
Abstract
Research on the causes of sudden cardiac arrest (CA) after ischemic stroke, especially disruption of the autonomic nervous system's central control, has recently focused more on the widespread cortical and subcortical network than on autonomic circuits at the spinal and brainstem level. However, no clinical case of sudden CA requiring cardiopulmonary resuscitation (CPR) after brainstem infarction has been reported. We report a case of a 78-year-old woman who died suddenly from a brainstem infarction. Her husband heard a falling sound and found her unresponsive and lying with agonal breathing. The initial cardiac rhythm was pulseless electrical activity confirmed by emergency medical technicians. Recovery of spontaneous circulation was achieved after CPR. Basilar artery occlusion was shown on computed tomography, but no other findings that could have caused CA were found. Targeted temperature management was initiated, but she died on hospital day 22. Brainstem infarction may cause sudden CA; therefore, definitive treatment may achieve better outcomes.
Introduction
Cardiac complications associated with stroke are recognized as stroke–heart syndrome (Scheitz et al, 2018). Research on the causes of sudden cardiac arrest (CA) after ischemic stroke, especially disruption of the autonomic nervous system's central control, has recently focused more on the widespread cortical and subcortical network, including the bilateral insular cortex, anterior cingulate gyrus, amygdala, and hypothalamus, than on autonomic circuits at the spinal and brainstem level (Chalkias et al, 2012; Kimmerly et al, 2005; Soros et al, 2012).
Studies on causes of CA during hospital stays in ischemic stroke patients have been reported (Joundi et al, 2016; Prosser et al, 2007), and cases of short-time sinus arrest caused by lateral medulla oblongata infarction were observed (Koay et al, 2013; von Heinemann et al, 2009). However, no clinical case of sudden CA requiring cardiopulmonary resuscitation (CPR) after brainstem infarction has been reported. We report a case of sudden CA after brainstem infarction and discuss the causes of sudden CA after ischemic stroke.
Case Presentation
A 78-year-old woman was transported to our hospital with recovery of spontaneous circulation (ROSC) after CA. Her husband heard a falling sound and found her unresponsive and lying supine with agonal breathing. Bystander CPR was not performed. The initial cardiac rhythm was pulseless electrical activity, confirmed by emergency medical technicians (EMTs). CPR, including chest compression and bag-valve-mask ventilation, was started 9 minutes after CA. ROSC was obtained after two cycles of CPR with two epinephrine injections by the EMTs.
On arrival to the emergency department (ED), her vital signs were as follows: Glasgow Coma Scale score 3, body temperature 36.8°C, blood pressure 184/130 mmHg, pulse rate 104 beats per minute, percutaneous oxygen saturation 100% (fraction of inspiratory oxygen 1.0), and respiration rate 13 times per minute. She was intubated immediately upon arrival. Her medical history was significant for atrial fibrillation with no anticoagulation, and her family medical history was unremarkable. She was spontaneously breathing, both pupil diameters were 3 mm, and showed light reflexes. However, 10 minutes later, both pupil diameters dilated to 6 mm, and light reflexes were not observed bilaterally.
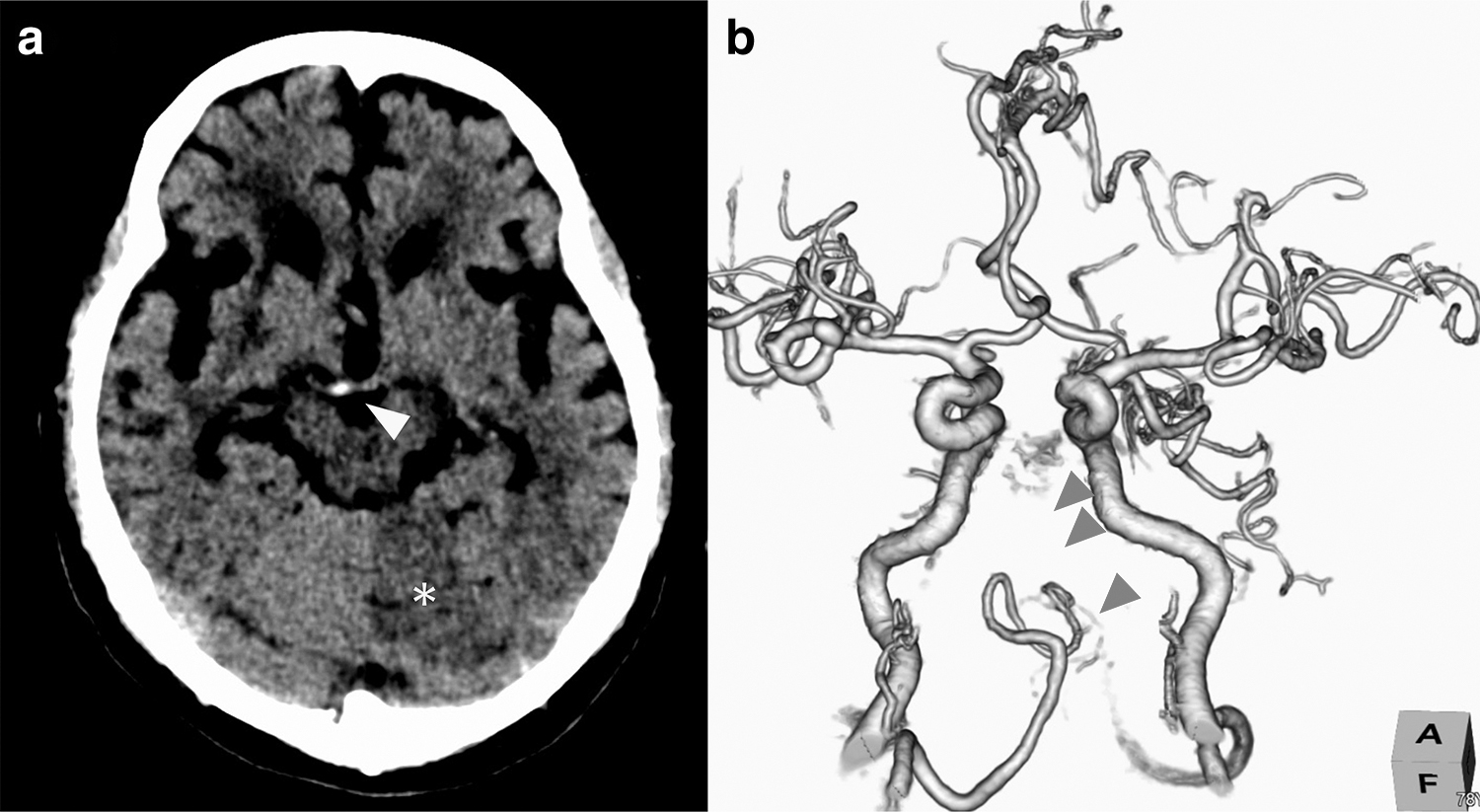
A computed tomography (CT) scan of the head showed a low-density area in the left superior cerebellar arterial region (Fig. 1a), and head CT angiography showed a basilar tip infarction (Fig. 1b). There was no diffuse hypoxic ischemic encephalopathy, pneumothorax, cardiac tamponade, aortic dissection, or pulmonary embolism. Electrocardiography only showed atrial fibrillation with no obvious ST-segment changes. Echocardiography showed prominent left ventricular hypertrophy. There was no evidence of prominent acidosis (pH 7.255), electrolyte imbalance (serum potassium 3.8 mEq/L), hypoglycemia (blood sugar 176.0 mg/dL), hypothermia (body temperature 36.8°C), hypovolemia, or drug use.
The cause of her CA was brainstem infarction. Because of her dilated pupils, her age, time of arrest, and lack of bystander CPR, the neurological prognosis was assumed to be poor. Therefore, endovascular thrombectomy or tissue plasminogen activator (t-PA) injection was not performed. She was admitted to the ICU for targeted temperature management but showed no improvement in her consciousness level. Her family chose best supportive care, and she died on hospital day 22.
Discussion
We reviewed the main causes of CA and eliminated all except acute brainstem infarction. The patient had experienced atrial fibrillation without anticoagulation, ablation, or rate/rhythm control, which may have resulted in the basilar tip infarction caused by a thrombus. Because of the absence of any lung parenchymal abnormalities, normal oxygenation postarrest, and lack of history of any stated preceding dyspnea, it is impossible that CA was preceded by respiratory arrest. Although it is known that respiratory arrest and dysautonomia due to brainstem infarction can cause CA subsequently, it remains unclear why brainstem infarction causes sudden CA.
Theoretically, dysautonomia caused by cerebral infarction is possible. The insular cortex, tractus solitarius nucleus, and ventrolateral medulla, including the nucleus tractus solitarii, comprise the central autonomic network (Benarroch, 1993). The insular cortex mediates high-order autonomic control, and stroke involvement may produce severe cardiac arrhythmias and other autonomic manifestations, resulting in sudden CA (Blech et al, 2018; Krause et al, 2017; Meyer et al, 2004; Scheitz et al, 2018; Wang et al, 2022); however, brainstem infarction may also cause dysautonomia leading to sudden CA by injuring the tractus solitarius nucleus, as shown by a previous case of CA caused by parasympathetic stimulation and of sympathetic inhibition caused by disinhibition of the tractus solitarii nucleus in basilar artery occlusion (von Heinemann et al, 2009).
On the basis of our experience with this significant case, following advanced definitive treatments are considered. If bystander CPR is performed and improved consciousness level seems likely, thrombectomy or t-PA may be considered (Katsanos et al, 2021; Lindsberg et al, 2004; Saver et al, 2016). However, because her neurological prognosis was poor, those treatments were not performed.
There were some limitations in this case. Follow-up CT was not performed because the patient's consciousness level had not improved and her expected neurological prognosis was poor. A left superior cerebellar artery region infarction, shown as a low-density area on the initial CT, was suspected, but the extent was unclear.
Conclusions
When CA is seen in the ED, resuscitation followed by the definitive treatment for specific causes is necessary to improve the prognosis. Brainstem infarction can cause sudden CA, and definitive treatment, including endovascular thrombectomy or t-PA, may achieve better outcomes immediately after ROSC.
Footnotes
Authors' Contributions
Writing—original draft (lead) and writing—review and editing (lead) by T.S. and T.H. Writing—review and editing (supporting) by M.G., S.I., and N.O.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.