
Abstract
To investigate the effect of forced-air warming and heated intravenous (IV) and irrigation fluids alone and in combination on body temperature, shivering, thermal comfort, pain, nausea and vomiting in adult patients undergoing surgery under general anesthesia in a prospective, four-group, randomized controlled trial. After induction of anesthesia, 120 patients were divided into the following groups: patients warmed with forced-air warming (n = 30), patients receiving warmed IV and irrigation fluid (n = 30), patients receiving warmed IV and irrigation fluid with forced-air warming (n = 30), and the control group without any intervention (n = 30). Body temperature, shivering, thermal comfort, pain, nausea and vomiting were monitored in the first 24 hours after surgery. The general characteristics of the groups, mean body temperature, length of stay, ambient temperature, and duration of surgery in the preoperative waiting unit were similar (p > 0.05). Compared with the other groups, patients in the control group had a significant decrease in body temperature from the 30th minute during surgery (p < 0.001), lower body temperature in the first 2 hours and thermal comfort in the first three hours after surgery (p < 0.01), and higher shivering levels in the first hour after surgery (p < 0.01). There was no significant difference between the groups in terms of postoperative pain, nausea and vomiting (p > 0.05). The study findings showed that normothermia was maintained in all three intervention groups during the surgery and in the first 24 hours after surgery. Moreover, postoperative thermal comfort increased and shivering levels decreased compared with the control group, but pain, nausea and vomiting levels were not affected. The study was registered on ClinicalTrials.gov (NCT04907617).
Introduction
Involuntary perioperative hypothermia (IPH), defined as a decrease in body core temperature <36°C from the preoperative period (1 hour before anesthesia) to the postoperative period (first 24 hours after anesthesia) (Bilgin, 2017), is a preventable adverse outcome of general anesthesia and surgery (Steelman Victoria et al., 2013). Although it frequently develops in the first hour of anesthesia, its incidence in the perioperative period ranges from 26% to 90% (Giuliano and Hendricks, 2017; Sun et al., 2015). Reduced metabolic heat production due to anesthetics, cold operating room environment, prolonged exposure of large skin surfaces to cold, significant blood loss during long surgical procedures, transfusion of large amounts of cold blood and/or blood products, heat loss due to intravenous (IV) and irrigation fluids, and impaired thermoregulation resulting in the redistribution of heat from the center to the periphery contribute to this problem (Bilgin, 2017; Madrid et al., 2016; McSwain et al., 2015).
Disturbances in thermoregulation can lead to serious complications such as hemostatic, coagulation, cardiac and renal dysfunction, liver and immune system dysfunction, and delayed wound healing (Iden and Höcker, 2017), leading to increased morbidity and even mortality (Hooper et al., 2009; Kiekkas et al., 2018). This may result in prolonged hospital (Jeyadoss et al., 2013) and intensive care unit stays, increased costs (Kiekkas et al., 2018; Lista et al., 2012), and decreased patient satisfaction (Burlingame and Conner, 2018; Hegarty et al., 2009; Hooper et al., 2009). Therefore, achieving and maintaining perioperative normothermia is important for optimal surgical outcomes, as well as patient safety and satisfaction (Rauch et al., 2021; Steelman Victoria et al., 2013).
Studies to prevent perioperative hypothermia have focused on providing heat sources (e.g., active heating methods: forced-air warming, heating fluids) and preventing heat loss (e.g., passive heating methods: covering the patient with warm blankets) (Kurnat-Thoma et al., 2016; McSwain et al., 2015). Evidence-based guidelines also recommend determining the patient's risk of hypothermia, close monitoring of body temperature (National Institute for Health and Clinical Excellence (NİCE), 2021), and the application of hypothermia prevention methods (Kang and Park, 2020; NİCE, 2021; Rauch et al., 2021). Since perioperative passive heating methods alone are not sufficient (Kang and Park, 2020), it has been emphasized that every patient who undergoes surgery with general anesthesia lasting >30 minutes and the fluids to be administered to the patient should be warmed with active heating methods (Hooper et al., 2009; Rauch et al., 2021).
In this context, the forced-air warming system is the most effective method (Burlingame and Conner, 2018). Another method recommended during the operation is the administration of heated fluids (Burlingame and Conner, 2018; Rauch et al., 2021). With no reported adverse effects, the efficacy of these methods on maintaining intraoperative normothermia and improving postoperative complications is clear with varying levels of evidence. However, well-designed studies comparing the efficacy of the methods are needed to clarify the clinical benefit and to demonstrate improved clinical outcomes for perioperative nurses.
Shivering is reported in 5–65% of patients in the early postoperative period due to IPH (Buggy and Crossley, 2000). Shivering, which intensifies after anesthesia, leads to deterioration of the thermal comfort of patients (Alderson et al., 2014; Bilgin, 2017; Hooper et al., 2009; TARD, 2013), postoperative pain (Lopez, 2018; Sessler et al., 1991), nausea and vomiting (Lopez, 2018).
In the literature, there are often studies focusing on the relationship of IPH with shivering (Aydın ve ark., 2019; Kim et al., 2019; Park et al., 2012) and thermal comfort (Campbell et al., 2015; Chebbout et al., 2017; Kang and Park, 2020; Madrid et al., 2016; Torossian et al., 2015), but there are limited studies focusing on the relationship with postoperative pain (Benson et al., 2012; Pu et al., 2014), nausea and vomiting (Aydın et al., 2019; Ayhan et al., 2018). These complications are not life threatening, but they need to be prevented and treated because they affect the patient's overall comfort and satisfaction with care (Sessler, 2016).
Perioperative nurses have important roles and responsibilities in the prevention and treatment of IPH and its related complications (Su and Nieh, 2018). This provides perioperative nurses with the opportunity to determine the best clinical practice (Bender et al., 2015).
Despite the recommendations of national (TARD, 2013) and international studies and guidelines (Hooper et al., 2009; NICE, 2021) to prevent IPH, it is known that there is no standard for monitoring and taking necessary precautions in clinical practices in Turkey. Active heating systems are used more in pediatric patients than in adult patients (Aksu et al., 2019), while passive heating methods are mostly preferred in adults (80.3%) (Koyuncu et al., 2022). Moreover, in studies in Turkey, it has been reported that the incidence of involuntary hypothermia was 69.9% in the first hour of surgery (Duman and Yılmaz, 2016) and 62.4% after surgery (Aldemir and Yilmaz, 2021).
Furthermore, it has been stated that temperature monitoring is not performed in 91% of patients to prevent perioperative hypothermia (Duman and Yılmaz, 2016), a very low proportion of patients (5.6%) are warmed intraoperatively with a hot forced-air warming system (Öner Cengiz et al., 2021) and heated fluids are administered (5.54%) (Aksu et al., 2019). The results of these studies conducted in different regions in Turkey are consistent with our clinical observations, and there is no standardized approach in line with current recommendations to prevent perioperative hypothermia in the institution where the study was conducted.
In light of this, the study aimed to investigate the effects of forced-air warming and heated IV and/or irrigation fluids alone and in combination on outcomes for perioperative nurses, namely postoperative body temperature, shivering, thermal comfort, pain, nausea and vomiting in adult patients undergoing surgery under general anesthesia, and to compare the effectiveness of these interventions. In light of this, the study aimed to investigate the effects of forced-air warming and heated IV and/or irrigation fluids alone and in combination on outcomes for perioperative nurses, namely postoperative body temperature, shivering, thermal comfort, pain, nausea and vomiting in adult patients undergoing surgery under general anesthesia and to compare the effectiveness of these interventions.
Null Hypothesis
There is no significant difference in body temperature, shivering, thermal comfort, pain, nausea and vomiting between patients who are warmed during the surgery with forced-air warming and heated IV and/or irrigation fluids alone and in combination and patients who do not receive any active heating.
Materials and Methods
Study design
This study was a prospective, four-group, and randomized controlled trial.
Sample and setting
This study was conducted between February 19, 2021 and July 01, 2021 in the operating room and surgical clinics of a university hospital in the Central Anatolia region of Turkey. As a routine practice in the institution in question, patients are delivered to the operating room with a stretcher/wheelchair accompanied by the ward nurse after removing all their clothes, putting on an operating shirt, measuring their vital signs, and covering them with a blanket. Patients are kept waiting in the preoperative waiting unit for ∼10–15 minutes, and then taken to the operating room.
The operating shirt is removed, and the patients are covered with surgical drapes; and IV fluids, irrigation solutions, blood, and/or blood products are administered at the temperature of the operating room according to the physician's order. Besides, 100 mg (milligram) Tramadol HCl (hydrochloride) (Trade name: Tramosel 100 mg ampoule), and Metoclopramide HCl (Trade name: Emoject 10 mg/mL (milligram/milliliter) Ampoule Containing Solution for Infusion) are administered in the last 10–15 minutes of the operation to control pain, nausea and vomiting.
After surgery, patients are transferred to the postanesthesia care unit (PACU) with surgical drapes over them. Patients stay in the PACU for ∼15–20 minutes, during which time their vital signs are measured and their treatment is continued. With the approval of the physician, the patients are transferred to the clinic by the PACU nurse with surgical drapes on them. In postoperative surgical clinics, if patients express that they are very cold or shivering, they are covered with additional hospital blankets. Analgesics (twice/day, on average) and antiemetics (once/day, on average) are administered for 1–2 days for pain control.
Since the power of the study is expressed as 1-β (β = probability of type II error) and studies should have 80% power, in general, the sample size was determined, considering that the evaluations between independent groups should have a large effect (d = 0.8) according to Cohen's effect size coefficient (Cohen, 1992). Based on the body temperature measurement in the previous study (Chebbout et al., 2017), it was calculated that a total of 104 patients should be included in the study with 26 patients in each group. Considering the 10% possible data loss in the study, it was decided to enroll a total of 120 patients, 30 in each group.
Inclusion criteria were as follows: being ≥18 years of age, undergoing surgery with general anesthesia, undergoing surgery longer than one hour, being in ASA class I-III, having no disability that would make communication difficult, communicating in Turkish, and giving informed written consent to participate in the study.
Exclusion criteria were as follows: having a preoperative body temperature >37.5°C or <36°C, undergoing a surgical procedure that prevents body temperature measurement through the tympanic route, intraoperative therapeutic hypothermia, head trauma or brain injury that affects body temperature (Fanelli et al., 2009), and drug treatment that would affect thermoregulation (Choi et al., 2016). Removal criteria were deterioration in general condition during and/or after surgery, exitus, and postoperative patient-controlled analgesia.
Randomization and allocation
Patients who met the inclusion criteria according to the order of hospitalization were randomly assigned to one of the four groups by matching with the randomization table created with a random number generator (www.randomizer.org). After induction of anesthesia, group 1 was warmed only with forced-air warming, group 2 received only warmed IV and irrigation fluids, group 3 received warmed IV and irrigation fluids with forced-air warming, and group 4 (control) received routine care.
Blinding
To prevent them from being affected by heating methods, a single-blind study design was used in which the interventions to be applied were explained to the participants while obtaining their informed written consent, but the participant did not know which group they were assigned to (Boutron et al., 2007).
Outcome measures and instruments
The primary outcome of this study is body temperature. Secondary outcomes of the study include postoperative shivering, thermal comfort, pain, nausea and vomiting.
Data were collected using “Descriptive Characteristics Form,” “Patient Follow-up Form,” “Thermal Comfort Scale,” “Bedside Shivering Scale,” “Numeric Rating Scale (NRS),” “Nausea and Vomiting Scale,” and “Modified Aldrete Score (MAS)” by the first author of the study.
Descriptive Characteristics Form: This form, which was developed based on the literature (Alderson et al., 2014; Burlingame and Conner, 2018; NİCE, 2021; TARD, 2013), included questions to determine the individual (age, gender, body mass index, presence of comorbid diseases, and history of surgery) and clinical characteristics (ASA class and duration of hospitalization) of the patients.
Patient follow-up form
This form, which was prepared in line with the literature (Burlingame and Conner, 2018; NİCE, 2021; TARD, 2013), consisted of four sections. The first part included information on vital signs (body temperature, blood pressure, pulse rate, and respiratory rate) and oxygen saturation, thermal comfort score, waiting time, and ambient temperature recorded in the waiting unit of all patients who were transferred from the surgical clinic to the operating room before surgery. The second section included information on vital signs, the temperature of the operating room, duration of surgery, amount of IV and irrigation fluids and blood/blood products administered, recorded at 30-minute intervals after induction of anesthesia in all patients admitted to the operating room.
In the third section, vital signs, thermal comfort score, shivering level, pain intensity, and nausea and vomiting status of all patients who were transferred from the operating room to the PACU were recorded during admission and discharge. In addition, the duration of stay in the PACU, ambient temperature, and modified Aldrete score (MAS) were recorded in this section. The fourth section included the vital signs of patients, thermal comfort score, shivering level, pain intensity, nausea and vomiting, analgesic and antiemetic requirements, and ambient temperature at 15-minute intervals for the first hour after admission from the PACU to the clinic and at the 2nd, 3rd, 4th, 12th, and 24th hour thereafter.
Thermal comfort scale
Based on previous studies (Ayhan et al., 2018; Horn et al., 2012), in this study, patients' thermal comfort was assessed using a Visual Analog Scale with 0 (extremities too cold) at one end, 50 [no discomfort (no shivering or sweating)] in the middle, and 100 (extremities too hot) at the other end.
Bedside shivering scale
In the study, the shivering levels of the patients were evaluated based on observation with the 4-item (0 = no shivering; 1 = mild; 2 = moderate; 3 = severe) shivering scale developed by Badjiata et al. (2008).
Numeric rating scale
In the study, postoperative pain intensity was assessed by NRS based on patients' self-report (0 = no pain, 1–3 = mild pain, 4–6 = moderate pain, 7–10 = severe pain) (Chou et al., 2016).
Nausea and vomiting scale
Based on the previous study (Ayhan et al., 2018), patients' postoperative nausea and vomiting status was evaluated as 0 = no nausea, 1 = nausea, and 2 = vomiting.
Modified Aldrete score
The discharge score of the patients from the PACU was obtained with the MAS. In the MAS, which consists of five factors including activity, respiration, circulation, state of consciousness, and oxygen saturation, each factor is scored between 0 and 2, and discharge from the PACU is provided with a score of >9 (Aldrete, 1995).
Interventions
Before induction of anesthesia, the patients assigned to groups 1 and 3 were covered with the cover of a forced-air warming system (Bair Hugger™ Warming Unit, Model 505; Augustine Medical, Inc., Eden Prairie, MN) with the surgical area exposed. After induction of anesthesia, the device was operated at a maximum level (43°C). When the patient's body temperature reached ≥37°C, device operation was interrupted. When the body temperature was <36.5°C, the device was turned on again (Riley and Andrzejowski, 2018). IV fluids administered to patients assigned to groups 2 and 3 were heated to 37°C with a blood and serum warming system (Automer blood/fluid warmer system, Acemedikal, South Korea), and irrigation solutions were heated to 38–40°C with a thermostatically controlled warming cabinet (Enthermic Warming Cabinet 1002 W) (NİCE, 2021).
Patients assigned to group 4 received “routine care” at the institution where the study was conducted, and no intraoperative warming intervention was applied to this group. In all groups, blood and/or blood products used in case of intraoperative requirement were administered by warming to 37°C with a blood and serum warming system (Automer blood/fluid warming system). Besides, all groups were covered with normal hospital blankets before and after surgery.
Ethical considerations
This study was approved by Marmara University Faculty of Medicine Clinical Research Ethics Committee (Protocol No: 09.2020/770) and Yozgat Bozok University Application and Research Center (Date: 14.05.2020 Number: 16142545-903.99-E.10438). The study was conducted in cooperation with the health care professionals working in the surgical clinics and operating rooms where the study was conducted after providing the necessary information.
Patients who met the inclusion criteria after hospitalization were interviewed in the patient room the day before surgery and invited for the study. They were informed about the reasons for entering the sample, research activities, and duration. Verbal and written consent was obtained from patients who volunteered and agreed to participate in the study. The principles of the Declaration of Helsinki (DTB General Assembly, Fortaleza, Brazil, October 2013) and the Law on Medical Research Involving Human Subjects were followed throughout the study. There have been no changes to the trial protocol since its start.
Statistical analysis
Data were presented as mean ± standard deviation (SD) or number and frequency. Comparisons of variables that did not show the normal distribution in three groups or more were analyzed with the Kruskal–Wallis H test. Mixed-effects linear models were used to evaluate the differences between groups in repeated measures, and Bonferroni correction was applied for the comparison of main effects. The Chi-square test and Fisher's exact test were used to compare categorical variables. Moreover, p < 0.05 was considered statistically significant.
Results
Characteristics of participants and homogeneity test
During the study period, 335 patients who underwent surgery under general anesthesia were screened, and 120 patients (53.3% single-incision laparoscopic surgery and 46.7% hand-assisted laparoscopic surgery) met the inclusion criteria (effect size = 0.375, power = 98.8%) (Fig. 1).
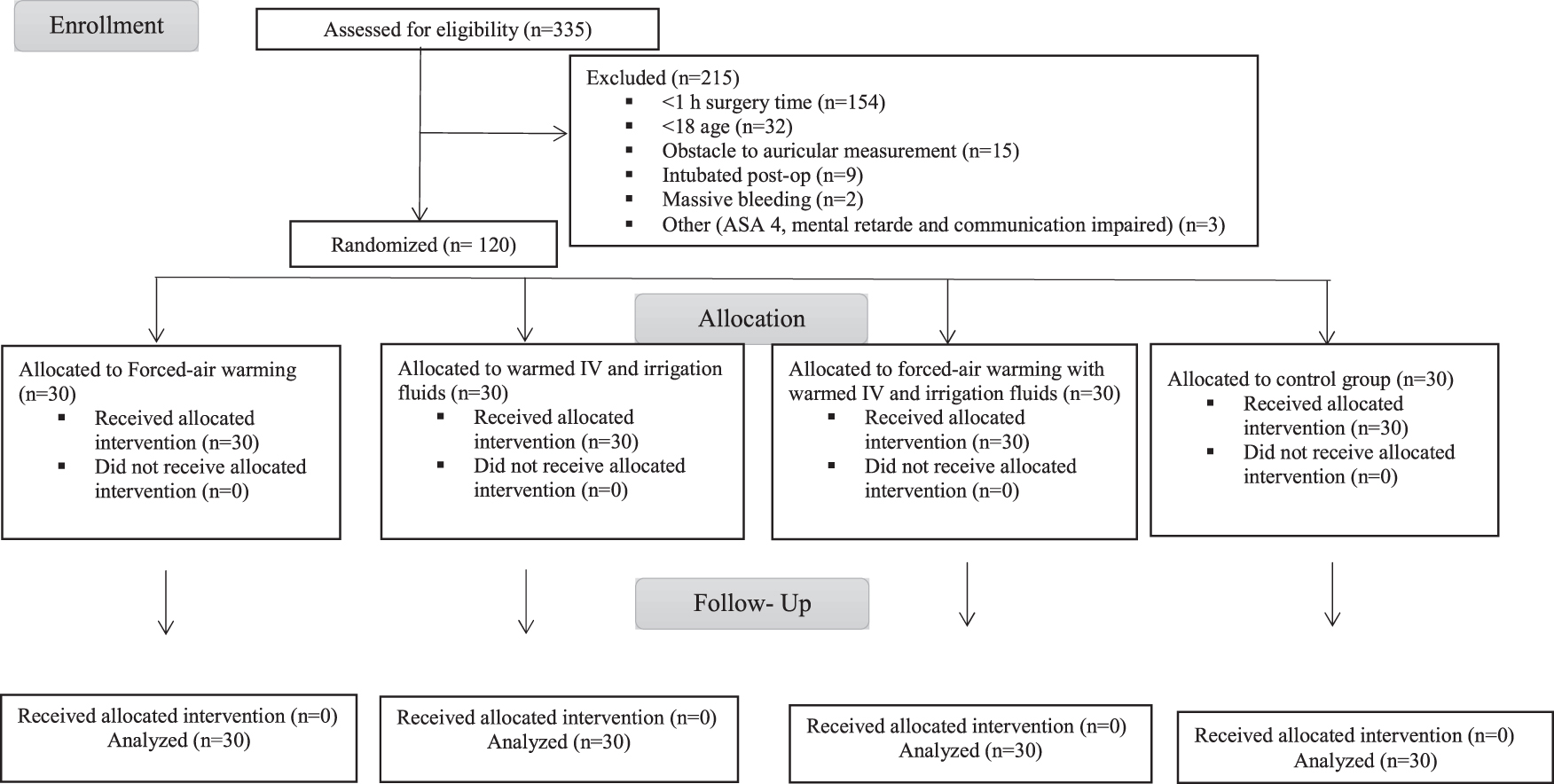
CONSORT flow diagram.
The general characteristics of the groups and homogeneity test results are shown in Table 1. There was no statistically significant difference between the four groups in terms of general characteristics. No tremor was observed in any group during admission to the preoperative waiting unit, stay, and discharge.
General Characteristics of the Groups (N = 120)
BMI, body mass index; MAS, modified Aldrete score; SILS, single-incision laparoscopic surgery; HALS, hand-assisted laparoscopic surgery; SD, standard deviation; F, ANOVA test; χ2, Fisher's exact test; H, Kruskal–Wallis H test; Group 1, Group heated by forced-air warming system; Group 2, the group given heated IV and irrigation fluid; Group 3, the group in which heated IV and irrigation fluid were applied together with forced-air warming system; Group 4, control group.
Primary outcomes: Intraoperative body temperature and comparison of the effect of interventions on body temperature
The perioperative body temperature of the groups is presented in Table 2. In the preoperative waiting unit, the mean body temperature of the groups was similar, and all groups were normothermic. Perioperative measurements at 30-minute intervals showed no significant change in the mean body temperature of groups 1, 2, and 3 (F = 1.415, p = 0.184; F = 1.131, p = 0.345; and F = 1.197, p = 0.300, respectively), whereas the body temperature of the control group patients gradually decreased (F = 8.249, p = 0.001) and was significantly lower than the intervention groups from the 30th minute after induction of anesthesia; moreover, hypothermia developed at the 60th minute (p < 0.05).
Comparison of Perioperative Body Temperature of the Groups (N = 120)
SD, standard deviation; amixed-effects model; H, Kruskal–Wallis H test.
Group 1, group heated by forced-air warming system; Group 2, the group given heated IV and irrigation fluid; Group 3, the group in which heated IV and irrigation fluid were applied together with forced-air warming system; Group 4, control group.
On admission to the PACU, no hypothermia was observed in group 3, while one patient in group 1 (intraoperative bleeding of ∼1000 cc), two patients in group 2 (operation time was ∼260 minutes), and 16 patients in the control group were hypothermic (p = 0.001). In postoperative measurements made at different time points, the body temperature of the control group patients reached 36°C, 15 minutes after admission to the surgical clinic but was significantly lower than the intervention groups until the 2nd hour (p < 0.05). There was no significant difference between the groups in terms of other vital signs (systolic and diastolic blood pressure, heart rate, and respiratory rate) and oxygen saturation, which were monitored simultaneously with body temperature in the perioperative period (p > 0.05).
When the body temperatures of the intervention groups heated with different heating methods during the surgery were compared, it was observed that there was no significant difference between the groups in terms of the mean body temperature in the first 30 minutes after induction of anesthesia (p > 0.05), but there was a significant difference in the 60th, 90th, and 120th minutes due to the higher mean body temperature of group 3 compared with groups 1 and 2 (p < 0.05) (Table 3).
Comparison of the Intraoperative Body Temperature of the Intervention Groups (N = 90)
SD, standard deviation; amixed-effects model.
Group 1, group heated by forced-air warming system; Group 2, the group given heated IV and irrigation fluid; Group 3, the group in which heated IV and irrigation fluid were applied together with forced-air warming system; Group 4, control group.
Secondary Outcomes: Comparison of postoperative shivering, thermal comfort, pain, nausea and vomiting
Compared with the intervention groups, patients in the control group had higher shivering levels in the postoperative period up to the first hour after admission to the surgical clinic, including the PACU, and significantly lower thermal comfort levels up to the third hour (Table 4). In the first 24 hours postoperatively, there was no significant difference between the groups in terms of pain intensity, nausea and vomiting levels (Table 5), and analgesic (F = 1.242, p = 0.298) and antiemetic (F = 0.569, p = 0.637) requirements.
Postoperative Thermal Comfort and Shivering Levels of the Groups (N = 120)
SD, standard deviation; PACU, postanesthesia care unit; amixed-effects model; H, Kruskal–Wallis H test; χ2, Fisher's exact test.
Group 1, group heated by forced-air warming system; Group 2, the group given heated IV and irrigation fluid; Group 3, the group in which heated IV and irrigation fluid were applied together with forced-air warming system; Group 4, control group.
Postoperative Pain, Nausea and Vomiting of the Groups (N = 120)
PNV, postoperative nausea and vomiting; SD, standard deviation; amixed-effects model; χ2: Fisher's exact test.
Group 1, group heated by forced-air warming system; Group 2, the group given heated IV and irrigation fluid; Group 3, the group in which heated IV and irrigation fluid were applied together with forced-air warming system; Group 4, control group.
Discussion
This study investigated the effect of intraoperative forced-air warming and heated IV and irrigation fluids alone and in combination on body temperature, shivering, thermal comfort, pain, and nausea and vomiting in adult patients undergoing surgery under general anesthesia. The study findings showed that all three interventions achieved intraoperative normothermia, and the group that received heated IV and irrigation fluids in combination with the forced-air warming system had the best body temperature from the 60th minute of surgery. Furthermore, the study findings showed that the interventions maintained postoperative normothermia, reduced patients' shivering, and increased their thermal comfort, but did not affect pain intensity, nausea and vomiting, and the need for analgesics and antiemetics.
Normal body temperature (>36°C) was maintained in all three intervention groups from the time of admission to the preoperative waiting unit until the first 24 hours after surgery. In contrast, in the control group patients, while the body temperature was normal in the preoperative waiting unit (36.4°C), it decreased by 0.9°C at the end of an average of 120 minutes of surgery, and hypothermia developed at 60 minutes of surgery (35.8°C).
In general, during general anesthesia, body core temperature drops by ∼1.0°C to 1.5°C in the first hour after induction of anesthesia due to a redistribution of heat from the center to the periphery due to slowed metabolism (Kang and Park, 2020; Rauch et al., 2021), which can last up to the first 24 hours after surgery (Giuliano and Hendricks, 2017; Karalapillai et al., 2013; Sun et al., 2015). In a multicenter retrospective analysis of 50,689 patients undergoing major elective noncardiac surgery, it was reported that approximately half of the patients were hypothermic in the first 24 hours after admission to the intensive care unit and >80% recovered within 3 hours of admission to the clinic (Karalapillai et al., 2013).
There are also studies reporting that the body temperature (Kurz et al., 1996) of patients who have been not warmed during surgery was significantly lower until the first (Janicki et al., 2002), second (Park and Choi, 2010), third (Frank et al., 1995; Nieh and Su, 2018), fourth (Kurz et al., 1995), and fifth hours after surgery compared with patients who have been warmed with various methods. In this study, although the body temperature of the control group patients increased to 36°C at the 15th minute after admission to the surgical clinic, it was significantly lower than that observed in all three intervention groups from the 30th minute of surgery until the 2nd hour after admission to the postoperative surgical clinic.
In each intervention group, body temperature did not fall <36.2°C neither during the surgery nor during the first 24 hours after surgery. This provided evidence for the effect of all three interventions in maintaining normothermia during the operation. In previous studies, it has been reported that hypothermia has developed from the 30th minute of surgery (Balki et al., 2020; Zhang et al., 2018) in patients who have not been warmed during general anesthesia, whereas normothermia has been maintained (Choi et al., 2016; Kang and Park, 2020; Pan et al., 2015; Pu et al., 2014; Zhang et al., 2018) in patients who have been warmed, and our findings confirmed the results of previous studies.
Among active heating methods, forced-air warming is the most effective (Burlingame and Conner, 2018). In a Cochrane review, it was found that adult patients undergoing abdominal surgery under general anesthesia had a beneficial effect in terms of surgical site infection and complications, cardiovascular complication rates in patients who were warmed with air blown heating before or during the surgery, or in both periods, compared with patients who did not use any active warming method. It has been shown to reduce shivering and increase the thermal comfort of patients (Madrid et al., 2016).
Another method recommended for the prevention of intraoperative hypothermia is the administration of heated fluids (Campbell et al., 2015; Hooper et al., 2009; Madrid et al., 2016; Riley and Andrzejowski, 2018). In another Cochrane review, it was concluded that the administration of intraoperatively heated IV and/or irrigation fluids had a beneficial effect on postoperative body temperature and shivering levels, but the clinical significance of this benefit was unclear and was a result of using this method in addition to other active warming methods. A national guide also reported that intraoperative heated fluids alone are not effective (Campbell et al., 2015).
A national guideline reported that intraoperative warmed fluids alone were not effective (TARD, 2013). To resolve this discrepancy, in this study, we applied active heating methods such as fluid warmers and forced-air warming systems alone and in combination during surgery. To resolve this discrepancy, in this study, we applied active heating methods such as fluid warmers and forced-air warming systems alone and in combination during surgery. In this study, we determined that intraoperative and postoperative normothermia was maintained in the group that received heated IV and irrigation fluids alone as well as in the group that was heated with a forced-air warming system alone. This finding provided evidence for the effect of intraoperative administration of warmed IV and/or irrigation fluids alone in preventing perioperative hypothermia.
Nevertheless, we observed that the group with combined warming had the highest body temperature after 60 minutes of surgery. Consistent with our findings, previous studies in which various intraoperative active heating methods have been applied alone and in combination have also reported that combined heating has been more effective (Ayhan et al., 2018; Zhang et al., 2018). These findings are a result of the synergistic effect of multiple heat sources.
Since general anesthesia may result in prolonged operative time, prolonged exposure of surgical sites to the cold environment, and may involve the use of various anesthetics such as regional or spinal anesthesia (Kang and Park, 2020), a combination of active heating methods is necessary to maintain intraoperative normothermia. In clinical practice, there are concerns that the use of forced-air warming systems may cause surgical site infection, but a meta-analysis reported that active heating of the body surface reduced surgical site infection (Balki et al., 2020).
In this study, none of the patients in the combined heating group had shivering at any time point in the postoperative period, whereas shivering was observed in one patient who was heated with the forced-air warming system alone, in two patients who were given heated fluids alone, and in 15 patients in the control group. Moreover, the rate and severity of shivering up to the 1st hour after admission to the surgical clinic were significantly higher in the control group. This result is consistent with previous study results, showing that the prevalence of postoperative shivering has decreased in patients who have been warmed during the surgery using various active heating methods such as forced-air warming and liquid heating devices (Ayhan et al., 2018; Kang and Park, 2020; Pu et al., 2014; Su and Nieh, 2018; Zhang et al., 2018).
Shivering is involuntary muscle movement to increase body temperature in response to cold (Bilgin, 2017). Postanesthesia shivering is associated with oxygen consumption, carbon dioxide production, cardiac output, increased metabolic rate, and hypertension (Bindu et al., 2017). Moreover, shivering during the awakening and recovery period is the most uncomfortable experience for patients in the postoperative period (Bilgin, 2017). Therefore, patients benefit more from combined heating in the prevention of postoperative shivering.
On the contrary, the intraoperative combined heating group had the highest body temperature, and no shivering was observed in any patient, which increased thermal comfort. In the study, although the thermal comfort of all three groups was significantly higher up to the 3rd hour after admission to the surgical clinic compared with the control group, the combined warmed group had the highest thermal comfort.
This finding is consistent with the results of the study, which reported that patients who were not heated compared with patients who were heated had significantly lower thermal comfort in the PACU (Cobb et al., 2016; Kang and Park, 2020; Lee et al., 2018; Nieh and Su, 2018; Santa Maria et al., 2017; Torossian et al., 2015) and up to 2nd hour after admission to the surgical clinic (Kurz et al., 1995). These results suggest that intraoperative combined heating provides physical benefits such as providing optimum body temperature and preventing shivering, as well as psychological comfort such as increasing thermal comfort by preventing involuntary muscle movements.
In the literature, it has been suggested that 15% of the shivering response caused by perioperative hypothermia is related to pain, and that postoperative shivering may also increase pain intensity (Lopez, 2018; Ma et al., 2017). However, there are studies (Kim et al., 2009) reporting that there is no difference in postoperative pain intensity between patients who have been warmed with various heating methods at different time points in the perioperative period and patients who have not been warmed.
In addition, there are studies reporting that the pain intensity of warmed patients has been significantly lower (Ma et al., 2017; Su and Nieh, 2018). Consistent with this study's findings, Kim et al. (2009) found that postoperative pain intensity was similar in patients who were actively heated during arthroscopic shoulder surgery and those who were not. This may be a consequence of the shorter incision width and shorter duration of surgery due to the type of surgical intervention and, thus, milder surgical trauma.
Moreover, in studies involving patients who underwent bilateral hip replacement (Ma et al., 2017) and laparoscopic thoracic and abdominal surgery (Su and Nieh, 2018), the lower postoperative pain intensity of heated patients may have been due to the long duration of surgery (3 hours), regardless of the type of surgery. Furthermore, postoperative pain intensity has been associated with major surgical interventions and prolonged surgical interventions (Coppes et al., 2020).
Similar controversies exist for postoperative nausea and vomiting, another common and unpleasant complication in adult patients undergoing surgery under general anesthesia that nurses have to deal with. Consistent with this study findings, studies reporting that there was no difference in postoperative nausea and vomiting between patients who were warmed with active heating methods during surgery and those who were not (Ayhan et al., 2018; Chung et al., 2012; Kurz et al., 1996; Ma et al., 2017), there are studies reporting that the incidence of nausea was significantly lower (intervention group 33.3%, control group 60%) and the incidence of vomiting decreased, although not significantly (intervention group 26.7%, control group 33.3%) (Aydın et al., 2019).
The fact that there was no significant difference between the groups in terms of postoperative nausea and vomiting in our study may result from a similar postoperative pain intensity and the type of analgesic administered. The intensity of postoperative pain and the type of analgesic used in its treatment affect postoperative nausea and vomiting (Reisli et al., 2021). In randomized controlled studies investigating the efficacy of similar heating methods as in this study (Aydın et al., 2019; Ayhan et al., 2018; Kim et al., 2009; Su and Nieh, 2018), it has been seen that the relationship between involuntary hypothermia and postoperative pain, nausea and vomiting is not clear. This may be a result of differences in the type of surgical intervention, analgesic and antiemetic management of the patients in the sample of the studies. Future comprehensive studies are needed to clarify the relationship between perioperative hypothermia and postoperative pain, nausea and vomiting.
Limitations
A limitation of this study is that only the effect of some active warming methods during surgery was examined.
Recommendations for Clinical Practice
For surgical interventions under general anesthesia lasting >30 minutes, it is recommended to use intraoperative active warming methods, and for surgical interventions lasting longer than one hour, it is recommended to warm the patients using heated IV and/or irrigation fluids in combination with a hot forced-air warming system. It is also recommended that comprehensive studies focusing on the effect of intraoperative active warming methods on postoperative pain, nausea and vomiting be conducted.
Conclusion
The findings of this study showed that normothermia was achieved in the first 24 hours postoperatively in the groups that were both heated with a forced-air warming system and in which heated IV and/or irrigation fluids were administered, and that the group with both methods together had the best body temperature from the 60th minute of surgery. Furthermore, the study findings showed that intraoperative alone and combined interventions improved patients' postoperative thermal comfort and reduced shivering, but did not affect pain intensity, nausea and vomiting levels, and analgesic and antiemetic requirements.
Footnotes
Acknowledgment
We thank Prof. Dr. Ahmet Sebe and Prof. Dr. Ferit Çiçekçioğlu, who assisted us in the supply of devices, operating room, surgical clinic nurses, and doctors, as well as for their support in providing information and guidance.
Authors' Contribution
O.S.A. and A.G. contributed to study conception and design, analysis and interpretation of data, acquisition of data, and drafting of the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.