
Abstract
In the setting of out-of-hospital cardiac arrest, therapeutic hypothermia (TH) has been shown to improve clinical outcomes. However, trials showing the advantage of TH did not include patients with cardiogenic shock (CS). We performed a comprehensive literature search for studies that evaluated the efficacy and safety of adjunctive TH compared with the standard of care (SOC) in patients with CS. The primary outcome was the mortality rate (in-hospital, short-, and mid-term). The secondary outcomes were the TH-related complications, duration of Intensive Care Unit (ICU) stay, duration of mechanical ventilation (MV-days), and improvement in cardiac function. Relative risk (RR) or the standardized mean difference (SMD) and corresponding 95% confidence intervals (CIs) were calculated using the random-effects model. A total of 7 clinical studies (3 RCTs included), and 712 patients (341 in the TH group and 371 in the SOC group) were included. As compared with the SOC, TH was not associated with a statistically significant improvement in the in-hospital (RR: 0.73%, 95% CI: 0.51–1.03; p = 0.08), short-term (RR: 0.90%, 95% CI: 0.75–1.06; p = 0.21), or mid-term (RR: 0.93%, 95% CI: 0.78–1.10; p = 0.38) mortality rates. Despite the improvement in the cardiac function in the TH group (SMD: 1.08, 95% CI: 0.02–2.1; p = 0.04), the TH strategy did not significantly shorten the MV days, or the ICU stay (p-values >0.05). Finally, there was a trend toward higher risks for infection, major bleeding, and the need for blood transfusion in the TH group. According to our meta-analysis of published clinical studies, TH is not beneficial in patients with CS and has a marginal safety profile. Larger-scale RCTs are needed to further clarify our results.
Introduction
Cardiogenic shock (CS) is defined by end-organ hypoperfusion, hypotension, high pulmonary capillary wedge pressure, and a cardiac index of 2.2 L/min/m2 or less (Van Diepen et al., 2017). Despite advances in CS diagnosis and treatment, in-hospital mortality rates did not change significantly (Jentzer, 2020). The primary cause of diverse end-organ damage and dysfunction in the context of CS is hypoperfusion, which also contributes to the high morbidity and death rates of the illness (Reyentovich et al., 2016).
In addition, CS is thought to have a pro-inflammatory cytokine profile, increased nitric oxide production, and severe vasoplegia, particularly in patients with recent cardiac arrest (Hochman, 2003; Prondzinsky et al., 2012).
Hypothermia reduces oxygen consumption, carbon dioxide production, and glucose utilization by 5% to 7% for every degree of body temperature decline (Soukup et al., 2002). In animal studies, lowering body temperature to 34°C increases the left ventricle's contractility without raising myocardial oxygen consumption (Nishimura et al., 2005). The key to lowering the mortality risk from CS is to rapidly address the imbalance between oxygen supply and demand. However, increasing oxygen delivery in patients who have experienced CS is challenging. Therefore, the clinical approach of induced hypothermia may restore the balance by reducing oxygen consumption (Polderman, 2009).
Therapeutic hypothermia (TH) has undergone substantial research and has been used to treat patients who have experienced cardiac arrest (Safar and Kochanek, 2002), but its clinical effectiveness in CS has not been confirmed. Although the effect of TH in CS patients has been the subject of numerous clinical trials, the findings from these trials have been mixed (Stegman et al., 2012). Further, the clinical investigations on the use of TH in the CS population lacked sufficient power, making it impossible to make clear conclusions about the intervention. Therefore, we conducted this meta-analysis to investigate the efficacy and safety of TH in patients with CS.
Methods
We conducted this systematic review and meta-analysis based on the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (Page et al., 2021). As this research was a systematic review and metanalysis of published data, patient and public involvement were not possible. This study was deemed exempt by the Institutional Review Board of the University of Iowa, as it was a meta-analysis of published studies that included de-identified patient information.
Data sources and search strategy
We performed a comprehensive search for published studies indexed in PubMed/MEDLINE, EMBASE, and Cochrane databases from inception to October 1st, 2022. We also performed a manual search for additional relevant studies using references from the included articles. Supplementary Table S1 describes the full search term used in each database searched.
Eligibility criteria
We included studies that met the following eligibility criteria: (1) peer-reviewed clinical studies, (2) that performed a direct comparison between adjunctive TH to the standard of care (SOC), (3) when used for patients with CS, and (4) reported the outcomes of interest. We excluded conference abstracts, single-arm studies, case reports, case series, animal studies, and observational studies. Two investigators (M.M. and A.A.) independently screened and selected the studies for the final review. Discrepancies were resolved by a third investigator (A.J.).
Data extraction
Extracted data included study design, country and year of the study, follow-up duration, sample size, inclusion and exclusion criteria, efficacy, and safety endpoints. Also, we extracted data for the number of patients who were managed with TH or with SOC only, their age, gender, and baseline comorbidities. We also extracted data on the method of cooling, target temperature, and protocol cooling tome. Finally, we extracted the outcomes of interest. Two investigators (M.M. and W.A.) independently extracted the data from the included studies. Any discrepancies were resolved by consensus.
Outcomes
The primary outcome of our meta-analysis was the mortality rate. We tested the in-hospital mortality, short-term mortality at 30 days, and mid-term mortality at the end of follow-up. We performed a subgroup analysis for the patient whose CS was caused by an acute myocardial infarction (AMI).
Our secondary outcomes included the TH-related complications (infection, major bleeding, need for blood transfusion, tachy- and bradyarrhythmia), duration of Intensive Care Unit (ICU) stay, duration of mechanical ventilation (MV-days), improvement of the cardiac function measured by hemodynamic monitoring, and the acute physiological score improvement.
Statistical analysis
We performed a meta-analysis of the included studies using Review Manager 5.3 (Cochrane Collaboration, Copenhagen, The Nordic Cochrane Centre) and Comprehensive Meta-Analysis (Biostat, Englewood, CO). The median and interquartile range were converted to mean and SD where applicable (Luo et al., 2018). The random-effects model was used to calculate the pooled risk ratio (RR), standardized mean difference (SMD), or mean difference (MD) with the corresponding confidence intervals (CI) for proportional and continuous variables. A p-value <0.05 was considered statistically significant. The heterogeneity was evaluated using the I2 statistic as defined by the Cochrane handbook for systematic reviews. An I2 value of ≥50% was considered significant heterogeneity for all outcomes (Higgins et al., 2003).
Sensitivity analysis
To confirm the robustness of our results, sensitivity analysis for the primary outcomes using a leave-one-out meta-analysis was performed to see if it had a significant influence on the meta-analysis result (i.e., jack-knife sensitivity analysis).
Quality and bias assessment
The Jadad composite scale was used to assess the methodological quality of the clinical trials based on randomization, blinding, and withdrawals (Moher et al., 1998). The scale ranged from 0 to 5 points (Moher et al., 1998). Studies with a total score of ≥3 were considered to have a low risk of bias. Ottawa Quality Assessment Scale (NOS) was used to assess the quality of the non-randomized studies based on the selection of the study groups, comparability of study groups, and ascertainment of exposure/outcome (Stang, 2010).
Studies with total scores of ≥6 were considered to have a low risk of bias. For outcomes reported by ≥5 studies, publication bias was assessed qualitatively by visual inspection of the funnel plot and quantitively by Egger's regression analysis. Two authors (A.B. and M.M.) independently assessed each study for bias. Discrepancies were resolved by a third reviewer (M.S.).
Results
Study selection
A total of 946 studies were retrieved by our search strategy. Among these, 63 were eligible for the systematic review. Seven studies met our inclusion criteria and were included in the meta-analysis (Zobel et al., 2012; Blatt et al., 2015; Orban et al., 2015; Suzuki et al., 2015; Fuernau et al., 2019; Fang et al., 2020; Levy et al., 2022). Figure 1 shows the PRISMA flow chart that illustrates how the final studies were selected.
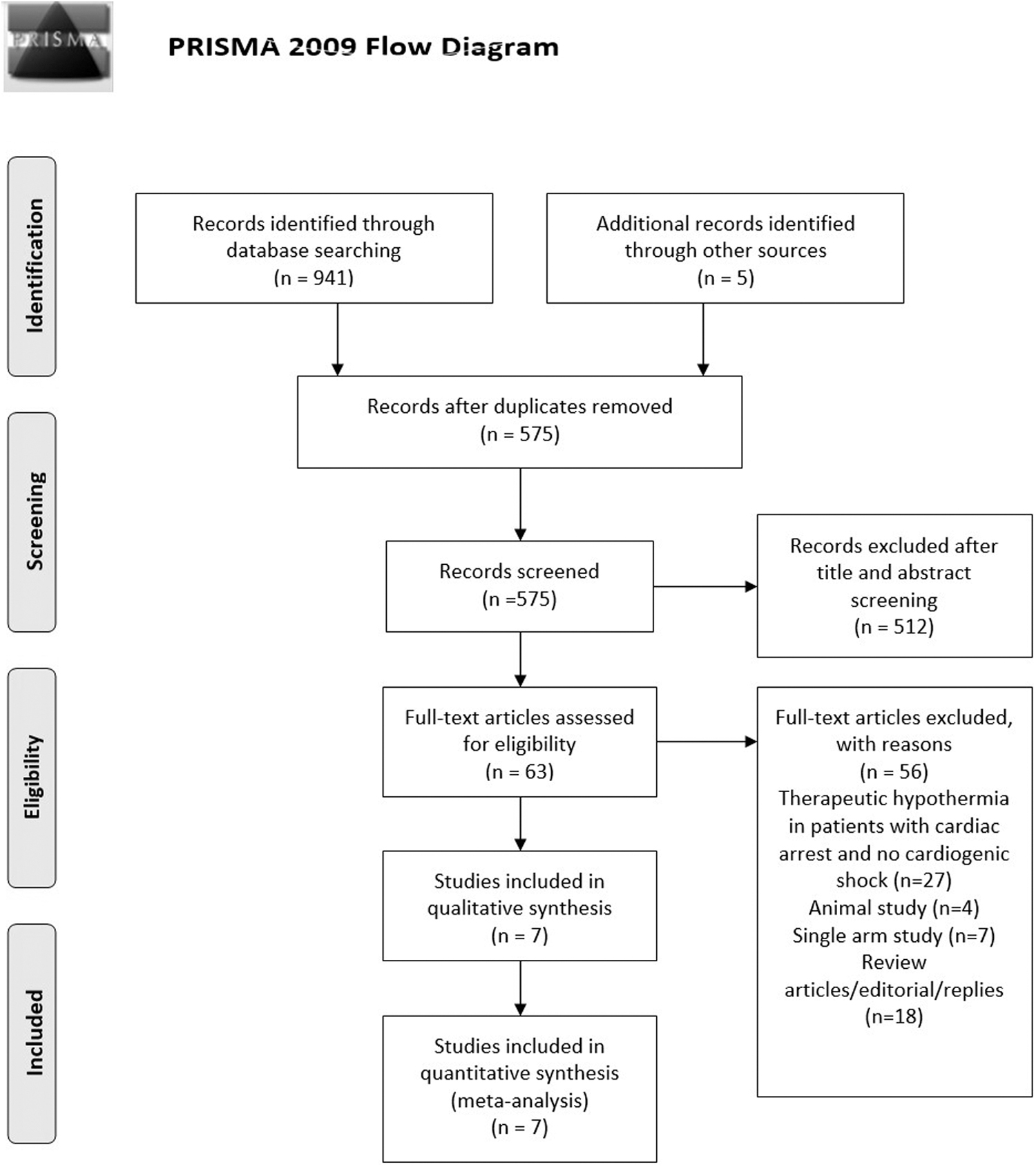
PRISMA flow diagram for the selection of studies.
Study characteristics
Table 1 shows the characteristics of the seven studies included in our meta-analysis. The studies included a total of 712 patients with CS, of whom 341 patients managed with adjunctive TH versus 371 with the SOC only. Regarding the study design, three of the included studies were randomized controlled trials (Orban et al., 2015; Fuernau et al., 2019; Levy et al., 2022), two were matching trials (Zobel et al., 2012; Blatt et al., 2015), one prospective case-control study (Fang et al., 2020), and one prospective cohort study (Suzuki et al., 2015).
Characteristics of Studies Included in the Meta-Analysis
ACS, acute coronary syndrome; CAD, coronary artery disease; CHF, congestive heart failure; CI, cardiac index; CPR, cardiopulmonary resuscitation; CS, cardiogenic shock; EOD, end-organ damage; ESRD, end-stage renal disease; HMD, hemodynamic monitoring; ICM, ischemic cardiomyopathy; ICU, intensive care unit; MI, myocardial infarction; MV, mechanical ventilation; NR, not reported; PC, pulmonary congestion; RCT, randomized control trial; SBP, systolic blood pressure; SOC, standard of care; STEMI, ST-elevation myocardial infarction; TH, therapeutic hypothermia; UoP, urine output; VA-ECMO, veno-arterial extracorporeal membrane oxygenation; VHD, valvular heart disease.
The etiology of CS varied among the studies that were included; 4 studies had patients with AMI (Blatt et al., 2015; Orban et al., 2015; Fuernau et al., 2019), one study had elective valve replacement surgery complicated with CS (Fang et al., 2020), one study had CS seen in patients who had experienced out-of-hospital cardiac arrest (Zobel et al., 2012), and the last study had a variety of etiologies with 36% of cases with AMI (Levy et al., 2022).
Regarding the hypothermia protocol, two studies used endovascular catheter cooling (Zobel et al., 2012; Blatt et al., 2015), one study used continuous blood purification cooling (Fang et al., 2020), one study used the Thermogard XP temperature management system (Fuernau et al., 2019), one study used a VA-ECMO circuit temperature controller (Levy et al., 2022), one study used surface cooling (Orban et al., 2015), and the final study used a combination of endovascular and surface cooling (Suzuki et al., 2015). TH time protocol ranged from 12 to 24 hours, the target body temperature varied between 32°C and 34°C, and the follow-up time varied between 3 days and 3 years.
Table 2 summarizes the baseline comorbidities for the included patients. In terms of age, gender, and other risk factors for cardiovascular disease, the TH group and the control group were comparable. The mean age was 60.6 ± 17 years, men represented 72% of the total patients, 29.1% were smokers, 53% had hypertension, 51.8% had hyperlipidemia, 35.7% had diabetes mellitus, and 22.4% had a prior myocardial infarction.
Baseline Patients and Procedural Characteristics Included in the Meta-Analysis
NS, not significant.
Outcomes of interest
In-hospital mortality
Six studies with 696 patients reported in-hospital mortality (average of 5 days); the in-hospital mortality rate did not differ significantly between the two groups (RR: 0.73%, 95% CI: 0.51–1.03; p = 0.08). No significant heterogeneity was observed (I2 = 20%, P heterogeneity = 0.28) Figure 2A. The subgroup analysis among patients with AMI showed no statistically significant difference in the in-hospital mortality rate between the TH and SOC groups (RR: 1.13%, 95% CI: 0.69–1.83; p = 0.63) Supplementary Figure S1.
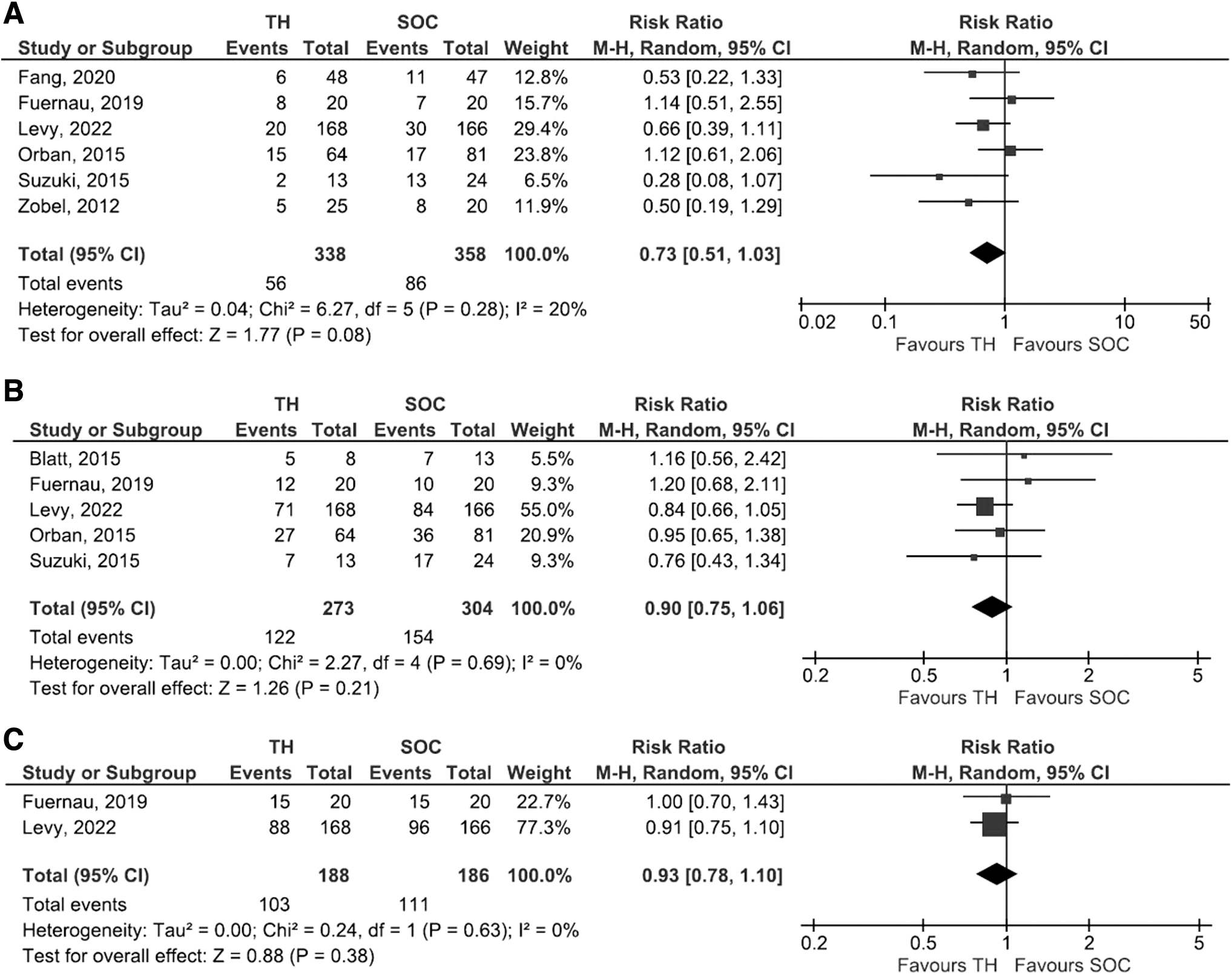
Forest plot comparing adjunctive therapeutic hypothermia and standard of care regarding
Short-term mortality
Five studies with 575 patients reported short-term mortality (at 30 days); the short-term mortality rate did not differ significantly between the two groups (RR: 0.90%, 95% CI: 0.75–1.06; p = 0.21). No significant heterogeneity was observed (I2 = 0%, P heterogeneity = 0.69) Figure 2B. The subgroup analysis among patients with AMI showed no statistically significant difference in the short-term mortality rate between the TH and SOC groups (RR: 1.04%, 95% CI: 0.78–1.39; p = 0.79) Supplementary Figure S2.
Mid-term mortality
Two studies with 374 patients reported mid-term mortality (average 2.5 years); the mid-term mortality rate did not differ significantly between the two groups (RR: 0.93%, 95% CI: 0.78–1.10; p = 0.38). No significant heterogeneity was observed (I2 = 0%, P heterogeneity = 0.63) Figure 2C.
Infection
There were 207 events of infection reported in four studies (113 vs. 94 events in the TH and control group respectively). The TH group had a numerically increased infection risk, but there was no statistically significant difference (RR: 1.20, 95% CI: 0.97–1.47; p = 0.09, I2 = 0%) as depicted in Figure 3A.

Forest plot comparing adjunctive therapeutic hypothermia and standard of care regarding
Major bleeding or need for blood transfusion
There were 189 events of major bleeding or need for blood transfusion reported in four studies (98 vs. 91 events in the TH and control group respectively). The TH group had a numerically higher bleeding risk, but there was no statistically significant difference (RR: 1.20, 95% CI: 0.85–1.69; p = 0.29, I2 = 27%) as depicted in Figure 3B.
Arrhythmia
There were 38 arrhythmia events reported in two studies (17 vs. 21 events in the TH and control group respectively). The SOC group had a numerically higher arrhythmia risk, but there was no statistically significant difference. (RR: 0.87, 95% CI: 0.52–1.44; p = 0.58, I2 = 0%) as depicted in Figure 3C.
MV days
This outcome was documented in three studies; MV days were statistically similar between the two groups (MD: 0.03, 95% CI: −4.26 to 4.32; p = 0.99) as depicted in Figure 4A

Forest plot comparing adjunctive therapeutic hypothermia and standard of care regarding
Significant heterogeneity was observed (I2 = 93%, P heterogeneity<0.01), yet a leave-one-out sensitivity analysis showed no heterogeneity after removing the Fang et al. (2020), study with the results being statistically significant favoring the SOC group (MD: 2.09, 95% CI: 0.31–3.87; p = 0.02, I2 = 0%), as shown in Supplementary Figure S3.
ICU-stay
This outcome was documented in three studies; ICU stay was statistically similar between the two groups (MD: −1.91, 95% CI: −7.07 to 3.24; p = 0.47), as depicted in Figure 4B
Significant heterogeneity was observed (I2 = 81%, P heterogeneity<0.01), yet a leave-one-out sensitivity analysis showed no heterogeneity after removing the Fang et al. (2020) study, with the results being consistent, as shown in Supplementary Figure S4.
Cardiac function improvement
Two studies reported the change in the cardiac function measured by invasive hemodynamic monitoring (cardiac index or cardiac power) between the two groups. The TH group had a statistically significant improvement in cardiac function by the end of the ICU stay (SMD: 1.08, 95% CI: 0.02–2.1; p = 0.04), as seen in Supplementary Figure S5.
Acute physiological score
Two studies reported the change in the acute physiological score between the two groups, with no statistically significant difference between the two groups (SMD: −2.05, 95% CI: −6.03 to 1.92; p = 0.31) as depicted in Supplementary Figure S6.
Quality and bias assessment
Quality assessment scores of the included studies are summarized in Supplementary Table S2. All studies scored low to moderate in quality assessment. The funnel plots for the in-hospital and short-term mortality appeared asymmetric by visual inspection (Supplementary Figs. S7 and S8). However, Egger's regression analysis did not show evidence of publication bias (p = 0.18, p = 0.33 respectively).
Discussion
This study was a systematic review and meta-analysis of all investigations that evaluated the efficacy and safety of adjunctive TH in patients with CS in comparison to the SOC. According to our results, using TH had no discernible impact on in-hospital, short-term, or mid-term survival. Adjunctive hypothermia did not significantly reduce the number of days spent on MV or the length of stay in the ICU, despite the increase in cardiac function shown in the TH group. Finally, there was a tendency in the TH group toward greater risks for infection, significant bleeding, and the need for blood transfusion.
In animal studies, moderate hypothermia in CS resulted in maintained or augmented inotropy, reduced oxygen consumption, and improved survival (Götberg et al., 2010). The theoretical advantages, however, have not been successfully translated into significant clinical outcomes in a number of human studies (Fuernau et al., 2019). These studies' size limitations and emphasis on hemodynamic changes were additional drawbacks.
Our findings suggest the lack of clinical benefits of TH in patients with CS, as it failed to improve survival, in contrast to the evidence of TH in cardiac arrest patients (Safar and Kochanek, 2002). AMI is the leading cause of CS, accounting for about 80% of cases, and CS remains the most common cause of mortality among patients hospitalized for myocardial infarction (Thiele et al., 2015). TH has been proposed as an adjunctive therapy for the treatment of AMI, and animal studies have shown that the use of TH in the acute setting may reduce infarct size (Stegman et al., 2012).
However, previous metanalyses (Alushi et al., 2021; Mhanna et al., 2022) investigated the use of TH in patients with AMI treated with percutaneous coronary intervention, and, at the cohort level, their results did not show a significant difference in all-cause mortality or infarct size in those treated with TH vs SOC. These findings share a similar sentiment with our subgroup analysis, which shows no mortality benefit in patients treated with TH for myocardial infarction-related CS compared with the SOC.
Previous retrospective data have demonstrated favorable hemodynamic changes in patients with CS after initiating TH (Stegman et al., 2015). This is consistent with our findings; however, although our results are statistically significant, the clinical utility of such a benefit needs to be considered against the questionable mortality benefit based on our data.
TH is not without risks; physiological changes brought on by hypothermia in the circulatory, homeostatic, and metabolic systems may negatively affect therapeutic outcomes. Hypothermia has been shown to affect platelet count and function as well as the synthesis and kinetics of the clotting cascade (Polderman, 2009). In the non-surgical setting, however, these effects have not previously been shown to pose a significantly increased risk of bleeding (Schefold et al., 2009; Kander and Schott, 2019; Mecklenburg et al., 2021).
Our results, though showing a tendency toward bleeding events and the need for blood transfusion, were not statistically significant. Whether this tendency is clinically significant in the setting of CS warrants further investigation. The immunosuppressive effects of TH have been previously discussed in the literature, and the theoretical risk for infection due to TH is widely accepted (Polderman, 2009). However, the literature is mixed regarding whether TH actually increases the risk for infection in the clinical setting (Geurts et al., 2014; Kim et al., 2020). Our results are similarly inconclusive, showing a tendency toward infection but were not statistically significant.
To our knowledge, this is the first systematic review and meta-analysis of the existing literature on TH for CS. This is of particular interest because, despite TH being a common practice for patients following cardiac arrest, most of the relevant trials studying TH for cardiac arrest have excluded patients with CS (Thiele et al., 2015). Moreover, there are other etiologies of CS for which TH has been studied but conclusions have been weak or mixed.
Our results suggest that TH may improve cardiac function based on hemodynamic measurements but does not appear to produce a mortality benefit and could potentially pose an increased risk of bleeding and infection. In a patient population that is already hypotensive and severely ill due to cardiac insult, the risks of such an intervention should be weighed against the potentially marginal clinical benefits.
There are certain limitations to our meta-analysis. First, despite pooling the data from all the available literature, the overall sample size was small with a low rate of events which might explain the overall neutral effect. Second, patient-level data was lacking which prevented us from adjusting our results to several variables. Third, although analysis using a random-effect model was performed, significant heterogeneity was found in some of the study's outcomes. Fourth, the hypothermia protocol was not standardized among the included studies. Finally, the etiology behind the CS varies among the included studies, which could explain the observed heterogeneity in some of the outcomes.
Our meta-analysis, on the other hand, has significant advantages. To begin, we used strict inclusion criteria and only included fully published clinical studies. Second, we investigated the effectiveness of TH in terms of mortality, hypothermia-related complications, and ICU stay. Third, our meta-analysis is the first to show that adjunctive hypothermia in CS could potentially increase the risk of infection and bleeding complications. Finally, we looked at CS patients with myocardial infarction as a subgroup with the results being consistent.
In conclusion, our meta-analysis demonstrated no benefit of TH in CS patients, with a marginal safety profile. Large-scale RCTs are needed to verify our results.
Footnotes
Authors' Contribution
M.M. and A.A. conceived and designed the study, drafted the manuscript, and critically revised the manuscript. M.M., A.J., and W.A. designed the study, and collected, analyzed, and interpreted the data. M.C.S., M.S., A.B., and S.M. collected the data and reviewed the literature. All authors read and approved the final manuscript.
Author Disclosure Statement
The authors declared no conflict of interest.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.