
Abstract
This study investigates the clinical profile and predictors of gastrointestinal/hepatic morbidities and feeding outcomes among neonates with hypoxic–ischemic encephalopathy (HIE). A single-center retrospective chart review of consecutive neonates >35 weeks of gestation admitted with a diagnosis of HIE between January 1, 2015, and December 31, 2020, and treated with therapeutic hypothermia, if met the institutional eligibility criteria. Outcomes assessed included necrotizing enterocolitis (NEC), conjugated hyperbilirubinemia, hepatic dysfunction, assisted feeding at discharge, and time to reach full enteral and oral feeds. Among 240 eligible neonates (gestational age 38.7 [1.7] weeks, birth weight 3279 [551] g), 148 (62%) received hypothermia therapy, and 7 (3%) and 5 (2%) were diagnosed with stage 1 NEC and stage 2–3 NEC, respectively. Twenty-nine (12%) were discharged home with a gastrostomy/gavage tube, conjugated hyperbilirubinemia (first week 22 [9%], at discharge 19 [8%]), and hepatic dysfunction (74 [31%]). Time to reach full oral feeds was significantly longer in hypothermic neonates compared with neonates who did not receive hypothermia (9 [7–12] days vs. 4.5 [3–9] days, p < 0.0001). Factors significantly associated with NEC were renal failure (odds ratio [OR] 9.24, 95% confidence interval [CI] 2.7–33), hepatic dysfunction (OR 5.69, 95% CI 1.6–26), and thrombocytopenia (OR 3.6, 95% CI 1.1–12), but no significant association with hypothermia, severity of brain injury, or stage of encephalopathy. Transient conjugated hyperbilirubinemia, hepatic dysfunction within first week of life, and need for assistive feeding are more common than NEC in HIE. Risk of NEC was associated with the severity of end-organ dysfunction in the first week of life, rather than severity of brain injury and hypothermia therapy per se.
Introduction
Hypoxic–
Secondly, perinatal asphyxia results in impaired pharyngo-esophageal protective reflexes, and thus, neonates often require gastrostomy tube or gavage feeds at discharge (Jensen et al., 2017). Lastly, delayed initiation and slow progression in enteral feeds during therapeutic hypothermia contribute to prolonged parenteral nutrition. This often contributes to increased risk of central line-related complications and aggravate ischemia-induced transient hepatic dysfunction and cholestasis (Zingg et al., 2012; Jolin-Dahel et al., 2013).
The practice of withholding enteral feeds during therapeutic hypothermia has been recently questioned. It is speculated that a combination of impaired gastrointestinal perfusion and proinflammatory response to intraluminal substrate may predispose to gut necrosis and NEC (Schnabl et al., 2008). The landmark cooling trials withheld feeds during hypothermia and delayed the introduction of enteral feeds to prevent NEC. Among 11 trials, only 3 trials reported data on NEC and that varied from 0% to 4% (Azzopardi et al., 2009; Jacobs et al., 2011). Recent observational studies reported the incidence of NEC as 0–1% using pragmatic definitions (Thyagarajan et al., 2015; Gale et al., 2021; Alburaki et al., 2022).
The introduction of enteral feeds during therapeutic hypothermia has been associated with shorter time to reach full enteral feeds (Thornton et al., 2014), lower inflammatory cytokine concentrations, fewer days of parenteral nutrition and hospital stay (Chang et al., 2018), with no difference in NEC (Thyagarajan et al., 2015). It essential to know the true risk of NEC as opposed to other gastrointestinal morbidities in neonates receiving therapeutic hypothermia for deciding the risks versus benefits of early enteral nutrition in this cohort.
There is also significant variability in the reported prevalence of other gastrointestinal morbidities in neonates with HIE. The Cool Cap study reported lower incidence of elevated liver enzymes in cooled subjects (38%) versus controls (53%) (Jacobs, 2005).
The ICE study reported lower rates of hepatic dysfunction among cooled subjects (35%) versus controls (45%), but a higher incidence of rectal bleeding and NEC in 4% of cooled subjects versus 2% of controls (Jacobs et al., 2011). On the contrary, Zhou et al. (2010) reported raised liver enzymes in 35% of the cooled subjects versus 28% of the controls. The NICHD trial reported hepatic dysfunction in 20% of cooled subjects versus 15% of controls. In the cooled group, 11% were discharged on gavage feeds (vs. 7% of controls) and 7% discharged with a gastrostomy tube (vs. 17% of controls) (Shankaran et al., 2005). Although hepatic dysfunction and feeding disturbances are well recognized, none of these trials focused specifically on the effects to the gastrointestinal system and the results are conflicting.
This study aimed to describe the gastrointestinal morbidity profile and feeding outcomes of neonates who are admitted with a diagnosis of HIE in a center offering therapeutic hypothermia according to internationally accepted eligibility criteria and withholding feeds during therapy. Furthermore, we aimed to identify potential risk factors that are associated with an increased risk of NEC, the most fatal among the known gastrointestinal morbidities.
Materials and Methods
Study design
We conducted a retrospective cohort study of neonates admitted to McMaster Children's Hospital tertiary care neonatal intensive care unit (NICU) with HIE between January 1, 2015, and December 31, 2020. The study was approved by the institutional research ethics board. Clinical data were retrieved from electronic medical records. We took a convenience sample of all consecutive eligible infants admitted to the center within the stipulated time period.
Study population
We included consecutive inborn and outborn neonates ≥35 weeks of gestation with the diagnosis of HIE. HIE was defined as the presence of either of the following criteria (A) evidence of an acute sentinel event such as fetal distress, cord prolapse, uterine rupture, reduced fetal movements, abruption, antepartum hemorrhage, or emergency cesarean section due to fetal distress; and/or (B) evidence of intrapartum hypoxia (at least one of: Apgar score of ≤5 at 10 minutes, mechanical ventilation or resuscitation within 10 minutes, cord pH <7.00 [venous or arterial], or an infant arterial pH <7.00 or base deficit ≥12 within 60 minutes of birth), along with any stage of encephalopathy. Encephalopathy was graded according to Sarnat staging at the time of admission into stage 1 (Mild), stage 2 (Moderate), and stage 3 (Severe) (Sarnat and Sarnat, 1976).
Stage of HIE was identified by the final assigned diagnosis entered in the electronic screening of admission notes. Neonates with cyanotic congenital heart disease, congenital brain anomalies/brain stem abnormalities, congenital anatomical airway issues, for example, Pierre Robin sequence, cleft-lip and palate, tracheoesophageal fistula, and biliary atresia were excluded from the study. The decision to initiate therapeutic hypothermia was taken by the attending neonatologist based on unit-specific therapeutic hypothermia policy adapted from the Canadian Pediatric Society position statement (Lemyre and Chau, 2018).
Outcome and clinical predictors
We reported all gastrointestinal and hepatic morbidities including (1) NEC (stage 2–3); (2) conjugated hyperbilirubinemia within first 7 days of life (DOL) and at discharge; and (3) hepatic dysfunction. We also reported feeding outcomes including (1) home discharge with gavage or gastrostomy tube feeds; (2) length of stay in level III NICU; (3) time to reach full enteral feeds; (4) time to reach full oral feeds; and (5) gastroesophageal reflux needing medications. NEC was defined by intestinal and radiographic signs of modified Bell's staging criteria (Bell et al., 1978). Conjugated hyperbilirubinemia was defined as direct bilirubin level >20% of the total bilirubin or >20 μmol/L within DOL 7 and at discharge. Hepatic dysfunction was defined as alanine transaminase (ALT) >100 IU/L or aspartate transaminase (AST) >100 IU/L within DOL 7 (Yan et al., 2022).
We retrieved patient-specific clinical predictors of NEC including (1) perinatal factors: birth weight, Apgar score at 5 and 10 minutes, cord blood or postnatal pH, gestational age, maternal characteristics and (2) neonatal factors: the presence or absence of clinical or electrical seizures within first 72 hours, multiorgan dysfunction, culture-proven sepsis, laboratory parameters in the first 72 hours, and severity of brain injury on magnetic resonance imaging (MRI). Brain injury was categorized as normal MRI and abnormal MRI. The latter group was further classified as watershed pattern of injury, basal ganglia pattern of injury, and presence of intra/extracranial hemorrhage.
Among multiorgan dysfunction, persistent pulmonary hypertension (PPHN) was defined by either echocardiographic evidence or inhaled nitric oxide therapy; renal failure was defined as urine output <0.5 mL/(kg·h) OR rising creatinine >100 mmol/L at any time within the first 72 hours; coagulopathy was defined as international normalized ratio (INR) >1.5 in the first 72 hours of life; and cardiac dysfunction defined as the need for inotrope to support blood pressure or echocardiographic evidence of cardiac dysfunction.
Statistical analysis
Descriptive statistics were used for the baseline characteristics and incidence of clinical outcomes. We reported the baseline characteristics of neonates who received therapeutic hypothermia compared with those who either did not receive therapeutic hypothermia or were started on and discontinued within 24 hours of life. Clinical characteristics were compared between the two groups using chi-squared test for categorical variables and one-way ANOVA for continuous variables. To identify the early clinical and laboratory predictors of NEC, the univariate logistic regression model was used and reported odds ratio (OR) with 95% confidence interval (CI). A p-value of <0.05 was considered significant. Given the low number of clinical outcomes of interest (NEC), multivariate regression analysis was not possible.
Results
There were 241 eligible neonates admitted during the study period and 1 neonate was excluded due to congenital airway anomalies and need for assistive feeding to ensure upper airway safety. The mean (standard deviation) gestational age and birth weight of the entire cohort was 38.7 (1.7) weeks and 3279 (551) g, respectively. The proportion of neonates who did not receive therapeutic hypothermia, who were initiated on hypothermia but discontinued before 24 hours of life, and who completed 72 hours of hypothermia protocol was 42 (16%), 50 (20%), and 148 (62%) respectively.
Perinatal characteristics of the study population
There was no significant difference in the maternal demographics, gestational age, birth weight, and sex distribution between neonates who received and did not receive a complete therapeutic hypothermia protocol (Table 1). There was no statistically significant difference between the groups in the incidence of seizures, PPHN, renal failure, coagulopathy, cardiac dysfunction, and culture-proven sepsis (Table 1). The proportion of neonates with abnormal brain MRI was lower in neonates who received complete therapeutic hypothermia protocol. The hypothermia group was more likely to receive sedation during the first week of life.
Maternal and Neonatal Characteristics of the Study Population
Hepatic dysfunction was defined as ALT >100 IU/L or AST >200 IU/L. PPHN was defined by either echocardiographic evidence or inhaled nitric oxide therapy; renal failure was defined as urine output <0.5 mL/(kg·h) OR rising creatinine >100 mmol/L at any time within first 72 hours; coagulopathy was defined as INR >1.5 in the first 72 hours of life; cardiac dysfunction defined as the need for inotrope to support BP or echocardiographic evidence of cardiac dysfunction; seizures included clinical and/or electro graphic seizures. Sedation included morphine/fentanyl/dexmedetomidine/midazolam infusions.
Mean ± SD, one-way ANOVA (continuous variable).
n (%) chi-square test (categorical variable).
ALT, alanine transaminase; AST, aspartate transaminase; BP, blood pressure; DOL, days of life; INR, international normalized ratio; IQR, interquartile range; MRI, magnetic resonance imaging; PPHN, persistent pulmonary hypertension; SD, standard deviation.
Outcomes
NEC was diagnosed in 12 (5%) infants, which included stage 1 (7 neonates) and stage 2–3 (5 neonates). Among them, all 5 neonates with stage 2–3 NEC needed laparotomy. Twenty-nine (12%) neonates were discharged home with either gastrostomy or gavage tube. Conjugated hyperbilirubinemia was noted in 22 (9%) neonates within DOL 7 and 19 (8%) neonates at discharge. Within the first week of life, 74 (31%) of neonates had hepatic dysfunction. Only 3 (1.2%) neonates had gastro-esophageal reflux treated with medications. Figure 1 illustrates the incidence rate of gastrointestinal/hepatic morbidities and abnormal feeding outcomes in the neonates who received and did not receive complete therapeutic hypothermia protocol. Neonates who did not receive hypothermia were started on enteral feeds earlier and reached full enteral and full oral feeds in shorter time compared with neonates who received hypothermia either for <24 or for 72 hours (Table 2).
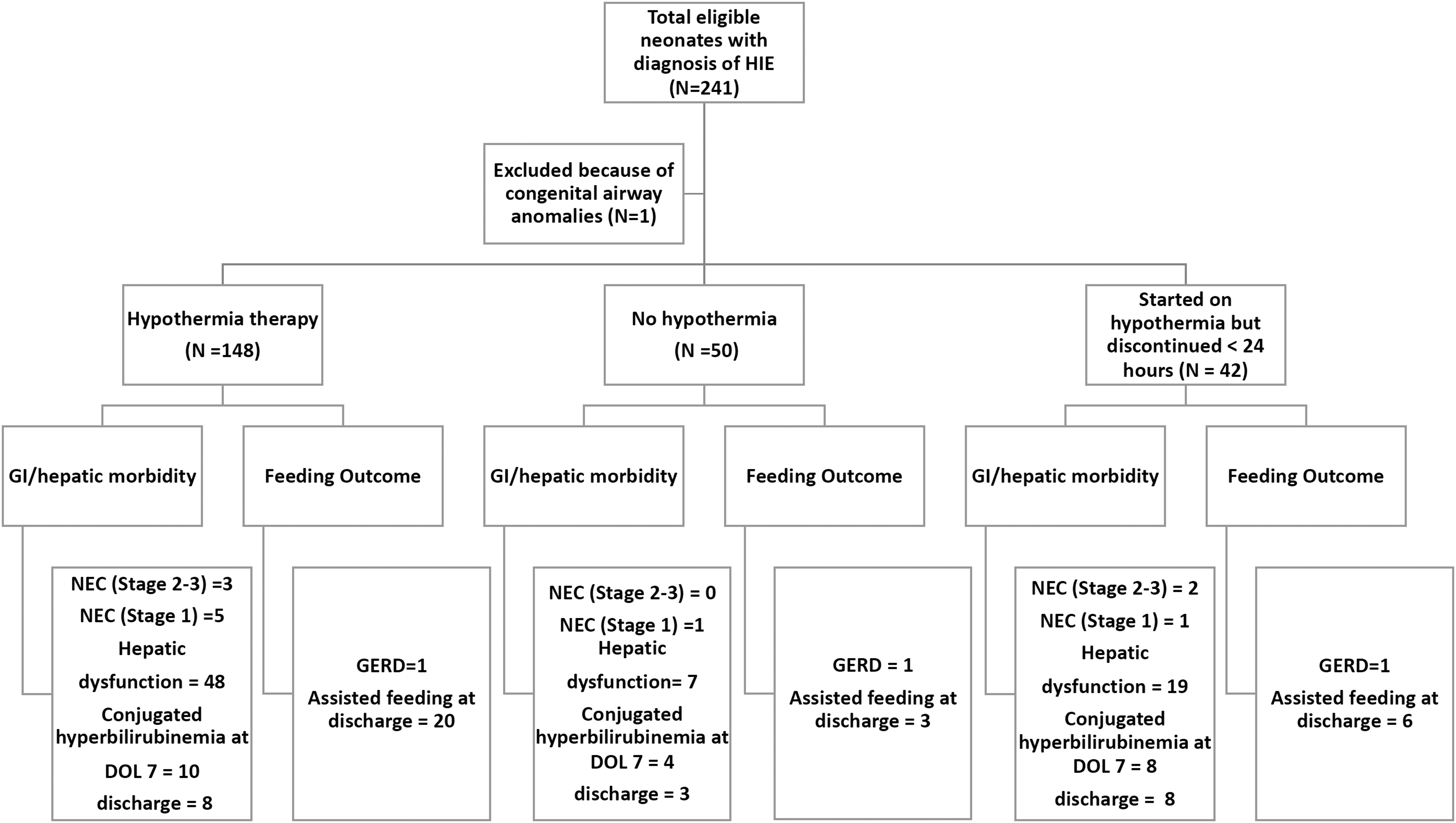
Flowchart of infants enrolled in the study and incidence of gastrointestinal and hepatic morbidities. DOL, Days of life; GERD, Gastroesopheal reflux disease; GI, Gastrointestinal; NEC, Necrotizing Enterocolitis.
Distribution of Clinical Outcomes Among the Study Population
Kruskal–Wallis test (continuous variable), chi-square test (categorical variable).
DOL, days of life; GI, gastrointestinal; IQR, interquartile range; SD, standard deviation.
There was not statistically significant difference between the three groups in the incidence of NEC, conjugated hyperbilirubinemia, hepatic dysfunction, gastroesophageal reflux requiring antireflux medications at discharge, and the need for assistive feeding at home (Table 2). Mortality rate in the total cohort was 10 (4%), among them 8 (5%) patients died in the hypothermia group.
Laboratory parameters
Figure 2 depicts the various biochemical changes in the first week of life in the cohort of patients. There was no statistically significant difference in most biochemical markers between the three groups, except for AST levels and sodium levels in the first week of life. The neonates who received thereapeutic hypothermia for any duration demonstrated higher AST levels [median (interquartile range, IQR) hypothermia >24 hours 119 (69–236) IU and hypothermia <24 hours 154 (78–374) IU] than neonates who did not receive in hypothermia [99 (85–165) IU]. Also the neonates exposed to hypothermia tend to lower sodium levels in the first week of life [median (IQR) hypothermia >24 hours 131 (128–133) mmol/L] compared with neoantes who received hypothermia <24 hours 133 (129–135) mmol/L and not exposed to hypothermia [134 (130–138) mmol/L].
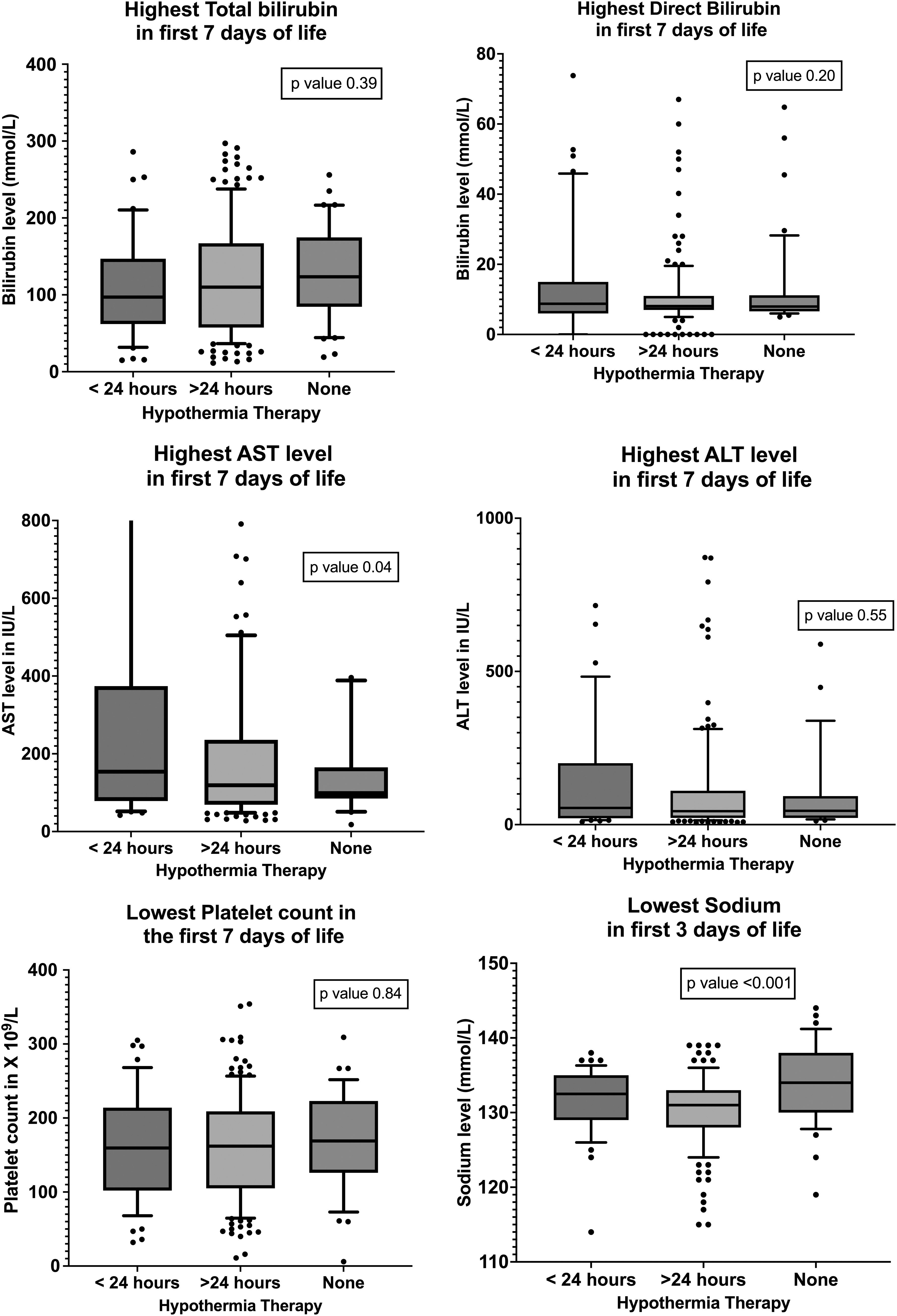
Comparing the commonly encountered serum biochemical and hematological alterations in neonates with hypoxic–ischemic encephalopathy with or without hypothermia therapy.
Clinical predictors of NEC
On univariate logistic regression, the clinical risk factors that significantly increased the risk of NEC were renal failure (OR 9.24, 95% CI 2.7–33), coagulopathy (OR 4.87, 95% CI 1.5–19), thrombocytopenia (lowest platelet count <100 × 109/L within DOL 3) (OR 3.63, 95% CI 1.1–12), and hepatic dysfunction in the first week of life (OR 5.69, 95% CI 1.6–26) (Table 3). There was no association between brain injury, severity of HIE, or hypothermia therapy, and the risk of NEC.
Clinical and Laboratory Predictors of Necrotizing Enterocolitis
Renal failure was defined as urine output <0.5 mL/(kg·h) or rising creatinine >100 mmol/L at anytime within the first 72 hours. Thrombocytopenia was defined as platelet count <100 × 109/L at any time within the first 72 hours. Hepatic dysfunction was defined as AST level >200 IU/L and/or ALT level >100 IU/L at any time within the first 7 DOL. Coagulopathy was defined as INR >1.5 at any time within first 7 DOL.
Log transformed.
ALT, alanine transaminase; AST, aspartate transaminase; CI, confidence interval; DOL, days of life; INR, international normalized ratio; MRI, magnetic resonance imaging, OR, odds ratio.
Clinical predictors of feeding outcomes
On univariate linear regression, the clinical risk factors that had significant effect on the time needed for reaching full enteral feeds were (1) PPHN (β = 7.1, 95% CI 2.9–11.3, p = 0.001); (2) culture-positive sepsis (β = 13.8, 95% CI 6.4–11.3, p = 0.003); and (3) basal ganglia injury (β = 9.1, 95% CI 4.6–13.5, p < 0.0001). The clinical risk factors that had significant effect on the time needed to reach full oral feeds were (1) PPHN (β = 6.8, 95% CI 2.2–11.5, p = 0.004) and (2) basal ganglia injury (β = 12.6, 95% CI 7.9–17.6, p < 0.0001).
Discussion/Conclusion
This study delineates a range of gastrointestinal and hepatic comorbidities along with feeding outcomes of neonates with HIE. Two-thirds of our cohort met the eligibility criteria and received therapeutic hypothermia. As per unit policy, enteral feeds were started only after rewarming. The commonest gastrointestinal complications that emerged from the present study included transient hepatic dysfunction defined by elevated liver enzymes in the first week of life. Other less frequent complications were transient conjugated hyperbilirubinemia in the first week of life, which may occasionally be persistent at discharge. One-tenth of neonates needed assistive feeding at discharge, indicating delayed development of oral–motor coordination.
NEC and gastro-esophageal reflux needing pharmacological treatment were the least common complications. Neonates who received therapeutic hypothermia either for the full 72 hours or were started but had to be discontinued before 24 hours tend to need longer time to achieve full oral feeds and therefore a longer stay in hospital.
Based on the hypothermia trials (Jacobs et al., 2013), it has been a common practice to keep neonates nil-per-mouth during hypothermia therapy to prevent additional stress on the intestines after a recent ischemic insult. This was based on the physiological principles that induced hypothermia causes splanchnic vasoconstriction (Ohri et al., 1997; Powell et al., 1999), platelet aggregation (Straub et al., 2005), impaired bowel function, and delayed gastric emptying (Polderman, 2009) and may increase the risk of NEC.
This possibility has been refuted in some recent observational studies that suggest that the baseline rate of NEC in this population is low, and therefore, early enteral feeds may indeed have some benefit in reducing the length of hospital stay (Thyagarajan et al., 2015; Chang et al., 2018; Gale et al., 2021), earlier establishment of full oral and enteral feeds (Thyagarajan et al., 2015; Chang et al., 2018), shorter periods of parenteral nutrition (Chang et al., 2018), higher rates of breastfeeding (Thyagarajan et al., 2015; Gale et al., 2021), and lower rates of late-onset infections (Gale et al., 2021). Importantly, early enteral feeds did not increase the incidence of NEC (Thyagarajan et al., 2015; Alburaki et al., 2022).
Similar benefits have been seen with early introduction of milk feeds in preterm infants, mediated by multiple mechanistic pathways such as preventing of villous atrophy, decreasing intestinal permeability, favorably influencing intestinal microbiome, reducing risk of systemic inflammation, and promoting neurologic and physiologic gut motility (Thornton et al., 2014). Our findings further support to refute the notion that therapeutic hypothermia increases the risk of NEC by demonstrating that the NEC (stage 2–3) is a less common complication (2%) compared with conjugated hyperbilirubinemia (9%), hepatic dysfunction (30%), and need for assistive feeding (12%). The hepatobiliary dysfunction is transient and expected to improve with earlier introduction of enteral feeds and reduced duration of parenteral nutrition (Karthigesu et al., 2021).
Moreover, oral feeding physiologically involves a complex interaction between the brain, oral–motor reflexes, and the multiple muscles of the mouth, pharynx, esophagus, and face. It also requires rhythmic coordination between sucking and swallowing, simultaneously with effective breathing. Higher postnatal age at introduction of oral feeds is an independent predictor of later feeding difficulties (Patra and Greene, 2019). Almost 12% of our cohort who received hypothermia therapy needed assistive feeding (gavage or gastrostomy) feeds at home and longer time to reach full oral feeds, perhaps partly contributed by the delayed introduction of feeds.
Although rare, a minor risk of NEC remains in this cohort. The incidence of NEC in this study is comparable with Jacob et al. (2011) who reported higher incidence of rectal bleeding and NEC (4%) among cooled subjects versus 2% among controls. However, it is higher than the baseline rates of NEC reported by other trials (Azzopardi et al., 2009) and observational studies (Thyagarajan et al., 2015; Gale et al., 2021). This study adds to the literature by identifying the key early clinical risk factors that may be associated with higher risk of NEC among neonates with HIE. The presence of renal failure, coagulopathy, hepatic dysfunction, and thrombocytopenia in the first week of life is associated with increased odds of developing any stage NEC, however, there was no association with hypothermia therapy, stage of encephalopathy, abnormal brain MRI, or cardiac dysfunction.
It is well known that fetuses would preserve blood perfusion to essential organs by rapid centralization of blood flow in favor of the brain, heart, and adrenals at the expense of almost all peripheral organs such as intestines, kidneys, liver, and bone marrow, in the face of a hypoxic insult (Jensen et al., 1999). We speculate that the risk of NEC in our cohort is related to the degree of reduction in splanchnic circulation during the primary hypoxic-insult rather than the degree of secondary brain injury, postnatal cardiac dysfunction, and hypothermia treatment per se. The incidence of transient hepatic dysfunction in our study was comparable with reports from selective head cooling trials (Jacobs, 2005; Zhou et al., 2010), and slightly higher than reported by whole-body cooling trials (Shankaran et al., 2005). The rate of renal dysfunction and assistive feeding techniques was comparable with other whole-body hypothermia trials (Shankaran et al., 2005).
The study had several limitations. Due to the retrospective study design, the assessment of stage of encephalopathy and the decision to initiate therapeutic hypothermia could not be standardized. Although the unit policy stated moderate-to-severe encephalopathy as the eligibility criteria for cooling, we found neonates with mild HIE were also offered therapeutic hypothermia based on clinician's decision. The inclusion of this group makes the study more pragmatic, given that therapeutic drift is a well-recognized phenomenon of recent times and many mild HIE neonates are exposed to hypothermia and delayed enteral feeds (Goswami et al., 2020). The commonly encountered reasons for noninitiation of hypothermia was clinical presentation after 6 hours of life. The common reasons for discontinuation were significant coagulaopathy and oxygenation failure.
Almost 90% of the neonates who were discontinued from hypothermia protocol were outborn, which indicates some neonates may have been deemed to be meeting the criteria for therapeutic hypothermia at the peripheral center, but upon arrival at the tertiary care were noted to be normal. Furthermore, there was lack of a consistent definition for disseminated intravascular coagulation, coagulopathy, and transfusion guidelines. We noted a significant association between a high INR and risk of NEC, but unable to delineate whether this association is due to a common pathway of insult versus complications of induced hypothermia versus NEC secondary to multiple blood transfusions given as a response to a high INR. The rate of coagulopathy in our study was higher (37% vs. 18%) compared to a prospective whole-body hypothermia trial (Shankaran et al., 2005), which likely reflects differences in defining coagulopathy. The study is particularly challenging given that the outcomes (multiorgan failure) are coexistent with each other rather than exposure (perinatal asphyxia)-outcome sequence. In addition, some of the morbidities such as the need for assistive feeding may have originated from nongastrointestinal morbidities such as basal ganglia injury. Future studies may be able to better assess the mechanistic pathways behind these associations. Lastly, our data were limited to discharges from a tertiary care unit. Almost 86 (36%) of our cohort were discharged with gavage tube to level II centers and their feeding ability at home discharge was unknown.
Our results demonstrate the risk of gastrointestinal morbidities and short-term feeding outcomes in a cohort of neonates who received and did not receive therapeutic hypothermia, either because hypothermia was not indicated or contraindicated. There is a small risk of NEC, most likely related to the degree of reduction in fetal blood flow to the liver, intestine, and kidneys during the primary insult rather than hypothermia therapy per se. Compared with neonates who did not receive hypothermia, neonates who received 72 hours of hypothermia therapy tend to have less brain injury on neuroimaging but need longer time to reach full enteral feeds, without any difference in the risk of NEC. This opens an exciting new avenue for prospective trials of strategies encouraging early enteral feeds, positive oral stimulations, and encouraging mother–infant bonding to reduce the negative effects on the gastrointestinal system.
Footnotes
Acknowledgments
We acknowledge the contributions of Wendy Seldeitz and the McMaster Children's Hospital Data management team for meticulous data entry and retrieval.
Statement of Ethics
The study was approved by Hamilton Integrated Research Ethics Board with a waiver of consent [REB# 13850-C] dated July 1, 2021.
Authors' Contributions
F.P.: A research student who completed the project toward a undergraduate thesis work under the supervision of I.G., and involved with data collection and article writing. A.M.: Involved in data collection and critical review of the article. I.G.: Study conceptualization, student supervision and principal investigator, data analysis, and article writing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.