
Abstract
Body temperature (BT) has been utilized to assess patient outcomes across various diseases. However, the impact of BT on mortality in the intensive care unit (ICU) among patients with congestive heart failure (CHF) and diabetes mellitus (DM) remains unclear. We conducted a retrospective cohort study using data from the Medical Information Mart for Intensive Care (MIMIC)-IV data set. The primary outcome assessed was in-hospital mortality rates. BT was treated as a categorical variable in the analyses. The association between BT on ICU admission and in-hospital mortality was examined using multivariable logistic regression models, restricted cubic spline, and subgroup analysis. The cohort comprised 7063 patients with both DM and CHF (3135 females and 3928 males), with an average age of 71.5 ± 12.2 years. Comparative analysis of the reference group (Q4) revealed increased in-hospital mortality in Q6 and Q1 temperature groups, with fully adjusted odds ratios of 2.08 (95% confidence interval [CI]: 1.45–2.96) and 1.95 (95% CI: 1.35–2.79), respectively. Restricted cubic spline analysis demonstrated a U-shaped relationship between temperature on admission and mortality risk (p nonlinearity <0.001), with the nadir of risk observed at 36.8°C. The effect sizes and corresponding CIs below and above the threshold were 0.581 (95% CI: 0.434–0.777) and 1.674 (95% CI: 1.204–2.328), respectively. Stratified analyses further validated the robustness of this correlation. Our study establishes a nonlinear association between BT and in-hospital mortality in patients with both CHF and DM, with optimal suitable BT at 36.8°C. Further research is necessary to confirm this relationship.
Introduction
Diabetes mellitus (DM) is a metabolic disorder characterized by chronic hyperglycemia and disturbances in carbohydrate, fat, and protein metabolism due to insufficient insulin secretion (Lee et al., 2019). The prevalence of diabetes is expected to rise significantly, with projections estimating 578 million adults with diabetes by 2030 and 700 million by 2045(Wang et al., 2022). Back in 1974, the Framingham studies highlighted a notable twofold to fivefold increase in the risk of heart failure (HF) among patients with diabetes (Kannel et al., 1974). Moreover, diabetic patients had higher rates of mortality and hospitalization from HF compared with nondiabetic patients (Aguilar et al., 2004; MacDonald et al., 2008; Pfeffer et al., 1992; Solomon et al., 2002). Despite the growing recognition of HF as a frequent and potentially fatal complication of diabetes, the exact factors linking DM and congestive heart failure (CHF) remain poorly understood (Bell, 2003).
Body temperature (BT) is a vital sign frequently measured in clinical settings, and it has been utilized to assess outcomes in patients with various conditions, including sepsis (Baek et al., 2022), trauma (Okada et al., 2022), and multiorgan failure (Whittle and Bates, 1979). Its significance in evaluating critically ill patients and guiding patient assessment and management has led to a growing focus on BT in recent years (Laupland, 2009; O'Grady et al., 2008). For instance, studies have demonstrated that lower BT in frail older emergency department patients is linked to significantly higher 30- and 90-day mortality (Alakare et al., 2022). Similarly, in adult trauma patients, both hypothermia and hyperthermia at hospital admission have been associated with increased in-hospital mortality (Okada et al., 2022). Moreover, research has shown that hypothermia in patients with sepsis is linked to in-hospital mortality, particularly in the normal body mass index group (Ito et al., 2022).
Despite the strong correlation between diabetes and HF, limited studies have explored the connection between BT levels among individuals with DM during hospitalization for CHF and their outcomes. Therefore, this study aims to investigate the association between BT and in-hospital mortality in a substantial cohort of American adults with both CHF and diabetes who are admitted to the intensive care unit (ICU).
Methods
Data source
This was a retrospective observational study using data from the Medical Information Mart for Intensive Care IV (MIMIC-IV) (Chen et al., 2019), an international database created as a collaboration between the Beth Israel Deaconess Medical Center and the Laboratory for Computational Physiology at the Massachusetts Institute of Technology (Wong et al., 2021). MIMIC contains a wide range of patient information, including demographics, hourly vital signs, laboratory test results, International Classification of Diseases and Ninth Revision (ICD-9) codes diagnoses, and other clinical characteristics (Luo et al., 2022). Before accessing the data, the first author (K.Z.) completed the “Protecting Human Research Participants” training course on the National Institutes of Health (NIH) website and received approval for research purposes (certification number: 11639604).
Approval for the establishment of the MIMIC database was obtained from the Institutional Review Boards of both the Beth Israel Deaconess Medical Center and the Massachusetts Institute of Technology (Yang et al., 2021). As all patient records in the MIMIC-Ⅳ database were anonymous, the Institutional Review Committee of Beth Israel Deaconess Medical Center waived the requirement for individual patient consent (Hou et al., 2022). The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Study population
Participants eligible for the study were patients with CHF who experienced diabetes (DM) for the first time during their ICU admission. The diagnosis of CHF was established using the International Classification of Diseases, Ninth Revision (ICD-9) code 4280. Data from their initial ICU admission were considered for patients with multiple ICU admissions. In the MIMIC IV database, a total of 16012 patients with CHF were initially included in the study. Exclusions were made for individuals younger than 18 years (n = 12), those without diabetes (n = 8920), and those with missing outcome data (n = 17). Ultimately, a total of 7063 participants met the eligibility criteria and were included in the study. The selection process and search strategy are illustrated in detail in Figure 1, which provides a flowchart of the study.
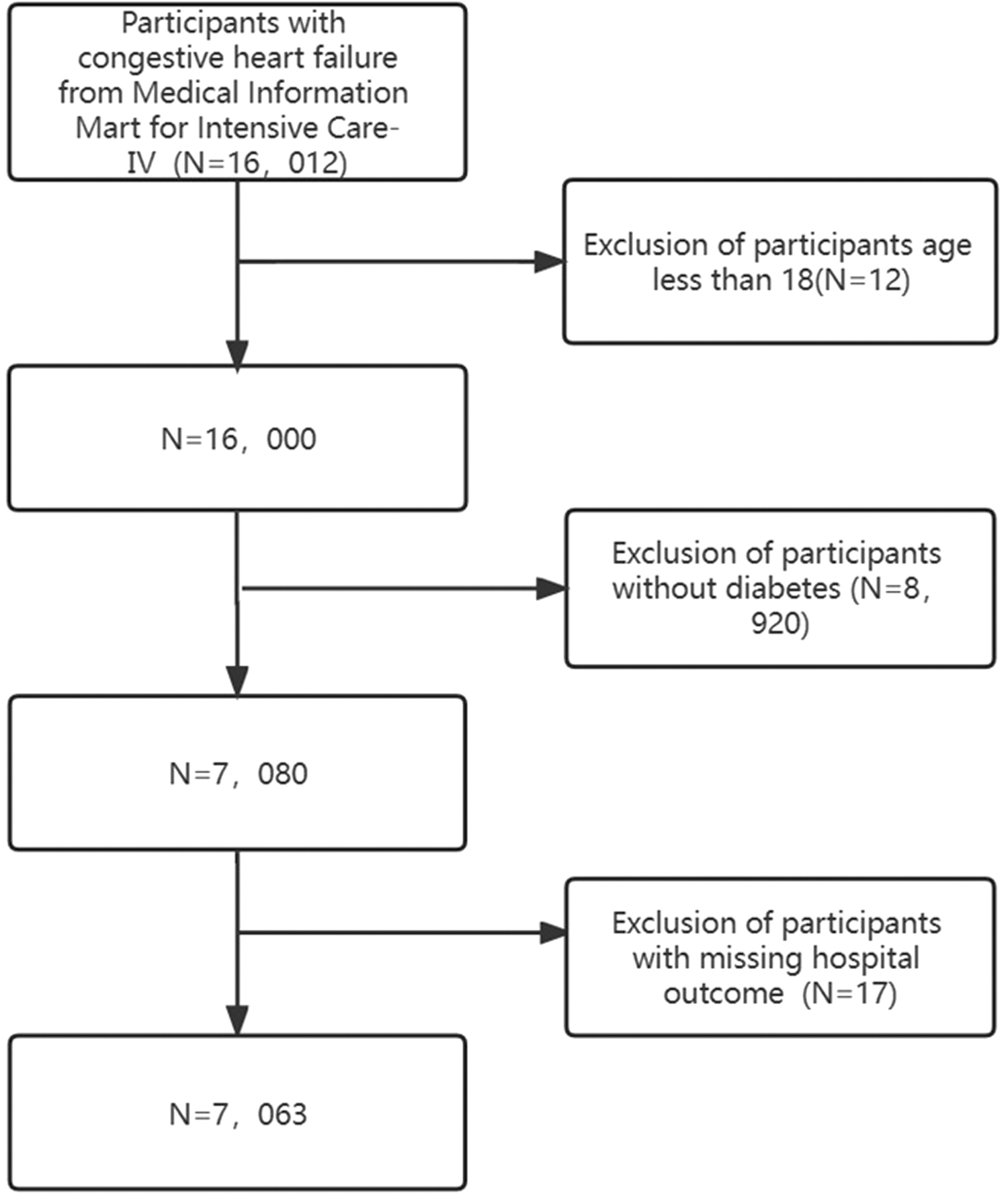
Flowchart of patient selection.
Data retrieval and outcomes
The study utilized the Structured Query Language (SQL) for data extraction. Within 24 hours of admission to the ICU, we collected various data points, including vital signs (heart rate, respiratory rate, systolic blood pressure [SBP]), the Sequential Organ Failure Assessment (SOFA) score, and the Simplified Acute Physiology Score II (SAPS II). In addition, demographic information such as age, race, and sex, as well as the severity of illness at ICU admission assessed by the SOFA score and SAPS II, was recorded. Treatment details, such as the use of ventilation and vasoactive drugs (norepinephrine, dopamine, epinephrine, phenylephrine, and vasopressin), along with medical procedures such as ventilation and intubation, were also documented. Comorbidities such as chronic obstructive pulmonary disease (COPD), hepatic failure (Hep F), and acute myocardial infarction (AMI) were noted.
Laboratory test indexes on admission included anion gap (AG), chloride, blood urea nitrogen (BUN), calcium, creatinine, potassium, sodium, mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), mean corpuscular volume (MCV), platelet count, hemoglobin, red blood cell distribution width (RDW), red blood cell count (RBC), and white cell count (WCC). Demographic characteristics and vital signs within the first 24 hours of admission were recorded, with the initial measurement upon admission serving as the laboratory examination indicators. The aim of the study was to extract the same variables as those present in the MIMIC-IV data set. The primary outcome measured was in-hospital mortality, determined by the patient's survival status at discharge.
Statistical analyses
The data were classified into two types: continuous and categorical variables. Continuous variables were categorized based on their normality distribution. Normally distributed continuous variables were presented as mean ± standard deviation and compared using Student's t-test, while non-normally distributed variables were presented as median ± interquartile range (IQR) and compared using the Wilcoxon rank-sum test. Categorical variables were expressed as percentages and compared using the chi-square test. The significance of differences among groups stratified by BT was assessed using the Kruskal–Wallis test or one-way analysis of variance.
To examine the association between BT and in-hospital mortality, multivariate logistic regression was performed. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to evaluate this relationship. Several models were used for adjustment, progressively adding covariates: Model 1 (crude model with no adjusted covariates), Model 2 (including demographic variables: sex, age, race), Model 3 (adding demographic variables and concomitant diseases: COPD, AMI, MC, HepF), Model 4 (further including demographic variables, complicating diseases, medical procedures: vent, intubated, medication situation: norepinephrine, dopamine, epinephrine, phenylephrine, vasopressin, as well as basic vital signs: respiratory rate, heart rate, SBP, and blood biochemical indicators: AG, BUN, chloride, creatinine, Hb, MCH, MCHC, MCV, platelet, potassium, sodium, RBC, RDW, WBC), and Model 5 (adjusted for demographic variables, complicating diseases, medical procedures, medication situation, basic vital signs, blood biochemical indicators, APSIII, SOFA). Logistic regression with BT categorized into six groups was used to test for trends.
A generalized additive model and a smooth curve fitting technique (penalized spline method) were used to examine potential nonlinear relationships between BT and in-hospital mortality. Stratified linear regression models and likelihood ratio tests were applied to identify modifications and interactions in subgroups based on various factors.
All analyses were conducted using the statistical software packages R, version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria), and Free Statistics software, version 1.7. A significance level of p < 0.05 (two-sided) was considered statistically significant. The reporting of this cross-sectional study adhered to the STROBE statement.
Results
Baseline characteristics of selected participants
Table 1 presents baseline characteristics of 7063 patients with concurrent diabetes and CHF, categorized into six groups based on their temperature: Q1 (≤36.3°C), Q2 (36.3–36.5°C), Q3 (36.5–36.7°C), Q4 (36.7–36.9°C), Q5 (36.9–37.1°C), and Q6 (≥37.1°C). The entire patient cohort had a mean age of 71.5 ± 12.2 years. Differences in age, race, norepinephrine, dopamine, epinephrine, phenylephrine, vent intubated, COPD, AMI, MC, AG, BUN, calcium, chloride, creatinine, Hb, MCH, MCHC, MCV, platelet, potassium, sodium, RBC, RDW, WBC, SOFA, APSIII, and Hstatus among the six temperature groups were statistically significant (p < 0.05).
Characteristics of the Study Population (N = 7063)
Q1 (≤36.3°C), Q2 (36.3–36.5°C), Q3 (36.5–36.7°C), Q4 (36.7–36.9°C), Q5 (36.9–37.1°C), and Q6 (≥37.1°C).
%, weighted proportion; AG, anion gap; AMI, acute myocardial infarction; APSIII, Acute Physiology III; BUN, blood urea nitrogen; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HepF, hepatic failure; Hstatus, hospital status; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; RBC, red blood cell count; RDW, red blood cell distribution width; SOFA, Sequential Organ Failure Assessment; WBC, white blood cell count.
p Values of multiple comparisons were corrected by the false discovery rate method.
Q1–Q6: according to temperature.
Association between temperature and in-hospital mortality
Table 2 illustrates the relationship between BT and in-hospital mortality in patients with CHF and diabetes. The study examined ORs and their corresponding 95% CIs for various BT ranges, as well as the risk of in-hospital mortality in CHF and diabetes patients. The analysis accounted for pertinent demographic variables (sex, age, race), concurrent medical conditions (COPD, AMI, MC, diabetes, HepF), medical procedures (vent, intubated), medication usage (norepinephrine, dopamine, epinephrine, phenylephrine, vasopressin), essential vital signs (respiratory rate, heart rate, SBP), blood biochemical indicators (AG, BUN, chloride, creatinine, Hb, MCH, MCHC, MCV, platelet, potassium, sodium, RBC, RDW, WBC), APSIII, and SOFA scores.
Multivariable Logistic Regression to Assess the Association of Temperature with In-Hospital Mortality Rate
Model 1: No adjustment.
Model 2: Adjusted for demographic variables (sex, age, race).
Model 3: Adjusted for demographic variables, concomitant disease (COPD, AMI, MC, HepF).
Model 4: Adjusted for demographic variables, complicating disease, medical procedures (vent, intubated), vital signs (heart rate, respiratory rate, SBP), medication situation (norepinephrine, dopamine, epinephrine, phenylephrine, vasopressin), blood biochemical indicators (AG, BUN, chloride, creatinine, Hb, MCH, MCHC, MCV, platelet, potassium, sodium, RBC, RDW, WBC).
Model 5: Adjusted for demographic variables, complicating disease, medical procedures, vital signs, medication situation, blood biochemical indicators, APS III, SOFA
The unit of temperature is °C, %, weighted proportion; AG, anion gap; AMI, acute myocardial infarction; APSIII, Acute Physiology III; BUN, blood urea nitrogen; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HepF, hepatic failure; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; RBC, red blood cell count; RDW, red blood cell distribution width; SBP, systolic blood pressure; SOFA, Sequential Organ Failure Assessment; WBC, white blood cell count; CI, confidence interval; OR, odds ratios; Ref, reference.
Both low and high BTs were associated with a higher risk of mortality compared with the reference group, even after adjusting for the aforementioned factors. Specifically, in comparison with the reference group, the ORs and 95% CIs for each of the BT six groups were as follows: (Q1: OR = 1.95, 95% CI 1.35–2.79, p < 0.001; Q2: OR = 1.46, 95% CI 0.99–2.14, p = 0.054; Q3: OR = 1.44, 95% CI 1.01–2.04, p = 0.043; Q4: reference; Q5: OR = 1.3, 95% CI 0.91–1.86, p = 0.153; Q6: OR = 2.08, 95% CI 1.45–2.96, p < 0.001). These associations were consistent across all the five statistical models (Table 2).
Dose–response relationships
The present study establishes a nonlinear association between BT and in-hospital mortality in patients diagnosed with CHF and diabetes, while controlling for potential confounding variables (see Fig. 2). Specifically, a negative correlation exists between BT and the risk of in-hospital mortality until reaching a threshold of 36.8°C (OR = 0.581 [95% CI 0.434–0.777], p < 0.001). Beyond this threshold, exceeding 36.8°C, the risk of in-hospital mortality significantly increases (OR = 1.674 [95% CI 1.204–2.328], p = 0.0022) (refer to Table 3).

Dose–response relationships between temperature and in-hospital mortality rate OR. Solid and dashed lines represent the predicted value and 95% CIs. Adjusted for demographic variables (sex, age, race), concomitant disease (COPD, AMI, MC, HepF), vital signs (heart rate, respiratory rate, SBP), medical procedures (vent, intubated), medication situation (norepinephrine, dopamine, epinephrine, phenylephrine, vasopressin), blood biochemical indicators (AG, BUN, chloride, creatinine, Hb, MCH, MCHC, MCV, platelet, potassium, sodium, RBC, RDW, WBC), APSIII, SOFA. Only 99% of the data are shown. %, weighted proportion; AG, anion gap; AMI, acute myocardial infarction; APSIII, Acute Physiology III; BUN, blood urea nitrogen; CHF, congestive heart failure; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HepF, hepatic failure; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; OR, odds ratios; RBC, red blood cell count; RDW, red blood cell distribution width; SBP, systolic blood pressure; SOFA, Sequential Organ Failure Assessment; Ref, reference; WBC, white blood cell count.
Threshold Effect Analysis of Relationship of Temperature with In-Hospital Mortality Rate
Adjusted for demographic variables (sex, age, race), concomitant disease (COPD, AMI, MC, HepF), medical procedures (vent, intubated), vital signs (heart rate, respiratory rate, SBP), medication situation (norepinephrine, dopamine, epinephrine, phenylephrine, vasopressin), blood biochemical indicators (AG, BUN, chloride, creatinine, Hb, MCH, MCHC, MCV, platelet, potassium, sodium, RBC, RDW, WBC), APSIII, SOFA.
%, weighted proportion; AG, anion gap; AMI, acute myocardial infarction; APSIII, Acute Physiology III; BUN, blood urea nitrogen; CHF, congestive heart failure; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HepF, hepatic failure; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; OR, odds ratios; RBC, red blood cell count; RDW, red blood cell distribution width; Ref, reference; SBP, systolic blood pressure; SOFA, Sequential Organ Failure Assessment; WBC, white blood cell count.
Subgroup analysis
In this study, we conducted subgroup analyses to examine the influence of different factors on the association between BT and in-hospital mortality. Variables such as age, sex, race, and Hep F were used for stratification. The results of these subgroup analyses, including their interactions, are provided in Supplementary Figure S1. Notably, no statistically significant associations were observed in any of the subgroups (p > 0.05).
Discussion
BT is a crucial physiological indicator of the human body, and maintaining a normal BT is indispensable for the regulation of normal life activities (Bindu et al., 2017). In this retrospective cohort study, a significant correlation between BT and mortality risk was observed in patients diagnosed with CHF and diabetes. Both hypo- and hyperthermia demonstrated statistically significant associations with increased mortality compared with the middle reference group. This relationship remained significant even after controlling for potential confounding factors, indicating an independent nonlinear association between BT and mortality in patients with CHF and diabetes. Moreover, stratified analyses consistently underscored the robustness of the association between BT and in-hospital mortality.
Numerous prior studies have addressed the influence of BT on in-hospital mortality risk, particularly in adult patients with trauma. Consistent with our findings, Wade et al. (2011) demonstrated that both hypothermia and hyperthermia upon hospital admission were linked to higher in-hospital mortality. Similarly, Saxena et al. (2015) reported increased risk of death for patients with stroke and traumatic brain injury experiencing peak temperatures below 37°C or above 39°C compared with those with normal BT. Moreover, Casscells et al. (2005) identified a significant association between hypothermia at hospital arrival and elevated in-hospital mortality in a retrospective study involving 291 HF hospitalized patients for HF exacerbation.
Nevertheless, some studies have presented differing results. For instance, a previous study found that hypothermia appeared more detrimental than hyperthermia as it was associated with increased 1-year mortality (Erkens et al., 2020). In addition, hypothermia was linked to notably higher mortality rates in patients with worsening HF (Payvar et al., 2013), frailty in older adults in the emergency department (Alakare et al., 2022), and after coronary artery bypass grafting (Hannan et al., 2010). It is worth noting that the subjects in these prior studies were primarily patients with other ailments, and only limited investigations have simultaneously explored both CHF and DM. In our study, we discovered that both low and high BTs were associated with a heightened risk of mortality when compared with the reference group, even after adjusting for the aforementioned factors.
This study deviates from previous investigations by utilizing smooth curve fitting and generalized additive models to explore the nonlinear relationship between BT and in-hospital mortality in patients with CHF and diabetes. Subsequently, subgroup analysis was conducted to ensure the consistency of the primary findings. The results reveal a nonlinear association between BT and in-hospital mortality in individuals with HF and diabetes, characterized by a critical point at 36.8°C. While an increase in BT is linked to a decreased risk of in-hospital mortality, a significant elevation in risk is observed among subjects with a BT of 36.8°C or higher, indicating a further decline in outcomes. These findings highlight the importance of considering both hypothermia and hyperthermia in clinical practice.
Plausible explanations for the heightened mortality risk associated with BT are evident, despite an incomplete understanding of the precise underlying mechanism. It has been observed that immune cells exhibit optimal functioning at ∼36.8°C, and deviations from this temperature range, either higher or lower, can result in decreased immunity, thereby leading to infection and an increased risk of death in patients (Los et al., 2022). Another factor contributing to the increased mortality risk can be attributed to the molecular mechanism of oxyhemoglobin.
Previous studies examining conditions other than CHF indicate that addressing hypothermia could potentially mitigate complications such as metabolic acidosis and arrhythmias (Astrup et al., 1965). This is due to the negative impact of alterations in temperature and pH on the dissociation curve of oxyhemoglobin in human blood (Astrup et al., 1965). In addition, hypothermia-induced shivering may further strain the heart, necessitating augmented cardiac output to supply the involved muscles (Brengelmann, 1996).
Our study offers several notable strengths. First, it is the pioneering investigation into the relationship between BT and in-hospital mortality in patients with CHF and diabetes admitted to the ICU, focusing on a previously unexplored area. The findings of our study reveal a nonlinear association between BT and in-hospital mortality, providing a solid theoretical basis for establishing targeted strategies for BT control in these patients. In addition, the broad applicability of our conclusions to various clinical scenarios further reinforces their significance. To ensure robustness, we addressed confounding factors through the use of logistic regression analysis with multiple models and conducted relevant subgroup analyses.
Despite these strengths, we must acknowledge the limitations of our study. Due to its retrospective nature, inherent biases may be present, even with our efforts to adjust for relevant variables to ensure result accuracy. While we chose BT as the parameter of interest for its ease of measurement and clinical convenience, we recognize that there may be other relevant factors worth considering. Furthermore, our study only considered the first BT measurement after ICU admission, without tracking its dynamics over time. Nevertheless, this initial measurement may better reflect the BT at the beginning of hospitalization. However, it is essential to be cautious when applying our study's results to other nations or ICU institutions since the research was conducted in a single ICU facility in the United States.
Despite this limitation, the substantial and representative sample size enhances the reliability of our findings. For future validation and broader applicability, we recommend conducting multicenter prospective studies.
Conclusions
A nonlinear association between BT and in-hospital mortality is observed in patients with DM and CHF, with an optimal BT of 36.8°C. This study derives its clinical significance from analyzing data from MIMIC to assess the relationship between BT and in-hospital mortality. The findings not only add to the current literature but also provide potential insights into the underlying pathogenesis of this association. To enhance the validity and coherence of these results, future research should consider using prospective, randomized controlled study designs.
Footnotes
Acknowledgment
We appreciate Dr. Jie Liu of the Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital, for statistics, study design consultations, and editing the article.
Authors' Contributions
K.Z. contributed as the first author of this article. Y.H., F.M.G., J.Y.L., and J.Y.Z. were responsible for the concept and design of the study. Z.Z.G., J.G.C., B.W.C., and M.G. explained the analysis. Z.Y.H., X.Y.Q., T.Y.C., Y.F.G., J.Y.X., R.H., and T.L.Z. are responsible for data recovery. K.Z., T.Z.L., and B.L. are the primary corresponding authors. All the authors critically revised the important intellectual content of the article and approved the final draft.
Ethics Approval and Consent to Participate
The establishment of this database was approved by the Massachusetts Institute of Technology (Cambridge, MA, USA) and Beth Israel Deaconess Medical Center (Boston, MA, USA), and informed consents were exempted due to all patients' data being anonymized before the data were obtained. We also complied with all the relevant ethical regulations regarding the use of data in our study. All reports adhered to the guidelines for Strengthening the Reporting of Observational Studies in Epidemiology and the Declaration of Helsinki.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.