
Abstract
Cerebral tissue oxygen saturation (CrSO2) measured with near-infrared spectroscopy (NIRS) technology has recently become the subject of several research studies. The aim of this study was to investigate the diagnostic value of CrSO2 measurements in perinatal asphyxia (PA) cases. The study included a patient group of 42 PA cases, who were to be applied with therapeutic hypothermia (TH), and a control group of 42 healthy term newborns. PA cases were determined as moderate or severe encephalopathy (Sarnat score stage II or III) in clinical evaluation. In both groups, left (CrSO2L) and right (CrSO2R) NIRS measurements were taken for 10 minutes on the scalp. The arithmetic mean value of measurements was calculated and compared. The mean measurements were CrSO2R 67.38 ± 9.39 and CrSO2L 66.73 ± 7.76 in the patient group, and CrSO2R 80.28 ± 8.04 and CrSO2L 79.14 ± 8.49 in the control group. The mean CrSO2R and CrSO2L measurements of the patient group were statistically significantly lower than those of the control group (p < 0.001). In the Pearson correlation analysis, a significant correlation was determined in the patient group between cord blood gas pH and CrSO2R (r: 0.539, p < 0.001) and CrSO2L (r: 0.54, p < 0.001). For a cutoff value of CrSO2L ≤ 72%, the positive predictive value was 80 and the negative predictive value was 84.6. For a cutoff value of CrSO2R ≤ 74%, the positive predictive value was 79.5 and the negative predictive value was 82.5. Low CrSO2 measurements obtained with the NIRS method in PA cases to be applied with TH together with cord blood gas parameters can be considered a helpful parameter in diagnosis.
Introduction
Intrapartum-related hypoxic events can cause perinatal asphyxia (PA), and this is one of the leading causes of perinatal mortality (Martinello et al., 2017; McAdams and Juul 2016). The pathophysiology of PA is based on disruptions occurring in ventilation at the pulmonary level because of insufficient gas exchange in the placenta or postnatal events (Muniraman et al., 2017; Rakesh et al., 2018; Tanigasalam et al., 2016). Consequently, oxygen and carbon dioxide exchange is impaired and arterial hypoxemia, hypercarbia, and acidosis develop. As a result of this pathological process, the functions of several tissues and organs are impaired (Rakesh et al., 2018; Tanigasalam et al., 2016).
To minimize the complications of PA, therapeutic hypothermia (TH) is currently widely used (Natarajan et al., 2016; Papile et al., 2014). This treatment method leads to a reduction in neonatal mortality and neurological sequelae, and has become a part of standard treatment (Liu et al., 2017). For the planning of TH, the treatment criteria of blood gas pH or base deficit (BD) must be in a range appropriate for hypothermia treatment (Burnsed and Zanelli, 2017; Datta, 2017). When blood gas pH is ≤7 and/or BD ≤ −16 mmol/L, TH is applied to moderate and severe PA cases (Burnsed and Zanelli, 2017; Datta, 2017).
Together with the decision for TH application, pH and BD obtained from blood gases are known to be parameters indicative of survival and morbidity (Knutzen et al., 2015; Martí Gamboa et al., 2017). Although there several assistive markers and amplitude-integrated electroencephalography (aEEG), when blood gas parameters do not fully meet the decision for TH, several clinical difficulties are encountered. (Arnaez et al., 2018; Bustamante-Hervás et al., 2022; Jones et al., 2018; Kazanasmaz and Gumus, 2020).
Near-infrared spectroscopy (NIRS) noninvasively measures regional tissue oxygen saturation (rSO2) of various organs. rSO2 imaged as a percentage (from 0% to 100%) is the measurement of the level of regional tissue oxygen saturation in local deep tissue in the sensor region. Cerebral tissue oxygen saturation (CrSO2) obtained regionally with NIRS has recently become the subject of research in several pathological conditions related to the central nervous system (CNS) (Abramo et al., 2013; Arnaez et al., 2018; Gumulak et al., 2017; Kinoshita et al., 2015). Although the changes occurring in CrSO2 in hypoxic conditions affecting the CNS have been shown in clinical studies, there is no consensus on this subject as yet. The aim of this study was to compare the CrSO2 values of PA cases before TH with those of healthy infants and to evaluate the benefit of CrSO2 as a parameter in the diagnosis of PA.
Materials and Methods
This prospective study was conducted in the neonatal intensive care unit (NICU) in Turkey. This study complies with the principles of the 2008 Declaration of Helsinki and was approved by the local Ethics Committee of Harran University, Medical Faculty, in Turkey (Approval date and number: 18.10.2021, Session 18, 76884). Written informed consent was obtained from the parents of patients who participated in this study.
Patient selection
The study included a total of 84 subjects, as a study group of 42 cases with PA and a control group of 42 healthy infants. The PA patients were those who were admitted to the NICU for TH administration within the first 6 hours of life. TH was applied as whole body cooling (Arctic Sun® 5000 Temperature Management System) for 72 hours to PA patients with gestational age ≥36 weeks, within the first 6 hours of life (≤6), with blood pH ≤7.00 in blood gas measured from cord blood and/or BD ≤−16 mmol/L, to those with 10-minute Apgar scores of <5 and/or those with ongoing need for resuscitation, and to those with moderate or severe encephalopathy (Sarnat score stage II or III) in clinical evaluation (Burnsed and Zanelli, 2017; Datta, 2017).
The voluntary control group cases were selected from healthy newborns in the first 6 hours of life in the general population matched to the study group in terms of gender, gestational age at birth, and birthweight.
Cerebral regional oxygen saturation was monitored noninvasively and continuously with NIRS using MASIMO O3 Regional Oximetry (Masimo Corporation, Irvine, CA). Two probes were attached to the forehead bilaterally. At the stage of preparation for TH, measurements taken by the device throughout 10 minutes were recorded. As soon as the TH was started, the measurements were terminated. The results of the measurements obtained separately from the two probes on the right (CrSO2R) and left (CrSO2L) sides were analyzed on a computer and the arithmetic mean value was obtained.
At the same time, as the CrSO2 measurements were being taken, heart rate per minute and oxygen saturation (SpO2) values were recorded with a pulse oximetry probe (Rainbow Pulse CO-Oximeter; Masimo, Irvine, CA) over the skin for 10 minutes and the results were analyzed and the arithmetic mean values were obtained. All infants measured were within the first 6 hours of their lives.
Exclusion criteria
As defined in the manufacturer's instructions, exclusion criteria included conditions that could affect the measurement results such as improper sensor application or the use of incorrect sensor, intravascular dyes such as indocyanine green or methylene blue or externally applied coloring (such as indelible ink), venous congestion and pooled blood under the skin, moisture, birthmarks, skin discoloration or foreign objects (e.g., metal plate) in the light path, a physiological condition that may affect vasomotor tone or change invasomotor tone, excessive ambient light, high intensity light, or direct sunlight, adjacent placement of optical sensors not connected to the same O3® Module, and abnormal venous pulsations (e.g., tricuspid value regurgitation, Trendelenburg position). Cases were also excluded if there was a pathological condition such as hemoglobinopathy, anemia, cardiac arrest, or hypotension, or any condition related to movement (crying, etc.) so that continuous measurements of the sensor could not be made.
The working principle of the NIRS device
The working principle of the O3 Regional Oximeter System (O3 System) is based on the the reflection of spectroscopy scattered at multiple distances. The O3 System examines the microvasculature in cross-sections of tissue (a mixed base formed of arteries, capillaries, and venules) using light and the light returning after having passed through the tissue is analyzed. The Masimo O3 Regional Oximeter device contains a light diffuser and several detectors. More than one lightwave (4 wavelength light emitting diodes [LEDs]) is radiated to pass through the relevant region, and by the system measuring the length of these lightwaves with photo detectors after they have passed through the tissue, the reduction occurring in each lightwave is calculated. These optic decreases are then mapped on rSO2 (Beard, 2011).
The Masimo O3 Regional Oximetry System has a common diffuser and two detectors placed separately from each other at different distances from the diffuser. The shallow detector in the two-detector system is closer to the diffuser (LEDs) and obtains optic signals passing through relatively more superficial tissue, while the deep detector is further from the diffuser and, in addition to the surface layers, obtains optic signals passing through deeper tissue (Fig. 1). The O3 sensors formed from a single diffuser and two detectors are adhesive sensors for single patient use.

Schematic of an example of a regional oximeter sensor measuring deep tissue oxygenation.
Endpoints
The primary endpoint of the study was to evaluate the correlation between CrSO2 measurements of patients with PA (pre-TH) and cord blood gas parameters (pH and BD). Secondary endpoints were the relationships between absolute values and changes in rSO2 among before TH time points.
Statistical analyses
Statistical analysis was performed using SPSS version 24.0 (SPSS Inc., Chicago, IL). Power analysis was performed by using G*Power v3.1.9.4 to detect the sample size. It was selected for α-level 0.05 and for β-level 0.20 (power is 80%). Descriptive statistics were summarized as number, percentage, median (minimum–maximum), and mean and standard deviation. The suitability of variables to normal distribution was investigated using visual (histogram and probability graphs) and the Kolmogorov–Smirnov test.
Continuous variables were analyzed with either Student's t-test or Mann–Whitney U-test depending on distribution and homogeneity of data. Pearson correlation testing was used to investigate the relationship between parameters. Correlation coefficient (r) was found as a result of Pearson correlation analysis. Repeated-measures analyses were performed using generalized estimating equations (GEE) method. Specificity and sensitivity analysis were performed by using receiver operating characteristic (ROC) curve analysis technique. In the ROC analysis, the area under the curve values was studied. Comparisons were considered statistically significant when the probability (p) value was less than 0.05 (p < 0.05).
Results
A total of 84 cases were included in the study. Forty-two cases were in the group of patients with PA planned to be administered TH, and 42 were in the control group consisting of healthy infants. Gender and week of delivery distribution of both groups were similar (Table 1). There was no significant difference between the mean birth weights, mean measurement time, median HR, and median SpO2 of the groups (Table 1).
Comparison of Demographic Characteristics and Measurement Results of Study Groups
Bold value emphasizes that statistically the values are very significant (p < 0.001).
Pearson chi-square test.
Independent sample t-test.
Mann–Whitney U test.
BPM, beats per minute; CrSO2L, cerebral tissue oxygen saturation left; CrSO2R, cerebral tissue oxygen saturation right; SD, standard deviation
When the umbilical cord arterial blood gas analysis results of infants in the patient group treated with TH were examined, the mean pH value was 6.93 ± 0.09 and the mean BD value was 17.81 ± 3.8 (Table 1). All the patients in the patient group received respiratory support. Invasive mechanical ventilation (IMV) was applied to 40 cases, while noninvasive continuous positive airway pressure (CPAP) ventilation support was applied to 2 cases. Noninvasive CPAP support (one case for 4 days and the other for 2 days) was given to only two patients. The mean duration of stay in IMV was 15.21 ± 12.97 days. The mean length of stay in the NICU was 30.79 ± 16.55 days.
A significant difference was observed between groups in the mean CrSO2R and CrSO2L measurements (Fig. 2). The mean CrSO2R measurement was 67.38 ± 9.39 in the patient group and 80.28 ± 8.04 in the control group. CrSO2R was significantly higher in healthy controls than in patients with PA (p < 0.001) (Table 1). Similarly, the mean CrSO2L measurement was 66.73 ± 7.76 in the patient group and 79.14 ± 8.49 in the control group. CrSO2L was significantly higher in healthy controls than in patients with PA (p < 0.001). When the mean CrSO2R (73.83 ± 10.84) and CrSO2L (72.94 ± 10.2) measurements of 84 participants were compared with the paired sample t-test, the measurement results were found to be similar (p = 0.214). There was a positive correlation between CrSO2R and CrSO2L in the Pearson correlation analysis (r: 0.81, p < 0.001).

CrSO2R and CrSO2L distribution according to the measurements results. CrSO2L, cerebral tissue oxygen saturation left; CrSO2R, cerebral tissue oxygen saturation right.
There was no significant correlation relationship between CrSO2R measurements and birth week (r: 0.04, p: 0.65) and birth weight (r: −0.06, p: 0.53). Similarly, there was no significant correlation relationship between CrSO2L measurements and birth week (r: 0.06, p: 0.59) and birth weight (r: −0.02, p: 0.98). A significant correlation was observed between CrSO2R, CrSO2L, pH, and BD levels in the patient group. The Pearson correlation analysis revealed a negative correlation between the pH and BD measurements (r: −0.535, p < 0.001). Moreover, a positive correlation was found between pH and CrSO2R (r: 0.539, p < 0.001) and pH and CrSO2L (r: 0.54, p < 0.001) measurements. There was no significant relationship between BD and CrSO2R and CrSO2L measurements (p > 0.05).
The GEE method was used with independent gender and group variables for repeated longitudinal measurements of CrSO2R and CrSO2L. The gender variable was found to be insignificant in both CrSO2R and CrSO2 L measurements in the GEE model. However, the group variable was found to be significant in the GEE model (Table 2).
Generalized Estimation Equation Univariate Model for Analyzing the Impact of Each Variable on Repeated CrSO2R and CrSO2L Measurements
Set to zero because this parameter is redundant.
CI, confidence interval.
ROC curves were plotted to compare predictive values of CrSO2R and CrSO2L in the diagnosis of PA for 84 participants (Fig. 3). When a cutoff value of ≤72% CrSO2L was used in the prediction of PA, sensitivity and specificity were 85.71% and 78.57%, respectively, and positive and negative predictive values were 80 and 84.6, respectively (Table 3). A cutoff value of ≤74% used for CrSO2R had sensitivity of 83.33% and specificity of 78.57% in the prediction of PA with positive and negative predictive values of 79.5 and 82.5, respectively.
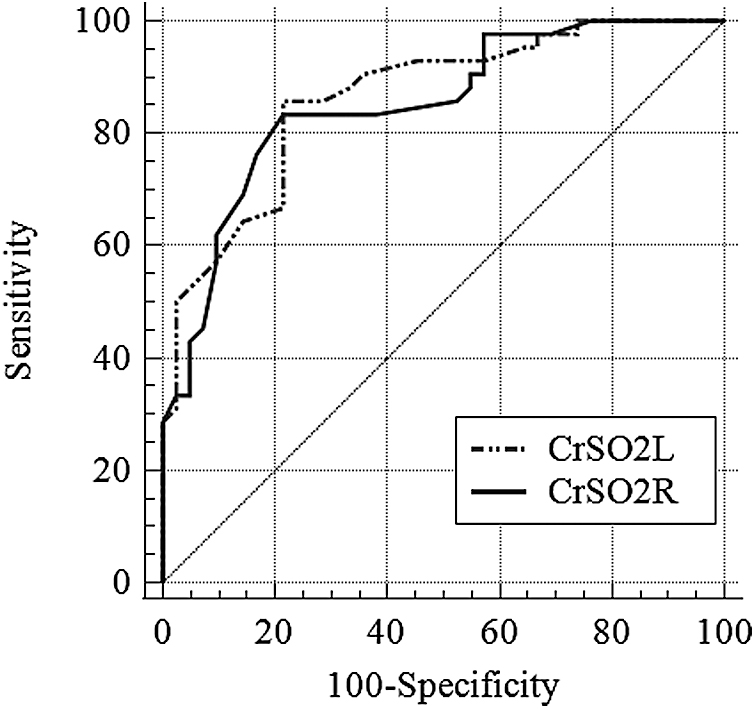
The ROC curve for CrSO2R and CrSO2L. ROC, receiver operating characteristic.
Diagnosis Screening Tests and ROC Curve Results for CrSO2R and CrSO2L Measurements
ROC, receiver operating characteristic.
Discussion
CrSO2 obtained with NIRS is currently widely used to estimate oxygenation in several tissues, primarily the CNS (17–19). In a study by Schat et al. (2019), CrSO2 was measured in preterm infants to evaluate the risk of necrotizing enterocolitis (NEC), and it was reported that low CrSO2 was associated with NEC. In another experimental study of young pigs, Al-Subu et al. (2020) performed NIRS measurements before and after cardiac arrest and demonstrated that there was a significant increase in CrSO2 measurements together with the return of spontaneous circulation. Balcı et al. (2021) observed low CrSO2 measurements during a cardiopulmonary bypass procedure in an adult patient population, and although a rapid increase was seen in CrSO2 following reperfusion, the basal measurement values could not be regained.
In another study by Tsou et al. (2020), there was reported to be a relationship between a fall of >20% in the CrSO2 measurements throughout extracorporeal membrane oxygenation and negative short-term neurological outcomes.
In previous studies of infants with PA, a positive relationship has been reported not with low CrSO2 measurements, but between the severity of trend for elevation of CrSO2 in the first 24–48 hours during TH and negative neurodevelopmental outcomes, and it has been stated that this could be associated with worsening damage or increasing reperfusion (Jain et al., 2017; Peng et al., 2015). Although there are studies in literature related to the use of NIRS during TH, there is no study with sufficient NIRS data in the period of the first 6 hours of life immediately before cooling. In this context, it can be considered that CrSO2 measurements of PA cases in the early period before the application of TH could have a useful role in the diagnosis of PA.
In this study, both the CrSO2L and the CrSO2R measurements were similar and were determined to be statistically significantly lower than those of healthy newborns (p < 0.001). In addition, a cutoff value of CrSO2L ≤ 72% was found to have 85% sensitivity and 78% specificity, while a cutoff value of CrSO2R ≤ 74% had 83% sensitivity and 78% specificity. The paired sample t-test revealed no difference in the CrSO2 measurements obtained from the left and right sides (p = 0.214), and in Pearson correlation analysis, a strong positive correlation was determined (r: 0.81, p < 0.001). These findings suggest that CrSO2 measurements obtained from both the left and right sides could be used as an assistive marker together with blood gas parameters in the diagnosis of asphyxia.
Theoretically, it can be thought that the balance between cerebral oxygen metabolism and cerebral blood flow (CBF) could be estimated with CrSO2. Although several changes can occur in the body with the cerebral autoregulation mechanism, if the CBF is kept stable, this autoregulation mechanism can be affected negatively in pathological hypoxic conditions such as PA (Giesinger et al., 2019; Rodriguez et al., 2020). In a study by Rodriguez et al. (2020), a positive relationship was found between right ventricle output and CrSO2 in infants with PA applied with TH, and it was concluded that reduced right ventricle performance could contribute to the exacerbation of brain damage by changing cerebral perfusion and oxygenation.
In a study of close to term asphytic lambs, Badurdeen et al. (2020) performed measurements related to cerebral oxygen hemodynamics and kinetics immediately after the return of spontaneous circulation following cardiopulmonary resuscitation. The results of that study showed HR and CrSO2 were correlated with oxygen presentation, and CrSO2 was inversely proportional to cerebral fractional oxygen extraction, and could be used as a parameter related to oxygen distribution in the early stage of asphyxia.
In the same study, it was emphasized that CrSO2 was less useful in the determination of oxygen distribution of jugular artery saturation (Badurdeen et al., 2020). Similarly, in this study, although the CrSO2 measurements of asphytic infants immediately before the stage of cooling showed a significant difference from those of healthy infants, no significant difference was determined in the peripheral SpO2 and HR values examined at the same time on pulse oxymetry. Despite the absence of a difference in SpO2 and HR values between the groups, the lower CrSO2 measurements in the PA group suggest that they could affect the changed cerebral oxygen supply and demand secondary to hypoxic damage in the CNS and/or impaired cardiac functions secondary to hypoxic damage.
For the planning of TH treatment, the treatment criteria of pH or BD must be in an appropriate range. pH and BD have been shown to be good markers of survival and discharge from hospital after PA (Burnsed and Zanelli, 2017; Datta, 2017). Umbilical cord acidemia in cord blood gases is currently used as a standardized screening method for the timely diagnosis of PA in newborns (Blecharczyk et al., 2022). The results of this study showed a negative relationship between pH and BD in umbilical cord blood gas analysis in cases with PA. Similarly, a positive relationship was found between pH and both the CrSO2L and CrSO2R measurements of PA cases, but there was no relationship with BD. As the umbilical cord blood gas analysis was only performed in the PA cases, this was thought to have contributed to there being no significant relationship between BD and CrSO2 measurements.
There were some limitations to this study, primarily that umbilical cord blood gas analysis was obtained only from the PA cases and therefore no diagnostic comparison could be made between the blood gas parameters and the NIRS measurements. Therefore, the primary endpoints of the study could not be clearly indicated.
A second limitation was that as the NIRS measurements were performed for the diagnosis of PA, a trend graph could not be obtained related to the NIRS measurements because the measurements were only recorded for 10 minutes. Finally, although the CrSO2 measurements of PA cases in this study were consistently found to be lower than those of healthy infants, the underlying pathology could only be interpreted at an estimated level. There is a need for further more comprehensive studies to take measurements such as echocardiography and aEEG during the CrSO2 measurements in PA cases to be able to contribute to the clarification of the underlying pathophysiology.
In conclusion, the results of this study demonstrated that the early period CrSO2L and CrSO2R measurements in PA cases to be applied with TH were significantly lower than those of healthy newborns with similar characteristics. There was also determined to be a positive relationship between pH and the CrSO2L and CrSO2R measurements. It can be considered that, in addition to cord blood gas analysis, bilateral CrSO2 measurements can be used as a parameter in the diagnosis of PA.
Footnotes
Authors' Contributions
All authors contributed toward data analysis, and drafting and revising the article, and agree to be accountable for all aspects of the work.
Author Disclosure Statement
No financial or nonfinancial benefit has been received or will be received from any party related directly or indirectly to the subject of this article.
Funding Information
There is no funding to report for this study.