
Abstract
Hypothermia has multiple physiological effects, including decreasing metabolic rate and oxygen consumption (VO2). There are few human data about the magnitude of change in VO2 with decreases in core temperature. We aimed to quantify to magnitude of reduction in resting VO2 as we reduced core temperature in lightly sedated healthy individuals. After informed consent and physical screening, we cooled participants by rapidly infusing 20 mL/kg of cold (4°C) saline intravenously and placing surface cooling pads on the torso. We attempted to suppress shivering using a 1 mcg/kg intravenous bolus of dexmedetomidine followed by titrated infusion at 1.0 to 1.5 μg/(kg·h). We measured resting metabolic rate VO2 through indirect calorimetry at baseline (37°C) and at 36°C, 35°C, 34°C, and 33°C. Nine participants had mean age 30 (standard deviation 10) years and 7 (78%) were male. Baseline VO2 was 3.36 mL/(kg·min) (interquartile range 2.98–3.76) mL/(kg·min). VO2 was associated with core temperature and declined with each degree decrease in core temperature, unless shivering occurred. Over the entire range from 37°C to 33°C, median VO2 declined 0.7 mL/(kg·min) (20.8%) in the absence of shivering. The largest average decrease in VO2 per degree Celsius was by 0.46 mL/(kg·min) (13.7%) and occurred between 37°C and 36°C in the absence of shivering. After a participant developed shivering, core body temperature did not decrease further, and VO2 increased. In lightly sedated humans, metabolic rate decreases around 5.2% for each 1°C decrease in core temperature from 37°C to 33°C. Because the largest decrease in metabolic rate occurs between 37°C and 36°C, subclinical shivering or other homeostatic reflexes may be present at lower temperatures.
Introduction
Manipulating temperature has been used as a therapeutic intervention for decades. Induced mild hypothermia is used to treat brain injury in patients recovering from cardiac arrest, and hypothermia is one tool for reducing brain edema and other injurious processes after stroke or traumatic brain injury (Doufas et al., 2003; Polderman, 2009; Weant et al., 2010). Induced hypothermia changes many aspects of animal physiology, but which effects are most important for any therapeutic intervention is unknown. Reduction of energy consumption and metabolic rate is one potential mechanism mediating the effect of induced hypothermia on disease processes, and animal models suggest that energy expenditure decreases 7–8% for each degree Celsius decrease in core temperature (Mickenfelder, 1968; Polderman, 2009; Rittenberger et al., 2019).
However, there are few data on the relationship between mild induced hypothermia and metabolic rate in humans. Understanding this relationship may allow for temperature and metabolic manipulation to be utilized for nondisease states, such as to prolong survival time waiting for rescue in emergency situations where oxygen supply/carbon dioxide (CO2) removal can be severely limited. In this study, we investigated the association between temperature and metabolic rate in humans.
We previously demonstrated that induction of mild hypothermia without shivering is possible and safe in spontaneously breathing healthy volunteers in an effort to explore whether whole-body hypothermia could be used safely in persons who were not comatose, anesthetized, or artificially ventilated (Callaway et al., 2015; Rittenberger et al., 2021; Rittenberger et al., 2019). In this study, we used indirect calorimetry to estimate whole-body metabolic rate, expressed as oxygen consumption (VO2), at different core body temperatures. We aimed to quantify the magnitude of reduction in VO2 as we reduced core temperature in lightly sedated healthy individuals.
Methods
The University of Pittsburgh Human Research Protections Office approved this study. All participants provided written informed consent before participation. We recruited healthy adults between the ages of 18 and 65. On a screening visit, participants completed the Physical Activity Readiness Questionnaire to confirm healthy status and readiness for exercise (Bredin et al., 2013). We excluded individuals with a history of active heart, vascular, or gastrointestinal disease, prior abdominal surgery, history of renal or hepatic impairment. We also excluded individuals with known allergy to our study sedative, dexmedetomidine. We excluded women who were pregnant or breastfeeding. On physical examination, we confirmed normal oral temperature (>36°C), heart rate (>50 beats per minute [bpm]), systolic blood pressure (100–160 mmHg), and diastolic blood pressure (≤90 mmHg). We obtained a 12-lead electrocardiogram and excluded individuals with any electrical conduction abnormalities.
Baseline information included age, body composition using body mass index, and calculated percent body fat. We estimated body fat using the Jackson Pollack method based on three-site skinfold caliper measurements at chest, abdomen and knee for males, and at triceps, superior iliac crest, and knee for women (Jackson et al., 1978).
Study protocol
Participants made three visits to the laboratory: (1) screening to confirm eligibility and to measure exercise capacity and maximal oxygen consumption (VO2 max), (2) baseline to measure resting metabolic rate (RMR), and (3) temperature manipulation testing.
Screening and maximal exercise assessment
Upon arrival to the laboratory, we obtained baseline demographics as well as oral temperature, arm cuff blood pressure and heart rate. Participants capable of becoming pregnant completed a urine pregnancy test. The protocol was not started if heart rate was <45 bpm or >100 bpm, systolic blood pressure was <100 mmHg or >160 mmHg, or if a participant's pregnancy test was positive. We asked participants to refrain from caffeine for at least 6 hours, and fast for at least 3 hours before performing the test.
We measured exercise capacity and maximal VO2 on a treadmill using the Modified Bruce Protocol in which treadmill incline and speed increases every 3 minutes until an individual can no longer continue the exercise (ACSM, 2018). We measured VO2 using open circuit spirometry (Parvomedics Inc., Sandy, UT, USA). After the treadmill test, we monitored participants for recovery for at least 30 minutes or until vital signs had returned to baseline.
Baseline testing: RMR (VO2) assessments
During a subsequent study visit, we measured VO2 using indirect calorimetry and ventilated-hood (canopy) technique (Parvomedics Inc.). In brief, this technique requires a participant to rest quietly under a hood while the metabolic cart samples the air within the canopy system to measure VO2 and CO2 excretion. The difference in gas exchange is used to estimate total metabolic rate (Parvomedics Inc.). We performed resting metabolic assessments between 8 am and 10 am to standardize effects of circadian rhythm. We asked participants to refrain from exercise, food, caffeine, and tobacco for 12 hours before their visit. Participants rested quietly for 30 minutes before obtaining measurements. Over a 30-minute observation period, we measured VO2, respiratory rate (RR), heart rate (HR), and calculated estimated kcal/day.
Experimental condition and temperature manipulation
Experiments started between 8 am and 11 am. We asked participants to refrain from eating or drinking (with the exception of water) for 6 hours and from caffeine or alcohol consumption for a minimum of 12 hours. At least 1 hour before starting the study, participants swallowed an ingestible core temperature pill (CorTemp; HQInc., Palmetto, FL, USA), which transmits core gastrointestinal temperature to a radio receiving unit and is our measure of core temperature. We inserted an 18 g or 20 g intravenous catheter into a vein above the wrist and below the shoulder bilaterally. Participants wore light athletic clothing in a laboratory with an ambient temperature between 20°C and 22°C.
We administered an intravenous bolus of 1.0 μg/kg dexmedetomidine in normal saline over 10 minutes, followed by an infusion starting at 1.0 μg/(kg·h). We increased the infusion by increments of 0.1 μg/(kg·h) if shivering occurred up to a maximum dose of 1.5 μg/(kg·h). To induce hypothermia, we rapidly infused 20 mL/kg (up to maximum of 2 L) of cold (4°C) 0.9% saline with a pressurized bag. After the saline infusion, we placed EMCools Flex Pads (EMCools, Traiskirchen, Austria) and cold ice packs (if necessary) were placed on the front and back of the participant's torso and legs. We left these ice packs in place until the participant reached a core temperature of 32°C, for a maximum of 6 hours, or if shivering could not be controlled despite maximum dexmedetomidine infusion rate. We monitored HR, RR, blood pressure, pulse oximetry, and end-tidal CO2 throughout the protocol.
We measured VO2 using the same indirect calorimetry canopy method. We recorded VO2 before beginning hypothermia (37°C), and at each 1°C decrease in core body temperature thereafter. We recorded VO2 after cooling was stopped, at each 1°C increase in core body temperature during the rewarming phase, and before discharge.
Shivering, sedation, and comfort assessments
We recorded Bedside Shivering Assessment (BSAS) and Richmond Agitation Sedation Scale (RASS) every 15 minutes. The BSAS is a 4-point scale to quantify patient shivering with 0, “no shivering”; 1, “shivering in jaw”; 2, “shivering including upper extremities”; and 3, “severe shivering-generalized or sustained upper/lower extremity shivering” (Badjatia et al., 2008). The RASS is a 10-point scale used to monitor sedation that ranges from −5, “unresponsive to voice or painful stimulation” to 4, “combative and danger to self or staff” (Ely et al., 2003; Sessler et al., 2002). Participants reported Thermal and Comfort Sensation scales at baseline, minutes 10, 20, 30, and every 30 minutes thereafter for the duration of the protocol. Thermal sensation was anchored by 1, “comfortable” and 5, “very cold.” Comfort was assessed using an “overall” measure of comfort scale anchored by 1, “comfortable” and 4, “very uncomfortable.”
Starting, stopping, and recovery criteria
We did not start the protocol if the participant had initial HR <45 or >100 bpm, RR <6 or >24, or systolic blood pressure <100 mmHg or >160 mmHg. We stopped the protocol if mean arterial pressure was <65 mmHg for >5 minutes, if oxygen saturation declined <90% for >1 minute, if the participant became deeply sedated (RASS −4), if a dexmedetomidine infusion rate of 1.5 mcg/(kg·h) failed to suppress shivering, if the participant requested to stop, or if a study physician decided that continuing was not safe.
At the end of cooling, we stopped the dexmedetomidine infusion and removed cooling pads. We monitored participants for a minimum of 90 minutes until sedation score was 0, they were able to eat or drink, able to ambulate safely, and a study physician deemed the participant safe to be discharged.
Statistical analyses
We reported descriptive statistics for all dependent variables. Data summaries are represented as mean and standard deviation if normally distributed, median and interquartile range (IQR) if data followed a non-normal distribution. Ordinal data are represented as number and percentages. We tested for an association between temperature and VO2 using linear regression accounting for clustering, because VO2 measurements were repeated within participants. We used an alpha error rate of 0.05 to define statistical significance. This was an exploratory analysis investigating the magnitude of change in metabolism with cooling and, therefore, we did not perform a formal power analysis.
We based our sample size on our prior study where we were able to detect physiological changes in healthy subjects with similar group size (Callaway et al., 2015; Rittenberger et al., 2021). We calculated the temperature coefficient, Q10 (temperature-dependent decrease in a reaction rate, such as metabolism, as defined by the ratio of metabolic rates at temperatures 10°C apart) for VO2 as (VO2 @ 37°C)/(VO2 @ Temp) (10/[37-Temp]) using all participant data with temperature <37°C and no shivering (BSAS = 0). We used STATA 16 (College Station, TX, USA) for all statistical analyses, and GraphPad Prism 7 (San Diego, CA, USA) for all graphical representations.
Results
Nine participants were enrolled and completed the study. Baseline characteristics are shown in Table 1. Core temperature decreased in all participants to between 35°C and 33°C (Fig. 1). Median VO2 declined with a decrease in core temperature, unless shivering occurred (Table 2). Using observations without shivering (BSAS = 0), VO2 was associated with temperature (slope = 0.18 ± 0.04; p < 0.001). Over the entire range from 37°C to 33°C, median VO2 declined by a median difference of −1.06 mL/(kg·min) [IQR 0.58–1.10 mL/(kg·min)] in the absence of shivering. After a participant developed shivering, core body temperature did not decrease further, and VO2 increased (Fig. 2). The largest decrease in VO2 in the absence of shivering (BSAS = 0) occurred between 37°C and 36°C, with a median difference of −0.70 mL/(kg·min) [IQR 0.24–0.82 mL/(kg·min)]. These data correspond to a median Q10 of 2.83 (IQR 2.00–4.95).
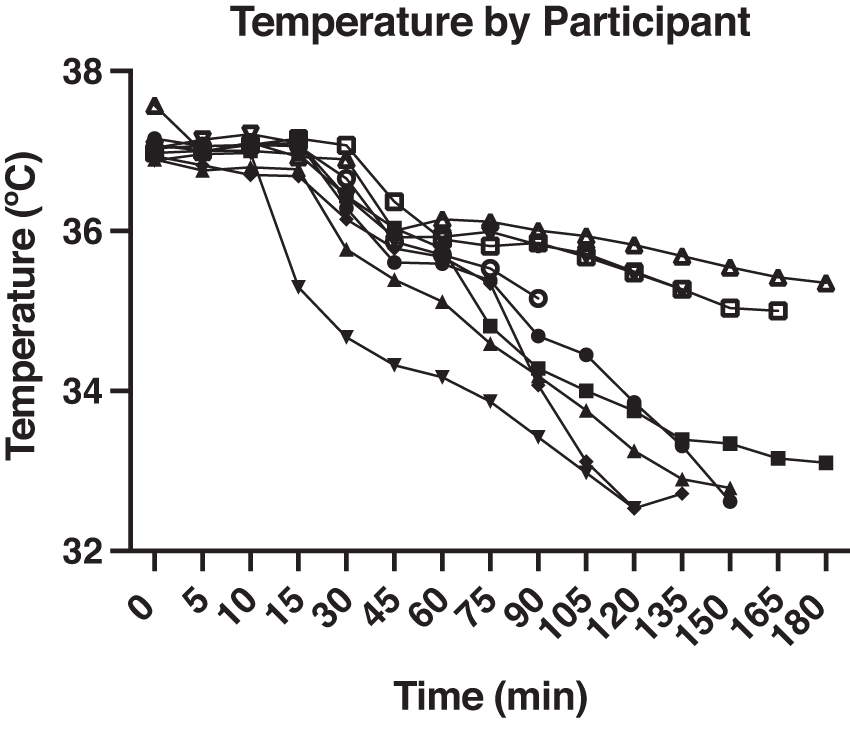
Change in individual participant temperature over time.

Participant Baseline Characteristics
IQR, interquartile range; VO2, oxygen consumption; VO2 max, maximal oxygen consumption.
Physiological Changes During Cooling
Values are median (IQR).
BSAS, Bedside Shivering Assessment; DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure; RASS, Richmond Agitation Sedation Scale; SBP, systolic blood pressure.
Most participants (n = 5) experienced little to no shivering, with a BSAS of 0 or 1 (Table 2). Among participants who had maximal shivering, a BSAS of 2 or greater, core temperature never decreased below 35°C. In all participants who had a maximal BSAS 0, −1, core temperature declined to 33°C (Fig. 2). Cold sensation measured with the thermal scale and discomfort on the comfort scale increased with declining temperature (Table 2). Heart rate decreased with declining temperature, whereas mean, systolic, and diastolic pressures did not change (Table 2). Sedation was mild, with median RASS score of −1 (IQR 0, −1) (Table 2).
Discussion
We observed a 20.8% overall decrease in VO2 in nine healthy participants while lowering core temperature from 37°C to 33°C with external cooling and intravenous sedation (5.2%/°C). We were able to cool 5 participants to 33°C; however, when shivering occurred cooling produced no further decrease in core temperature despite light sedation. Participants with visible shivering also promptly increased VO2. These data support the hypothesis that VO2 decreases with decreasing body temperature unless shivering occurs.
Hypothermia-induced metabolic reduction over the entire temperature range in our study (5.2%/°C) is less than the 7–8%/°C decrease noted by animal studies (Mickenfelder, 1968) and the 8%/°C change in cerebral metabolic rate reported during deep hypothermic circulatory arrest (McCullough et al., 1999). We estimated Q10 for VO2 to be 2.8, which is similar to the estimate of Q10 for cerebral metabolic rate of 2.3 (McCullough et al., 1999). Our study results are grossly similar to animal studies and cerebral metabolic studies. However, the relationship between temperature and metabolism may be altered in critically ill patients, which may explain this difference.
For instance, prior study found that in patients who are septic, metabolism is negatively correlated with illness severity, and positively correlated with temperature (Zauner et al., 2001). Future study should continue to explore this relationship between metabolism, temperature, and critical illness, and if the relationship differs based on if a patient is hyper or hypothermic. Importantly, we found a 13% decrease in metabolism between 37°C and 36°C, with smaller changes thereafter. This difference may be because individuals had subclinical shivering at lower temperatures that increased VO2 and offset any temperature-induced decrease in VO2. In contrast, preclinical studies often paralyzed animals removing any contributions to VO2 increase from shivering (Mickenfelder, 1968).
We have reported previous studies describing comfort, safety, and shivering mitigation for inducing hypothermia in spontaneously breathing individuals (Callaway et al., 2015; Rittenberger et al., 2021; Rittenberger et al., 2019). These studies highlight the importance of suppressing shivering both to achieve hypothermia and to minimize discomfort. The threshold for shivering in healthy humans is around 36.3°C, and many drugs can lower this threshold (Doufas et al., 2003; Lopez et al., 1994; Weant et al., 2010). In this study, we used the alpha-2-adrenergic drug dexmedetomidine, which we and others have found to be effective for lowering the shivering threshold without suppressing respiratory drive (Callaway et al., 2015; Doufas et al., 2003).
Hypothermia protocols for spontaneously breathing participants might have utility for treating diseases in patients or settings where general anesthesia or paralysis are undesirable. Acute myocardial disease, shock, or stroke are examples. Metabolic reduction could also have utility in nondisease states, such as to prolong survival time waiting for rescue in emergency situations where oxygen supply/CO2 removal can be severely limited. Examples include CO2 scrubber malfunctions in submarines or during spaceflight. Lowering metabolic rate of inactive crew or passengers may also be useful for reducing use of consumables and creation of waste during long-duration spaceflight or similar austere conditions (Regan et al., 2020; Rittenberger et al., 2019).
There are several limitations of this study. Of the nine participants, only five reached temperatures below 35°C because the remaining four participants experienced severe shivering (BSAS 2, −3). Temperatures did not decrease at consistent rates (both within and between participants), and we cannot exclude that physiological responses might differ depending on how quickly temperature changes. In some participants, despite the visual absence of shivering (BSAS 0), VO2 increased with a decrease in temperature, suggesting that subclinical shivering may have been present and impacted metabolism.
BSAS relies on visual assessment of shivering and may not be sensitive enough for this type of analysis. Finally, there was an imbalance in the number of men and women in our cohort, with the majority (n = 7) of the participants being male. Previous study suggests that although women thermoregulate at a higher temperature than men, their shivering thresholds are similar (Lopez et al., 1994). However, we do not know if the relationship between metabolism and lower core temperature differs between men and women.
Future studies should further investigate the relationship between metabolic rate and temperature, and how this may vary by sex, and seek to optimize shivering assessment and mitigation methods. Earlier detection of shivering may allow for earlier deployment of mitigation strategies and, therefore, more successful shivering prevention and metabolic suppression. To assess the utility of metabolic suppression for complex environments such as spaceflight, future studies should also investigate nutritional and exercise strategies that further facilitate the metabolic suppression while also preventing muscle atrophy. Changes in cognition, decision-making, and psychomotor vigilance during metabolic suppression also need to be characterized.
Conclusion
In lightly sedated humans, metabolic rate (VO2) decreases 5.2% for each 1°C decrease in core temperature from 37°C to 33°C. When shivering occurs, metabolic rate increases. The largest decrease in metabolic rate occurs between 37°C and 36°C with smaller decreases thereafter, suggesting that subclinical shivering or other homeostatic reflexes are present.
Footnotes
Authors' Contributions
Methodology, software, validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, and project administration by K.L.F. Methodology, validation, formal analysis, investigation, writing—review and editing, visualization, supervision, and project administration by A.W. Investigation and writing—review and editing by J.E., F.X.G., P.J.C., C.D., D.H., A.F., and A.A.D. Investigation, resources, writing—review and editing, and project administration by M.J.R. Conceptualization, methodology, investigation, writing—review and editing, supervision, and project administration by J.C.R. Conceptualization, methodology, software, validation, formal analysis, investigation, writing—review and editing, visualization, supervision, and funding acquisition by C.W.C.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was funded in part by the Translational Research Institute through NASA (NNX16AO69A).