SCI using bolus large-volume, ice-cold saline. Of note, no patient developed pulmonary edema using this approach and there was a 1.1°C decrease in temperature during prehospital care. Subsequent mechanical cooling was initiated to provide a target temperature of 34°C, which was achieved in 6 hours. The induction of therapeutic hypothermia was followed by early decompressive surgery (mean 8.1 hours) in patients with motor complete injuries and no unexpected complications were reported, in particular there was no excessive bleeding.
There are a number of preclinical trials that show supportive data for the use of therapeutic hypothermia in SCI. A recent meta-analysis reviewed 11 animal studies employing systemic hypothermia with 10 studies using surface cooling, and one using a cooling chamber (Ransom et al., 2022). Each of these animal studies found improvement in at least one aspect of neurological function compared with normothermic controls.
There are two clinical trials that have reported the use of therapeutic hypothermia after SCI but both have commenced cooling after hospital arrival. In a study by Dididze et al. (2013), 35 patients underwent systemic therapeutic hypothermia using an intravascular mechanical device with an average time to target temperature (33°C) of 7.76 hours. The complications in that study were mostly respiratory, including atelectasis in 83%, pneumonia in 60%, pulmonary edema in 43%, and acute respiratory distress syndrome in 11%. Thirteen patients (37%) developed urinary tract infections. Five patients had thromboembolic events and two patients developed transient cardiac asystole. However, there was no normothermic control patients to determine whether therapeutic hypothermia changed the rate of complications or improved outcomes.
The only randomized, controlled trial to date comparing therapeutic hypothermia (target 33°C) with normothermia (target 37°C) was reported by Vedantam et al. (2022). In that study, 50 patients with SCI who were admitted to one of five trauma centers in the United States were allocated to either therapeutic hypothermia initiated within 24 hours (27 patients) or normothermia (23 patients). The actual time to target temperature was not reported in that article, however the trial protocol required insertion of an intravascular cooling catheter within 24 hours. The main complications were respiratory complications seen in 55.6% of patients treated with hypothermia compared with 52.2% in the control patients (p = 0.81) and deep venous thrombosis seen in 14.8% of the hypothermia patients compared with 17.4% in the control patients (p = 0.71). This clinical trial is still recruiting, thus overall neurological outcomes in the two groups of patients are not yet reported.
The technique for induction of therapeutic hypothermia after hospital arrival has usually involved the IV cooling temperature catheter. However, the use of this device is associated with an increased risk of venous thrombosis, which was a complication seen in one patient in our study. In a study of 75 patients managed with an IV catheter temperature control catheter, the incidence of this complication has been shown to be 12/75 (16%) (Andremont et al., 2018).
In our study, hypothermia was combined with early surgery because preclinical data suggest that cooling prolongs the time available for decompression (Batchelor et al., 2010). Clinical studies examining decompression within 24 hours of injury are consistent in demonstrating benefit. In a meta-analysis, 15 studies in 1126 patients were reviewed with early surgery defined as <24 hours after injury (Ter Wengel et al., 2019). The main finding was that patients with complete cervical SCI (n = 422) had more frequent neurological improvement after early surgery than after later surgery (OR 2.6, 95% CI: 1.4–5.1).
Whether still earlier decompression further improves outcome is less certain. In a meta-analysis of four separate datasets, functional outcome data at 1 year after SCI in 1548 patients were reviewed (Badhiwala et al., 2021). Early surgery in that review was defined as <12 hours after injury. Patients who underwent early surgical decompression (n = 528) had better AIS grades at 1 year compared with those patients (n = 1020) who had later decompression surgery (OR 1 · 48, 95% CI 1.16–1.89; p = 0.0019).
On the other hand, in a study of very early decompressive surgery (<5 hours after injury) in 33 patients compared with early (5–24 hours) in 13 patients, there was improvement by two AIS grades observed in 31% in the early group compared with only 6% of the patients in the very early group (p = 0.03; relative risk, 5.2; 95% CI 1.1–35) (Mattiassich et al., 2017).
However, none of the above studies assessing the benefit of the timing of decompressive surgery adjusted the outcomes for differences in temperature management, thus it is unknown whether early or later therapeutic hypothermia before very early, early, or late decompressive surgery is beneficial.
Our study suggests that very early (prehospital) initiation of therapeutic hypothermia followed by early decompressive surgery (<8 hours) is worth exploring further as an approach, which is feasible and safe and needs further testing to determine whether it results in better outcomes. When compared with an historical control cohort treated in the same state and matched for initial injury severity, a significantly higher proportion of patients in our cooling trial with a motor complete injury improved by two AIS grades following treatment (60% vs. 12%, p = 0.03). Although our trial numbers were very small, this rate of recovery is better than the published usual rate of recovery in patients with ASIA A grade injury, where approximately only 10% of patients recover to ASIA B and 10% recover to ASIA C or D by 6 months postinjury (Ma et al., 2020).
Limitations
This study was small and a number of patients with incomplete SCI did not follow the study protocol. Also, we have used historical controls to compare outcomes, however that group may have differed from our patients in factors that affect outcomes, such as comorbidities, time to hospital, temperature management after hospital arrival, and time to surgery. Also, with respect to hospital temperature management after hospital arrival, we do not have sufficient data to determine whether intravascular cooling is faster and/or more effective than surface cooling/warming blankets. Finally, the demographics of SCI in our state may differ from that of other centers.
Conclusion
Overall, this preliminary study supports the feasibility and safety of prehospital cooling using large-volume, ice-cold saline to induce therapeutic hypothermia before early surgical decompression in patients with complete cervical motor SCI. A larger study of this approach in patients with motor complete cervical SCI compared with cooling after hospital arrival together with early decompression is needed to determine whether this approach improves outcomes.
Footnotes
Authors' Contributions
P.B.: Conceptualization, methodology (lead), and original draft (lead). S.B.: Conceptualization, and original draft (lead). D.G., A.U., and M.F.: Review and editing. J.B.: Data collection. P.S. and C.B.: Study management. M.S.: Paramedic education and support. K.S. and A.N.: Review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by grants from the National Health and Medical Research Council of Australia (NHMRC) and the Transport Accident Commission of Victoria (TAC). Stryker Australia Pty Ltd provided funding through the Alfred Foundation (Grant number: APP 1044894).