
Abstract
The Swiss National Asphyxia and Cooling Register was implemented in 2011. This study assessed quality indicators of the cooling process and (short-term) outcomes of neonates with hypoxic-ischemic encephalopathy (HIE) receiving therapeutic hypothermia (TH) longitudinally over time in Switzerland. This is a multicenter national retrospective cohort study of prospectively collected register data. Quality indicators were defined for longitudinal comparison (2011–2014 vs. 2015–2018) of processes of TH and (short-term) outcomes of neonates with moderate-to-severe HIE. Five hundred seventy neonates receiving TH in 10 Swiss cooling centers were included (2011–2018). Four hundred forty-nine (449/570; 78.8%) neonates with moderate-to-severe HIE received TH according to the Swiss National Asphyxia and Cooling Register Protocol. Quality indicators of processes of TH improved in 2015–2018 (compared with 2011–2014): less passive cooling (p = 0.013), shorter time to reach target temperature (p = 0.002), and less over- or undercooling (p < 0.001). In 2015–2018, adherence to performing a cranial magnetic resonance imaging after rewarming improved (p < 0.001), whereas less cranial ultrasounds were performed on admission (p = 0.012). With regard to quality indicators of short-term outcomes, persistent pulmonary hypertension of the neonate was reduced (p = 0.003), and there was a trend toward less coagulopathy (p = 0.063) in 2015–2018. There was no statistically significant change in the remaining processes and outcomes. The Swiss National Asphyxia and Cooling Register is well implemented with good overall adherence to the treatment protocol. Management of TH improved longitudinally. Continuous reevaluation of register data is desirable for quality assessment, benchmarking, and maintaining international evidence-based quality standards.
Introduction
Background
Birth asphyxia is still a major cause of neonatal mortality and may cause long-term neurological sequelae. Hypoxic-ischemic encephalopathy (HIE) arises from asphyxia of the brain and occurs in 1–8/1000 term neonates in industrialized countries (Douglas-Escobar and Weiss, 2015). Although several studies showed that therapeutic hypothermia (TH) improves the survival rate and the neurodevelopmental outcome of these neonates, there are still a lot of open research questions concerning HIE and TH ( Azzopardi et al, 2014; Azzopardi et al, 2009; Jacobs et al, 2013; Shankaran et al, 2012; Shankaran et al, 2005).
In 2011, the Swiss National Asphyxia and Cooling Register was established to register all term and near-term neonates with HIE (Brotschi et al, 2014; Hagmann et al, 2011). The register allows for comparison and benchmarking of processes and outcomes. There are 11 cooling centers offering TH for neonates with moderate-to-severe HIE in Switzerland, distributed all over the small country of 41,285 km2 with 8.6 million inhabitants. All cooling centers agreed on the Swiss National Asphyxia and Cooling Register Protocol based on a comprehensive literature review (Azzopardi et al, 2009; Brotschi et al, 2014; Hagmann et al, 2011; Shankaran et al, 2005). The unit representatives of the Swiss National Asphyxia and Cooling Register regularly agreed on evidence-based adaptations of the clinical practice guideline as indicated from initiation in 2011 until now. It thus warrants regular reassessment of the adherence to processes and analysis of short-term outcomes.
Objectives
The aim of this study was to evaluate processes of TH and (short-term) outcomes after TH in the Swiss National Asphyxia and Cooling Register since implementation over time. This study will help to identify processes and outcomes needing further improvement. The goal is to both streamline processes and enhance the care to improve outcomes of neonates with moderate-to-severe HIE in Switzerland, based on the current international evidence in the literature.
Materials and Methods
Study design, setting, and participants
Since 2011, neonates with HIE treated in 1 of 11 participating centers of SwissNeoNet are registered in the Swiss National Asphyxia and Cooling Register. All Swiss centers but one performing TH for moderate-to-severe HIE participated in this population-based retrospective cohort study of prospectively collected data. Therefore, the number of cooling centers included is 10. An ∼90% population coverage of all Swiss neonates receiving TH for HIE born between January 1, 2011, and December 31, 2018, was estimated. The data of neonates receiving off-protocol cooling due to clinical judgment of the attending neonatologist were analyzed separately and presented in the results before TH. They were consecutively excluded for the further processes and outcome analysis during and after TH. This was due to possible selection bias and to focus on process and outcome quality of neonates receiving TH according to protocol. Inclusion and exclusion criteria for TH according to the Swiss National Asphyxia and Cooling Register Protocol were applied (Supplementary Appendix S1).
Data sources, data collection, and variables
Division into two consecutive time periods
The goal of this study was to assess the adherence to the Swiss National Asphyxia and Cooling Register Protocol longitudinally over time. Therefore, the study period was divided into two consecutive time periods: (1) From initiation of the register in 2011 until the end of 2014 (2011–2014) and (2) 2015 until the end of 2018 when the quality task force of the Swiss National Asphyxia and Cooling Register was formed and agreed on this study (2015–2018).
Annual meetings of the unit representatives of the Swiss National Asphyxia and Cooling Register were held since the initiation in 2011. Minutes were sent out to all unit representatives to facilitate implementation at the local sites. Moreover, recommendations of the Swiss National Asphyxia and Cooling Register were shared with all practicing neonatologists in Switzerland by distributing a newsletter.
The division into these two consecutive time periods was explained by adaptations to the Swiss National Asphyxia and Cooling Register Protocol. In December 2014, the following recommendations arose from a unit representatives consensus meeting and alterations were made to the Swiss National Asphyxia and Cooling Register Protocol as of January 2015: Recommendation for active whole-body cooling (using servo-controlled cooling devices, set target temperature at 33.5°C) instead of passive whole-body cooling; eligibility for TH at ≥35 weeks of gestational age if cooling criteria met instead of ≥36 weeks of gestational age; recommendation to routinely perform cranial magnetic resonance imaging (cMRI) on all neonates after TH (independent of cranial ultrasound findings).
Baseline characteristics
Demographical perinatal and neonatal data were extracted from the Swiss National Asphyxia and Cooling Register. Severity of encephalopathy on admission was assessed using Sarnat scoring (Sarnat and Sarnat, 1976). Thompson scores to depict the severity of encephalopathy on admission were converted to Sarnat scores (Sarnat and Sarnat, 1976) according to Thompson et al (1997; Chansarn et al, 2021).
Quality indicators for processes and outcomes
The quality task force of the Swiss National Asphyxia and Cooling Register was formed in 2018. During several consensus meetings, quality indicators were developed and evaluated based on the data collected in the register. Definitions of the Swiss National Asphyxia and Cooling Register Protocol were applied throughout (Grass et al, 2021) (Supplementary Appendix S1 and Supplementary File S1). The following predefined standards were set based on the Swiss National Asphyxia and Cooling Register Protocol: target temperature during TH of 33.0–34.0°C; maximum time to reach target temperature of 7 hours after birth; limit for overcooling <33.0°C (at least 3 hours in succession); limit for undercooling >34.0°C (at least 3 hours in succession after TH target temperature reached and until rewarming started); target range for rewarming of 0.2–0.5°C per hour.
The developed quality indicators were separated into eight process and six (short-term) outcome quality indicators as per Donabedian (1988):
Process quality indicators
- Before TH: Off-protocol cooling (defined as cooling criteria not met or TH contraindicated);
- during TH: Passive whole-body cooling; time to reach target temperature for TH out of range (defined as more than 7 hours after birth); no cranial ultrasound performed on admission; amplitude-integrated electroencephalogram (aEEG) not performed during each day during TH and rewarming; over-/undercooling during TH;
- after TH: Temperature during rewarming not in range (speed of rewarming and variability); cMRI not performed between day of life 5–14.
Outcome quality indicators
- Arterial hypotension (requiring treatment) during TH and rewarming;
- seizures (clinical or electrographic) during TH and rewarming;
- infection (requiring antibiotic therapy; included pneumonia [consistent chest X-ray findings], culture-proven sepsis [early onset and late onset], and necrotizing enterocolitis [Bell stage 2–3]) before discharge;
- coagulopathy (any disorder requiring treatment to maintain or recover normal hemostasis according to unit's policy) before discharge;
- persistent pulmonary hypertension of the neonate (PPHN; confirmed by echocardiography and requiring treatment) before discharge;
- neonatal death before discharge (Grass et al, 2021).
Risk adjustment was performed for outcome quality indicators. Process quality indicators were expected to perform regardless of risk.
Statistical methods, ethics, and reporting
Baseline demographics, process, and outcome quality indicators were presented as absolute numbers and percentages for categorical variables, as mean (including standard deviation) for continuous, normally distributed variables, and as median (including interquartile range) for continuous, non-normally distributed variables.
A missing data analysis was performed, and the following standards were set for evaluation of data. Data completeness required per patient data set in temperature measurements: time to reach TH target temperature: 50% of all temperatures during hours 1–12 of TH; overcooling: 50% of all temperatures during hours 1–96 of TH; undercooling: 50% of all temperatures as of time point when TH target temperature was reached until rewarming started.
Data imputation was conducted based on plausibility: 16 neonates with unknown survival status were determined survivors by analysis of discharge data. One neonate with unknown birth location was determined outborn based on place of birth. One neonate with unknown status regarding major congenital malformations apparent at birth was determined not to have major congenital malformations as there was no mention of malformations in the remaining data set. With regard to data manipulation, all included neonates from one cooling center were reset to “passive cooling” after verification with the unit representative.
Dichotomous process and (short-term) outcome quality indicators were defined to generate standardized quality indicator evaluations. All analyses were performed on the national data set instead of de-identified center to center analyses.
Risk adjustment was performed for all outcome quality indicators, including male sex, small for gestational age (birth weight less than third percentile), Sarnat score on admission, composite pregnancy complication (maternal diabetes, maternal fever, or pre-eclampsia), and composite delivery sentinel events (placental abruption, ruptured uterus, shoulder dystocia, cord mishap, or head entrapment).
Chi square tests were used to test for differences of processes and outcomes between the two time periods. Differences between the two time periods were displayed using standardized mortality/morbidity ratio (SMR) charts in which SMR charts point estimate is a ratio between the observed events of a quality indicator for the period over expected events after indirect standardization toward the reference (entire time period). The reference set as 1 and the period's value per indicator is displayed in relation to the collective value with a 95% confidence interval. For each quality indicator, predefined standard included data completeness of 90% of the data required to be displayed in the SMR charts.
All analyses were performed in R version 3.6.1 (The R Foundation, 2021).
Data collection, analysis, and publication for this study were approved by the Swiss Association of Research Ethics Committees and the Swiss Federal Commission for Privacy Protection in Medical Research (PB 2016-02299).
STROBE guidelines were applied for reporting this study.
Results
Participants and descriptive data
Study population
In the study period between January 1, 2011, and December 31, 2018, 578 neonates were registered in the Swiss National Asphyxia and Cooling Register.
Five hundred seventy (570/578; 98.6%) neonates with HIE receiving TH in 10 centers were included in this analysis. One center did not provide sufficient data to the register, and data sets were thus excluded from this study (n = 8; 8/578; 1.4%).
Of the 570 included neonates with HIE receiving TH, 489 neonates survived until discharge (489/570; 85.8%). Of the 570 included neonates, 121 neonates (121/570; 21.2%) received off-protocol cooling (Table 1).
Study Population Receiving Therapeutic Hypothermia
Criteria for TH (A and B criteria to be met): A criteria: at least two of the following conditions: Apgar score ≤5 at 5 or 10 minutes and/or umbilical cord pH or pH within 1 hour ≤7.00 and/or base deficit ≥16 mmol/L and/or lactate ≥12 mmol/L and/or requirement of ongoing resuscitation in the delivery room >10 minutes. B criteria: Sarnat score >1 or Thompson score ≥7. Contraindications for TH (any to be met): gestational age <35 weeks; >6 hours of age at initiation of TH; major congenital malformation; severe growth restriction: birth weight <2000 g and head circumference less than −2 SD for gestational age.
SD, standard deviation; TH, therapeutic hypothermia.
Baseline characteristics
Throughout the whole study period, off-protocol cooling was the main limiting factor regarding adherence to protocol, occurring approximately in one fifth of the cases in both time periods (Table 1). The driving force of this deviation to protocol was not meeting the B criteria for TH, that is, less severity of encephalopathy reflected as Sarnat score 1. Off-protocol cooling due to Sarnat score 1 on admission occurred in 62% (75/121) of those receiving TH off-protocol.
A total of 449 (449/570; 78.8%) neonates with moderate-to-severe HIE received TH according to the Swiss National Asphyxia and Cooling Register Protocol in both time periods.
Baseline characteristics are depicted in Table 2.
Baseline Characteristics of the Study Population (of Neonates Receiving Therapeutic Hypothermia According to the Protocol)
Small for gestational age = birth weight less than third percentile; composite pregnancy complication = maternal diabetes, maternal fever, or pre-eclampsia; composite delivery sentinel events = placental abruption, ruptured uterus, shoulder dystocia, cord mishap, or head entrapment. n = 449 analyzed data sets (TH according to protocol); missing data excluded for the following variables: Apgar score at 1 minute n = 441 (441/449; 98%), Apgar score at 10 minutes n = 439 (439/449; 98%), arterial cord pH <7.00 n = 372 (372/449; 83%), base deficit ≥16 mmol/L n = 352 (352/449; 78%).
IQR, interquartile range.
Outcome data and main results
Process quality indicators
Quality indicators for processes were evaluated for both time periods (Table 3). Standardized morbidity/mortality charts are presented in Figure 1. All analyses were unadjusted since process quality indicators were expected to perform regardless of risk.
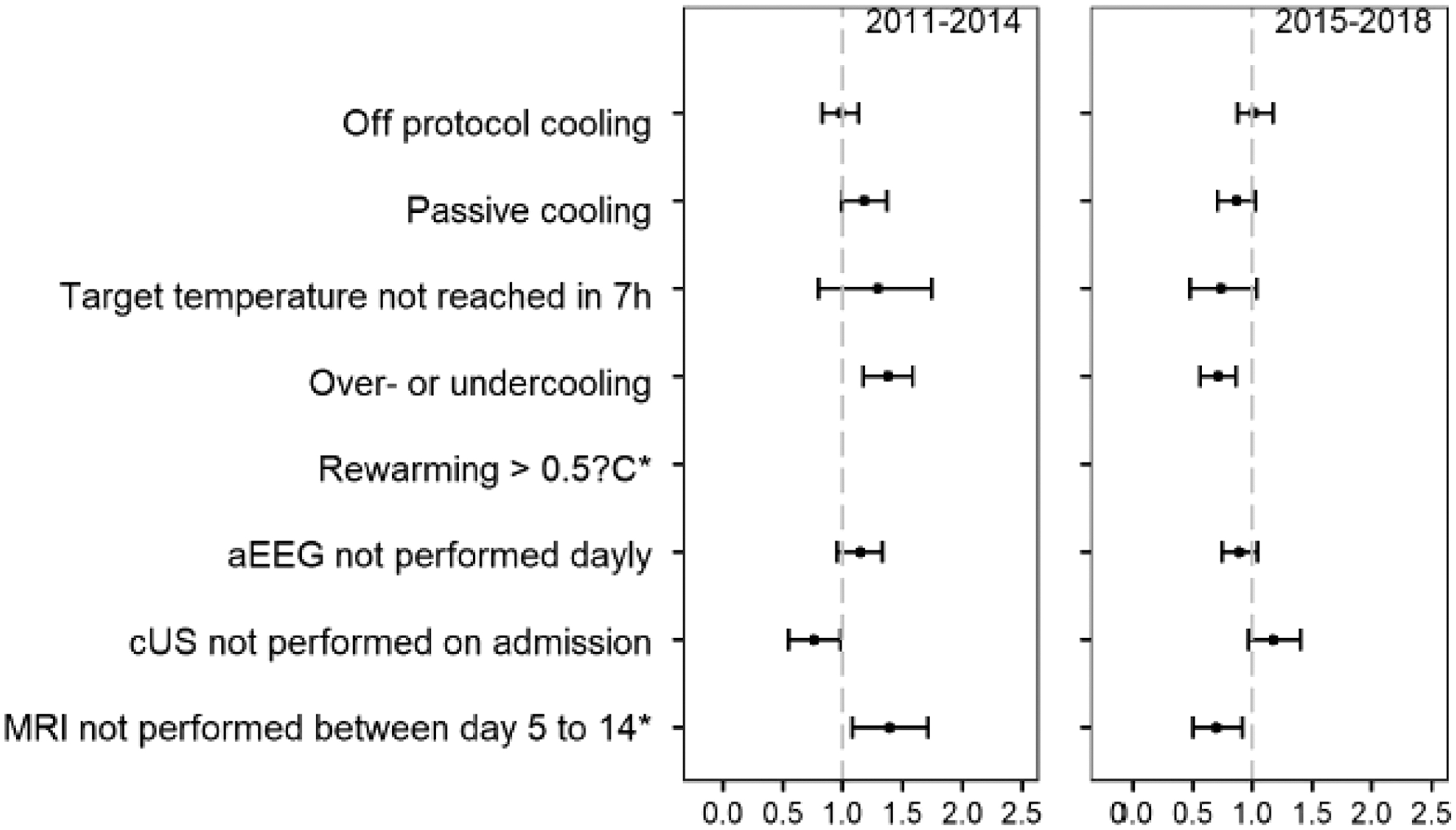
Standardized morbidity/mortality chart for quality indicators of processes. *Quality indicators with <90% of the data required were not represented in this standardized morbidity/mortality chart. aEEG, amplitude-integrated electroencephalogram; cUS, cranial ultrasound; MRI, magnetic resonance imaging.
(Quality Indicators of) Processes
Off-protocol cooling = cooling criteria not met or TH contraindicated; temperature on admission = temperature on admission to the center providing TH (prior passive cooling possible); time to reach TT for TH out of range = TT not reached within 7 hours; insufficient temperature monitoring first 12 hours = less than 50% of all temperatures during hours 1–12 of cooling. Sample sizes: before TH: n = 570 analyzed data sets (whole study population); no missing data. During TH: n = 449 analyzed data sets (TH according to protocol); missing data excluded for the following variables: temperature on admission n = 422 (422/449; 94%), time to reach TT for TH n = 435 (435/449; 97%), time to reach TT out of range n = 435 (435/449; 97%), over- or undercooling n = 433 (433/449; 96%). After TH: n = 376 analyzed data sets (survivors); missing data excluded for the following variables: rewarming per hour n = 257 (257/376; 68%), rewarming >0.5°C n = 252 (252/376; 67%).
Quality indicator.
aEEG, amplitude-integrated electroencephalogram; cMRI, cranial magnetic resonance imaging; TT, target temperature.
(Short-term) outcome quality indicators
Quality indicators for (short-term) outcomes were investigated for both time periods (Table 4). Standardized morbidity/mortality charts are depicted in Figure 2. All analyses were risk adjusted for male sex, small for gestational age (birth weight less than third percentile), Sarnat score on admission, composite pregnancy complication (maternal diabetes, maternal fever, or pre-eclampsia), and composite delivery sentinel events (placental abruption, ruptured uterus, shoulder dystocia, cord mishap, or head entrapment).

Standardized morbidity/mortality chart for quality indicators of (short-term) outcomes. PPHN, persistent pulmonary hypertension of the neonate.
Quality Indicators of (Short-Term) Outcomes
Outcome definitions according to the Swiss National Asphyxia and Cooling Register (Grass et al, 2021) (Supplementary Appendix S1 and Supplementary File S1). Infection: infections requiring antibiotic therapy consisted of pneumonia (consistent chest X-ray findings), culture-proven sepsis (early onset and late onset), and necrotizing enterocolitis (Bell stage 2–3) (Grass et al, 2021). n = 449 analyzed data sets (TH according to protocol) for all variables, no missing data.
PPHN, persistent pulmonary hypertension of the neonate.
Discussion
Statement of principal findings
This multicenter retrospective cohort study of prospectively collected data of the Swiss National Asphyxia and Cooling Register between 2011 and 2018 confirms feasibility, implementation, and overall adherence to the standardized clinical practice guideline for neonates with moderate or severe HIE receiving TH across Switzerland.
Differences in baseline characteristics, processes, and outcomes were identified between an earlier and a later time period. Processes and (short-term) outcomes served as quality indicators to assess longitudinal change between the two time periods. Adaptations to the Swiss National Asphyxia and Cooling Register Protocol based on arising evidence in the literature and discussed among the unit representatives of the Swiss National Asphyxia and Cooling Register were successfully implemented in the later time period: eligibility for TH at ≥35 weeks of gestational age, application of active servo-controlled whole-body cooling, and emphasis on routine neuroimaging with cMRI after rewarming.
Interpretation within the context of the literature
This study was completed by the quality task force of the Swiss National Asphyxia and Cooling Register in context of a triad of quality improvement analyses (Adams et al, 2021; Grass et al, 2021). It aimed to assess the implementation and usefulness of the Swiss National Asphyxia and Cooling Register with the management protocol over time. The need for national guidelines and a national patient register for HIE was supported by other European countries with comparable neonatal care (Gerstl et al, 2015) and also by international neonatal networks (Pfister et al, 2012).
Criteria for off-protocol cooling in this multicenter study were in agreement with findings of a single-center study (Carlton et al, 2020). This deviation from protocol was comparable in magnitude to previous studies of HIE populations (Carlton et al, 2020). TH for mild HIE (Sarnat score 1) is a drift in practice recently reported in many countries (Beltempo et al, 2022; Shipley et al, 2021; Yieh et al, 2022). Although there are published data that neonates with mild HIE showed abnormal neurodevelopmental outcome (Aoki et al, 2021; Conway et al, 2018; Prempunpong et al, 2018; Walsh et al, 2017), there is no evidence of the benefit of TH for mild HIE yet and results of randomized controlled trials are pending (Bonifacio, 2022; Chawla et al, 2020; Garcia-Alix et al, 2023; Saw et al, 2019).
The register reflected the reality of clinical decision-making. Senior attending neonatologists decided to start off-protocol cooling for Sarnat score 1 based on the clinical context and the expected trajectory. Moreover, clinical assessment of severity of HIE remains a challenge and might reflect some inter-rater variability when performing Sarnat scoring on admission (Bhagwani et al, 2016; Natarajan et al, 2018).
Some process quality indicators of TH showed longitudinal improvement in the later time period. Active cooling using servo-controlled cooling devices became standard of care with only a quarter of cases receiving passive cooling during the later time period (p = 0.013). Less over- and undercooling (p < 0.001) and shorter times to reach target temperature of TH (<4 hours, p = 0.002) might be associated with the implementation of active cooling in the later time period and were in agreement with previous reports (Brotschi et al, 2015).
Earlier identification of eligible cases and thus reaching target temperature of TH earlier was one of the aims flagged by a previous report of this quality task force (Adams et al, 2021). Meeting this goal over time was probably due to a learning process and increasing routine with TH, combined with ongoing outreach education of the cooling centers. This is of importance since reaching target temperature of TH is time-sensitive (Jacobs et al, 2013; Thoresen et al, 2013). Furthermore, precision of temperature management is associated with less brain injury on cMRI (Brotschi et al, 2017) and thus might possibly result in improved neurodevelopmental outcomes.
The prognostic value of findings on cMRI after rewarming was reemphasized in the annual meeting of the unit representatives at the end of 2014. A statistically significant rise in completion of a cMRI in the later time period (as of 2015) was thus very encouraging (p < 0.001). Findings from neuroimaging with cMRI were reported to be of value for neurodevelopmental outcome prognostication (Bach et al, 2021; Weeke et al, 2018), which again is essential for counseling families of a neonate with HIE after completion of TH. While completion of a cMRI increased in the later time period, performing a cranial ultrasound on admission, ideally before initiation of TH, decreased.
However, a cranial ultrasound on admission is warranted to rule out other underlying etiologies causing neonatal encephalopathy (such as perinatal stroke, intraventricular hemorrhage) (Glass, 2018; Mohammad et al, 2020; Russ et al, 2021). TH is not indicated for any etiologies of neonatal encephalopathy besides moderate-to-severe HIE (Glass, 2018; Russ et al, 2021), and cranial ultrasound helps distinguishing etiologies. Reinforcement of further education on the different indications for a cranial ultrasound on admission compared with the indication for a cMRI after rewarming is planned to improve complementary neuroimaging in this HIE population in the near future.
The investigation of the majority (5/6; 83%) of the (short-term) outcome quality indicators did not reveal any statistically significant change in outcomes between the two time periods. Severity of HIE was comparable in both time periods. The rates of arterial hypotension, seizures, infection, and death remained stable over time. One possible interpretation is that the majority of these outcomes are a direct disease burden of HIE itself and thus less modifiable by management during TH (Jacobs et al, 2013). Further details on these four outcomes were described previously in the outcome focused analysis of the quality task force initiative (Grass et al, 2021).
PPHN and coagulopathy instead were also described in association with the nature of HIE; however, both these outcomes are sensitive to temperature changes. There were trends in the direction of more morbidity with TH (Jacobs et al, 2013). Less PPHN in the later time period might be due to growing experience with TH, and proactive management of TH (including analgosedation) might help to avoid PPHN during TH. A trend toward less coagulopathy in the later time period might be associated with higher rates of active cooling, leading to less temperature instability, especially less overcooling, in the later time period.
Implications for policy, practice, and research
This longitudinal evaluation of the implementation of the Swiss National Asphyxia and Cooling Register assessed the adherence to the standardized protocol across Switzerland. The analysis of the register data showed that the implementation of the register improved patient management over time. However, it is crucial to regularly reassess the relevance of the Swiss National Asphyxia and Cooling Register to ensure that it remains up to date and fit for purpose. It was important to ensure that guidelines developed from research findings were applicable to clinical practice. Investigations such as this quality task force initiative generated peer review, open discussion, and led to adjustments in the protocol as indicated. Furthermore, it was a great opportunity to benchmark and provide feedback to the cooling centers.
Open research questions include the value of off-protocol cooling especially for Sarnat score 1 on admission. Testing the process and (short-term) outcome quality indicators for an association with long-term neurodevelopmental outcome is highly recommended as a next step.
Strengths and limitations
This was a national multicenter analysis of prospectively collected data of neonates receiving TH registered in the Swiss National Asphyxia and Cooling Register since 2011. This approach led to a high numbers of included study participants. The retrospective cohort design reflected real-life conditions and can be considered a population-based study. The number of neonates eligible for TH but not treated with TH remained unknown. However, it was estimated to be very low based on the high awareness for HIE, the clinical setting, and infrastructure in Switzerland.
This study benefited from the harmonized national application of a standardized clinical practice guideline in a well-described cohort of included neonates with moderate-to-severe HIE receiving TH. The Swiss National Asphyxia and Cooling Register followed standardized, however, single data entry. Data monitoring was performed regularly. This resulted in a high completeness of data sets for most variables of this study. Data completeness was lower for data during the rewarming phase. To minimize bias, standardization and risk adjustment were performed, and denominators were stated throughout.
The goal of this study was a longitudinal national quality assessment. Individual center-specific analyses were not performed. However, unit-identified data are available to the individual centers, can be used for benchmarking, and lead to local change. The ambiguity of some of the definitions of the short-term outcomes (e.g., coagulopathy) was a weakness and might have impacted coding of these outcomes upon data entry. As discussed in the associated publication by Grass et al (2021), the definitions of arterial hypotension and seizures have thus been further specified. Evaluation of unit-specific treatment protocols for these short-term outcomes and development of a standardized HIE care bundle is warranted as a next step. This study was restricted to short-term outcomes only, and long-term neurodevelopmental outcomes were not evaluated.
Conclusions
The Swiss National Asphyxia and Cooling Register Protocol is well implemented throughout Switzerland. Longitudinal data evaluation showed quality improvement in TH management over time. Off-protocol cooling and adherence to neuroimaging guidelines are areas for further improvement. The register is warranted for quality assessment and quality improvement and to consider adaptations to the treatment protocol based on new arising evidence.
Ethics Approval and Consent to Participate
Data collection, evaluation, and publication for this study were approved by the Swiss Association of Research Ethics Committees and the Swiss Federal Commission for Privacy Protection in Medical Research (KEK-ZH-Nr2014-0551 and KEK-ZH-Nr2014-0552).
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
We would like to thank the following data managers for entering data into the Swiss National Asphyxia and Cooling Register: Rahel Kusche (Aarau), Barbara Imboden (Lucerne), Tanja Wachinger (St. Gallen).
Collaborators—The Swiss National Asphyxia and Cooling Register: Aarau: Cantonal Hospital Aarau, Children's Clinic, Department of Neonatology (P. Meyer, G. Zeilinger, G. Konetzny); Basel: University Children's Hospital Basel (UKBB), Department of Neonatology (S.M. Schulzke, S. Wellmann, M. Hug); Berne: University Hospital Berne, Department of Pediatric Intensive Care (T. Riedel, T. Humpl, B. Wagner, K. Daetwyler, S. Pilgrim, M. Hug, M. Moegel); Chur: Children's Hospital Chur, Department of Neonatology (B. Rogdo, W. Bär, B. Scharrer, N. Binz); Lausanne: University Hospital (CHUV), Department of Neonatology (A. Truttmann, J.-F. Tolsa, A. Torregossa, J. Schneider); Lucerne: Children's Hospital of Lucerne, Neonatal and Pediatric Intensive Care Unit (M. Stocker, T. M. Berger, M. Fontana, K. Schwendener); St. Gallen: Children's Hospital St. Gallen, Neonatal and Pediatric Intensive Care Unit (A. Birkenmaier, J. P. Micallef, I. Hoigné); Winterthur: Clinic of Neonatology, Cantonal Hospital Winterthur (L. Hegi, M. Kleber); Zurich: University Hospital Zurich, Department of Neonatology (D. Bassler, G. Natalucci, M. Adams, U. Jochumsen, S. Boettger); and University Children's Hospital Zurich, Department of Intensive Care and Neonatology (L. Schlapbach, B. Frey, V. Bernet, C. Hagmann, B. Brotschi, B. Grass, R. Bolt).
Authors' Contributions
All authors made the conception of the study. A.B., B.B., and B.G. designed the study in detail. A.B. was responsible for acquisition of data, data analysis and interpretation, search and review of literature, and drafting of article. V.R., M.K., and K.S.S. helped with the acquisition of data. M.A. performed all statistical analyses of the study, interpreted results, and critically revised the article. B.G., B.B., and C.H. supervised the design of the study, data analysis and interpretation, search and review of literature, and critical review of article. All authors have read and approved the final article.
Author Disclosure Statement
The authors declare that they have no potential, perceived, or actual competing interest.
Funding Information
No funding was obtained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.