
Abstract
Cancer treatment often involves excisional surgery, but this approach may leave behind minimal residual disease, leading to tumor regrowth. Proinflammatory cytokines and their role in altering residual cancerous cells postsurgery have garnered attention. The study examines how mild intraoperative cooling affects cancer cells and their gene expression. It aims to discover strategies for reducing tumor growth after surgery. Nine cases of solid tumor were included in the study, nine samples were cooled with the Peltier–Seebeck device down to12°C, and cooled and noncooled regions of tumors were analyzed using reverse transcription-polymerase chain reaction. Key transcriptomes, including neural-cadherin, cadherins (CDH), 70-kDa Heat Shock Protein (HSP70), hypoxia-inducible factor (HIF), Y-Box-binding protein 1 (YB-1), matrix metalloproteinase 9 (MMP9), and matrix metalloproteinase 2 (MMP2), were measured to assess the impact of mild hypothermia on cancer cell metabolism and cold shock responses. Analysis of cooled and noncooled regions revealed reduced MMP2/9 levels in cooled regions in five out of seven cases, indicating potential suppression of tumor invasion and metastasis. CDH-1 expression was detected in five cases, with decreased levels observed in cooled regions in most cases, suggesting a role in tumor aggressiveness. YB-1 expression was increased in six out of eight samples, possibly correlating with local recurrence and reduced overall survival times. N-Cad expression was increased in all five samples where it was detected, indicating its potential involvement in tumor cell motility and invasion. HSPs showed a mild increase in four out of five cases following cooling, potentially contributing to tumor cell resistance to cooling-induced apoptosis. Intraoperative mild cooling resulted in the downregulation of key proteins playing a role in invasion and metastasis. However, Elevated YB-1 and N-Cad expression limits cooling's universal application. Further research is necessary to comprehend cooling-related transcriptome changes and their impact on patient outcomes.
Introduction
Cancer, characterized by uncontrolled cell growth, encompasses a diverse group of diseases with more than 100 identified types, each classified by the affected cell types (Mitra et al., 2018). Surgical intervention plays a crucial role in the treatment of cancer patients, offering increased chances of successful treatment and overall survival rates (Van der Bij et al., 2009). Nevertheless, the exact efficacy of surgery remains uncertain. Emerging experimental and clinical evidence suggests that surgery and resulting inflammation may potentially contribute to disease recurrence by instigating changes in the target tissue and cancer cell niche, promoting migration or invasion to other sites (Chen et al., 2019).
Among the various minimally invasive clinical methods in cancer treatment, cryosurgery and hyperthermia have gained prominence (IJff et al., 2022). These methods offer the advantage of fewer side effects and repeatability. Cryosurgery finds wide application in treating cutaneous and organ malignancies, while hyperthermia proves beneficial across different stages of cancer. However, the effects of hyperthermia on cancer are complex and influenced by factors such as tissue type, heat distribution, and heat sensitivity. Oncological surgery, though vital, can potentially lead to malignancy recurrence due to induced inflammation and abnormalities in the target tissue and cancer cells (Baust et al., 2014).
Cryosurgery employs extremely low temperatures to freeze and eliminate undesirable tissue in patients, making it a valuable option for treating cutaneous diseases such as tumors, warts, and specific skin conditions. Its minimally invasive nature, repeatability, and low side effects make it a promising treatment modality. Additionally, cryosurgery allows simultaneous treatment of multiple targets within an organ (Zimmerman and Crawford, 2012).
One concern associated with surgery is the potential stimulation of inflammatory cytokines, including Interleukins (IL), tumor necrosis factor Alpha (TNF α), tumor growth factor beta (TGF β), and Interferon-gamma (INF γ) (López-García and Castro-Manrreza, 2021). The presence of these cytokines in the cancerous cell niche during surgery may alter cellular phenotypes, leading to poor prognosis (Li et al., 2020). Furthermore, hypothermia has been found to lower cellular metabolism, and cooling the surgical cavity before resecting the tumor may render remaining cancerous cells more vulnerable to apoptosis, potentially reducing invasion and metastasis. Additionally, cooling may mitigate adverse interactions between inflammatory cytokines and cancerous cells (Chen et al., 2019).
Hypothermia is defined as the core body temperature reduction below 36°C. Induced hypothermia is referred to as purposely reduction the core body temperature reduction below 36°C. Therapeutic hypothermia means induced hypothermia as a medical method (Polderman and Herold, 2009).
Experimental and clinical data have pointed out hypothermia has a neuroprotective effect and its role is reported in some neurologic disease including traumatic brain injury, subarachnoid hemorrhage, stroke, intracranial pressure elevation, and spinal cord injury (Karnatovskaia et al., 2014).
However, there are some discrepancies in this regard which are probably due to the different time, temperature, and method of hypothermia (Clifton et al., 2001; Hutchison et al., 2008; Maekawa et al., 2015; Wowk et al., 2014).
There are different underlying mechanisms by reducing the metabolism of injured neurons (Schaller and Graf, 2003), reactive oxygen species, and inflammatory cytokines. However, some anti-inflammatory interleukins such as Interleukin 10 (IL10) are less produced in hypothermia (Hofstetter et al., 2007; Vitkovic et al., 2002; Yatsiv et al., 2002).
While different cooling methods are available, ranging from crushed ice in plastic bags to chemical cooling by spray, they are not always applicable within the surgical cavity. To address this limitation, our faculty's students have developed a cooling device designed to induce local hypothermia in the tumor region during surgery. This system utilizes a Peltier device, which operates based on the Peltier phenomenon, transferring heat from one side to another when an electrical current passes through it, leading to one side becoming hot and the other cold.
The Peltier module consists of two thin ceramic wafers with embedded P-type and N-type bismuth-telluride semiconductor materials. The N-type semiconductor carries an excess of electrons, while the P-type material has a deficit of electrons, resulting in a double interactive interface (Figs. 1 and 2). Depending on the direction of the current, thermoelectrics can be used for either heating or cooling. In the context of our application, cooling mode is prioritized. Utilizing a thermoelectric in the heating mode is highly efficient, as internal heating (Joulian heat) and the load from the cold side are pumped to the hot side, reducing the power required to achieve the desired temperature (Godfrey, 1996; Slanina et al., 2018).
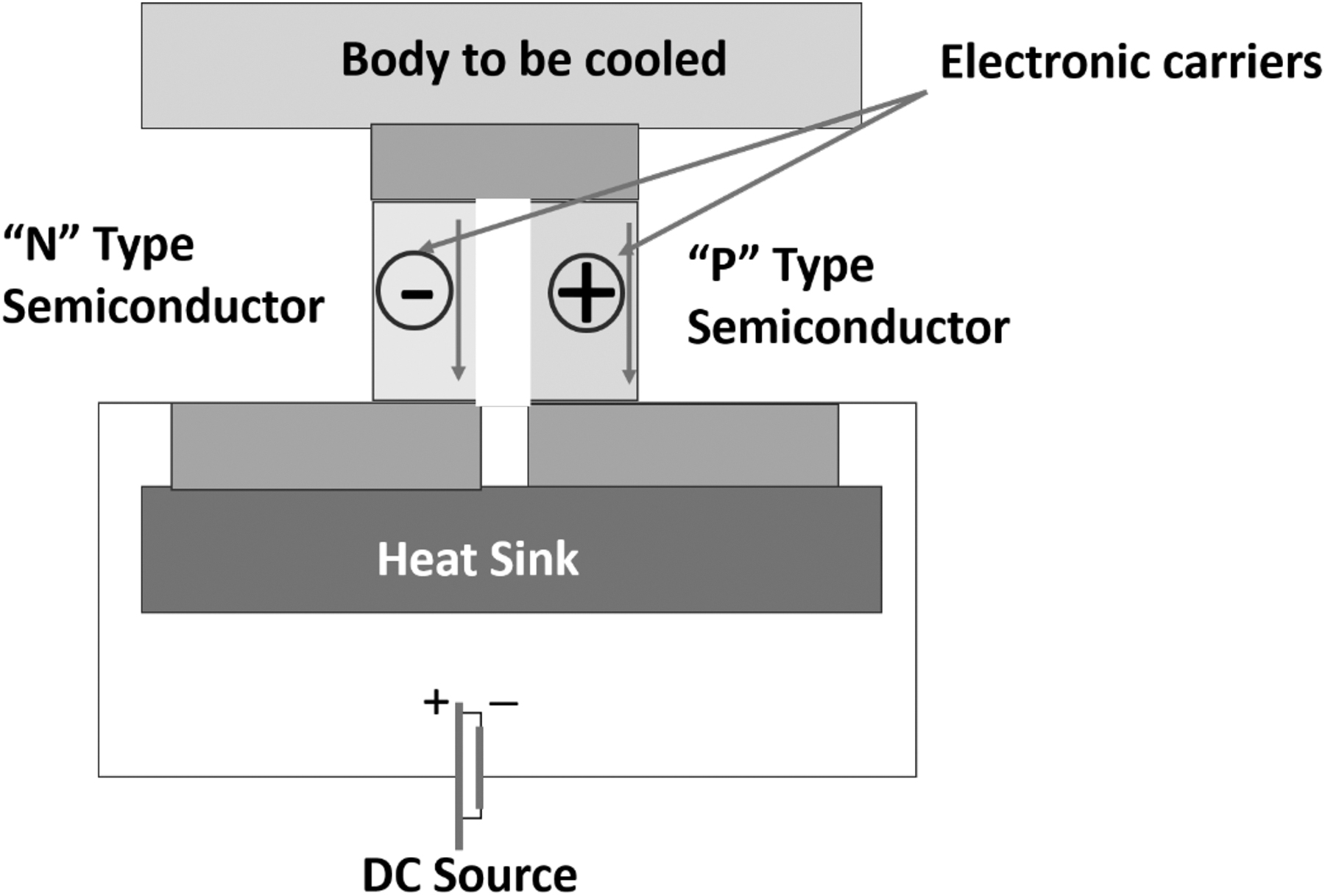
Cross section of a typical thermoelectric module.

Peltier module, extra heat sink, and electric fan help to maintain the cooled side in low temperature.
Materials and Methods
Case selection
A total of 21 cases initially participated in this study after providing informed consent, and the study received approval from the hospital's ethics committee. However, 12 cases were subsequently excluded based on the following exclusion criteria, resulting in a final cohort study of 9 cases (Fig. 3). The demographic information of the included cases is summarized in Tables 1 and 2. The inclusion criteria focused on cases with solid tumors, as the primary aim was to conduct in vitro analysis using resected tumor samples. Exclusion criteria were established for cases where tumor size precluded the delineation of cooled and noncooled regions according to the dimensions of the Peltier–Seebeck device. Cases were also excluded if surgical or anesthesia-related complications prevented the 20-minute cooling procedure or if inadequate sampling during the operation rendered the analysis inconclusive.
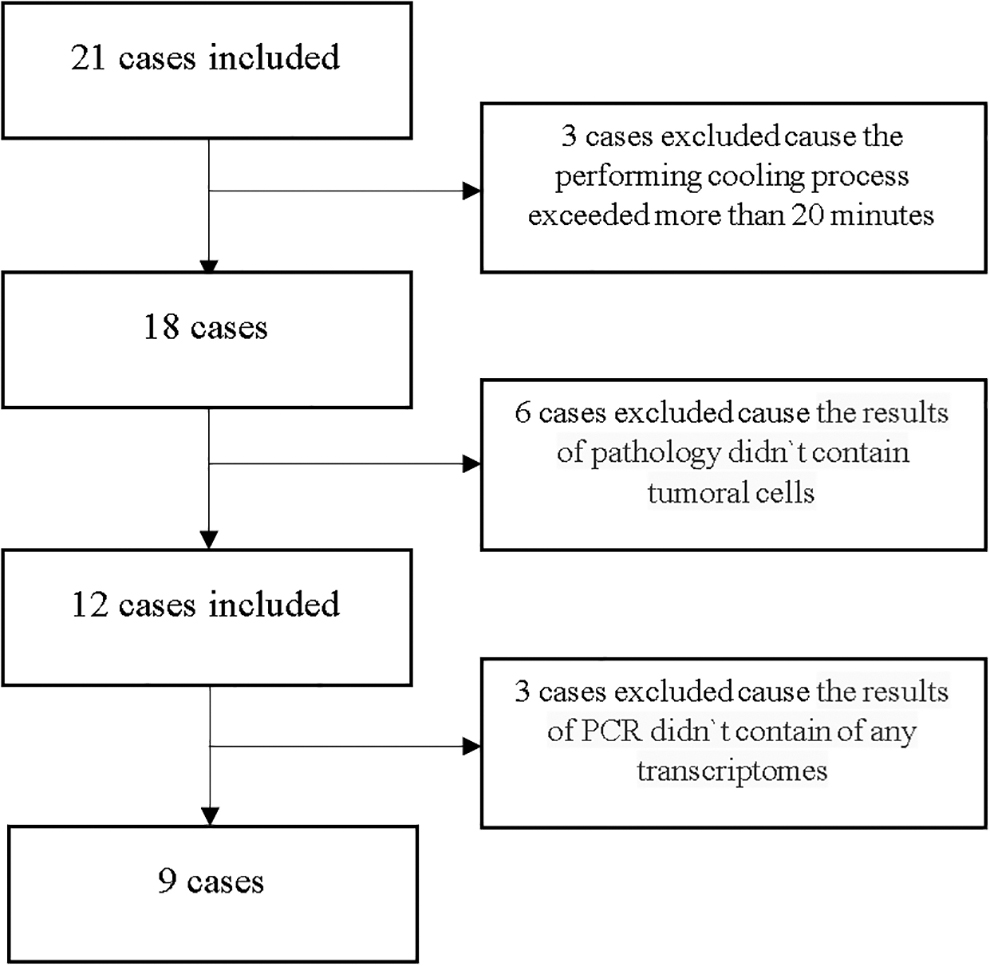
Table of exclude studies.
Baseline Characteristics
Cases` Information
+ and − indicates whether the patient received neoadjuvant or not.
+ and − indicates whether the patient had metastasis or not.
Experimental methodology
To investigate the impact of mild hypothermia on cancer cells, we adopted an approach utilizing reverse transcription-polymerase chain reaction (RT-PCR) to analyze both cooled and noncooled regions of tumors following complete dissection. The transcriptomes of neural-cadherin (NCAD), cadherins (CDH), 70-kDa heat shock protein (HSP70), hypoxia-inducible factor (HIF), matrix metalloproteinase 9 (MMP9), and matrix metalloproteinase 2 (MMP2) were assessed to explore the effects of mild hypothermia on cancer cell metabolism while minimizing cold shock responses.
Cooling procedure
For this study, large-sized tumors were selected to enable the identification of distinct cooled and noncooled regions. We utilized the Peltier–Seebeck system to achieve controlled cooling, maintaining the ambient temperature in the cooled region at ∼12°C. The cooling process was initiated immediately upon direct exposure to the tumor and lasted for ∼20 minutes. A 2 × 2 cm2 Peltier module was placed on the tumor's superficial area to facilitate cooling. The noncooled region is the farthest region from the cooled region on our tumor mass (Fig. 4).
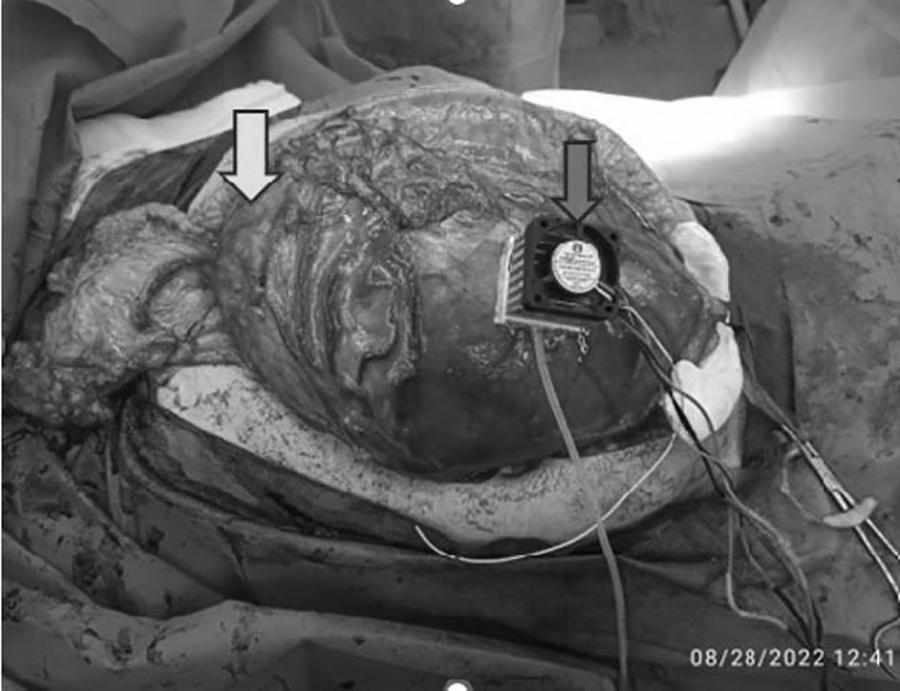
The cooling process on the tumor of a patient with a retroperitoneal tumor, right arrow shows the cooled region and left arrow mentions the noncooled region.
After the removal of vital organs from the tumor and before cutting the main blood vessels, the Peltier device was applied to the tumor for a duration of 20–25 minutes. All tumors included in the study were accessible, exhibited sufficient size, and demonstrated a homogeneous format, allowing for immediate resection after the cooling procedure. The cooled site was designated by applying the Peltier device for 20 minutes at a location distant from critical margins during surgery conducted under mild hypothermia conditions (15°C).
Tissue specimen collection
Fresh histologically normal tissue specimens were collected from the resected tumors of the nine patients (six females and three males) who underwent the cooling procedure and tumor resection at the Department of Cancer Surgery, Tehran University of Medical Sciences. Clinical-pathological data were retrospectively evaluated or collected from patient files by a surgeon and a pathologist.
RNA sequencing of the specimen
RNA
RNA samples were obtained from human breast cavity side margins, extracted from both cooled and noncooled cells. The samples were thawed and subjected to incubation at 70°C for 90 seconds. To generate cDNA, we treated the samples with a reverse transcription master mix and incubated them in a thermocycler at 50°C for 30 minutes, followed by 70°C for 15 minutes. To extract free primers, we added 1.0 μL of EXOSAP mix to each sample and incubated the mixture at 37°C for 30 minutes, subsequently inactivating it at 80°C for 25 minutes.
Next, a 3′ poly (A) tail was added to the cDNA in each sample by incubating them in the master mix at 37°C for 15 minutes, followed by inactivation at 70°C for 10 minutes. The second layer of cDNA was integrated by dividing each sample into four and incubating them in the master mix at 95°C for 3 minutes, 50°C for 2 minutes, and 72°C for 10 minutes. Subsequently, PCR amplification was performed with the master mix, consisting of an initial step at 95°C for 3 minutes, followed by 20 cycles of 95°C for 30 seconds, 67°C for 1 minute, and 72°C for 6 seconds.
After PCR amplification, the four responses from each sample were combined and filtered using the Qiagen PCR purification kit (cat. no 28106). The elution was performed in 50 μL EB buffer (cat. no 28106). MMP9, MMP2, NCad, HSP70, CDH1, YB-1, and HIF were selected for assessing in the margin samples.
The primers and probes used in the experiment (Table 3) were designed by AlleleID (Premier Biosoft) and synthesized by BonYakteh Corp. The nucleotide sequences used for the design of the probe-primers were obtained from the NCBI database. The designed probe primers were aligned using BLAS to ensure gene specificity. Similarly, each sample was divided into four, and a second round of PCR amplification was performed using a master mix consisting of nine cycles at 98°C for 3 minutes, 67°C for 1 minute, and 72°C for 6 minutes. The samples were then pooled, washed using Agencourt AMPure XP beads, and eluted in 40 μL 1 × low-TE buffer (Table 3).
For a comparative and accurate analysis of the results obtained from RT-PCR of cooled and noncooled samples, the fold cooled/noncooled was calculated.
Oligonucleotide Primer and Probe Sequences Used in the Present Study
Human.
Results
Of the initial 21 cases included, 9 cases remained in the study based on exclusion criteria. The mean age of the participants was 42.6 years (range: 20–76). The gender distribution consisted of three males (33%) and six females (66%). Three cases had undergone neoadjuvant chemotherapy (33%), and two cases presented with metastatic tumors (22.2%).
In the real-time reaction, when we compare the expression level of a gene in several groups, the best way to express the number of changes of that gene in one sample compared to another sample is fold change. The concept of fold change is the same as “how many times,” in other words, the expression of the desired gene in the samples of the first group (Cooled samples) compared to the samples of the second group (noncooled samples) increased or decreased.
Based on this, if the fold change value is more than “1,” it means that the desired gene expression is higher in cooled samples than in noncooled samples.
Based on the cooled/noncooled fold data obtained from RT-PCR, the results of the following analyses are described in detail (Table 4).
Fold Cooled/Noncooled Results
MMP, matrix metalloproteinase; CDH, cadherins; YB-1, Y-box-binding protein 1; NCAD, neural-cadherin; HSP, heat shock protein; HIF, hypoxia-inducible factor.
MMP2 expression
MMP2 expression was examined in nine cases. Out of these, MMP2 expression was detected in eight cases, ranging from 0.11 to 1.37 (C1–C6 and C8–C9). All cases with different tumors showed MMP2 expression, except for a 60-year-old male with liver metastasis originating from gastric cancer (C7). Among the detected cases, MMP2 among six cases was upregulated, while in two cases downregulated.
MMP9 expression
MMP9 expression was observed in eight out of nine cases, ranging from 0.508 to 2.46 (C1–C8). The only case without MMP9 expression was a 23-year-old male with retroperitoneal tumor and no metastasis (C9). Among the detected cases, three cases had upregulation of MMP9, while five cases had downregulation.
MMP2/9 ratio
In the cases where both MMP2 and MMP9 transcripts were expressed, the MMP2/9 ratio was calculated for seven cases, ranging from 0.15 to 1.63.
CDH1 expression
Out of the nine samples analyzed by RT-PCR, CDH1 expression was detected in five samples, ranging from 0.39 to 1.13 (C1–C3, C7–C8). Both metastatic cases (C3/C7) showed CDH1 expression, and both had levels below 1 which means the downregulation of CDH1 expression. Similarly, the three cases that had undergone neoadjuvant chemotherapy (C1, C7, C8) showed CDH1 expression, with four out of five cases having levels below one also means the downregulation of CDH1 expression. The only case with higher expression was C2, a 76-year-old woman with sigmoid colon adenocarcinoma without metastasis or neoadjuvant chemotherapy.
YB-1 expression
Among the nine samples evaluated by RT-PCR, YB-1 expression was detected in eight samples (ranging from 0.63 to 7.9). Notably, C9, the same case in which MMP-9 was not expressed, also showed no YB-1 expression. Out of the eight samples with YB-1 expression, six had higher expression (ranging from 1.14 to 7.9), while two samples had lower expression (0.63, 0.80).
NCAD expression
Among the nine cases studied, NCAD expression was detected in five samples, ranging from 1.14 to 42. All of these samples had upregulation of NCAD expression. A 34-year-old female with uterine tumor and no metastasis or neoadjuvant chemotherapy showed the highest NCAD expression level of 42 (C5). The results for C4 and C6, two cases with arm sarcoma and retroperitoneal tumor, were 7.92 and 4.96, respectively. Two cases showed expression levels slightly higher than noncooled samples: C1 (1.32) and C7 (1.34).
HSP70 expression
Among the nine cases studied, HSP70 expression was detected in five samples, ranging from 1.08 to 18.117. Out of the five samples with HSP70 expression, four showed levels in the range of 1.08 to 2.7. Only one cooled sample, a 40-year-old woman with arm sarcoma (C4), exhibited a significantly higher expression level of 18.117 compared to the other cases.
HIF expression
Out of the nine samples analyzed by RT-PCR, HIF expression was detected in four samples, ranging from 0.19 to 4.7. Among these, three cases had HIF upregulation expression (C7: 2.06, C5: 3.11, C2: 4.7), while only one case had a downregulation expression (C1: 0.19).
Discussion
Excisional surgery is a primary treatment method for cancer; however, it can lead to minimal residual disease and subsequent tumor growth. Proinflammatory cytokines, including IL-1, IL-6, and TNF-α, are implicated as probable causes of this phenomenon (Coffey et al., 2003). These cytokines increase fibrinogen production, which shields remaining tumor cells from natural killer cells (NK cells), facilitating adhesion to endothelial cells and the release of angiogenic factors (Palumbo et al., 2005; Seth et al., 2013).
MMPs play a crucial role in tumor angiogenesis, invasion, and metastasis. High expression of MMP-2 has been associated with poor survival rates and increased tumor invasion in various cancer types (Kubben et al., 2006a; Kubben et al., 2006b; Kubben et al., 2007; Sier et al., 1996). In our study, we observed varying levels of MMP2/9 expression in cooled and noncooled regions, with reduced MMP2/9 levels in cooled regions in five out of seven cases (Table 4). The prognostic significance of the MMP2/9 ratio remains controversial, with some studies showing its relevance in certain solid tumors, such as colorectal or ovarian cancer, but not as a factor for progression or invasion in others (Langers et al., 2008; Sillanpää et al., 2007).
The CDH family proteins were significantly upregulated in solid cancer tumors, leading to increased proliferation and metastasis, especially in colorectal cancer (Kim et al., 2023). In our study, CDH-1 expression was detected in five out of nine samples, with reduced levels observed in cooled samples in most cases (Table 4). The role of CDH-1 in tumor aggressiveness has been documented in other studies as well (Li et al., 2022). CDH-1 was expressed in invasive lobular carcinomas and invasive ductal carcinomas (Ribatti et al., 2020).
Y-Box-binding protein 1 (YB-1) is a member of the cold-shock domain superfamily and is involved in stimulating the entrance of epithelial cells to mesenchymal phases (Ma et al., 2018). In our study, YB-1 expression was increased in six out of eight samples, suggesting its possible correlation with local recurrence and reduced overall survival times (Yan et al., 2014).
Although some reports confirmed the overexpression of YB-1 in rectal tubular adenoma, in rectal cancer the level was decreased (Zhang et al., 2015). In breast cancer tumors YB-1 overexpression may not be an independent factor for tumor progression grades and it is in strong correlation with Her2 neu factors of the tumor, but LN involvement showed a positive correlation with YB-1 overexpression (Bansal et al., 2018). Similarly, YB-1 is expressed both in benign and malignant ovarian tumors. Moreover, no correlation was reported between YB-1 expression and the FIGO stage (Tarkowski et al., 2006).
N-Cadherin (N-Cad) expression has been associated with tumor differentiation and progression in colorectal cancer (Yan et al., 2015). In our study, N-Cad expression was increased in all five samples where it was detected (Table 4), indicating its potential role in tumor cell motility and invasion. Such role is as far strong that scientists defined N-Cad-dependent tumor metastasis in many solid tumors such as breast and ovarian cancer tumors (Assidi, 2022; Cao et al., 2019; Nieman et al., 1999). Its overexpression is also in correlation with reduced overall survival time (Assidi, 2022).
HSPs are a family of proteins that become upregulated in cancer cells in response to internal environmental stress such as lack of proteostasis or any physically or chemically changes in tumor microenvironment. These changes could be ranged from hypoxia to nutrient deprivation and acidosis (Ciocca et al., 2013). Resistance to cell death is one of the main characteristics of cancer cells in which HSP has been activated (Seclì et al., 2021). Some reports revealed that hypoxia regulates HSP70 expression by direct binding of HIF to hypoxia-responsive elements in the HSP70–2 promoter. As a result, overexpression of HSP70–2 enhanced the resistance of tumor cells to hypoxia-induced apoptosis (Huang et al., 2009).
In our study, HSP expression was evaluated in five cases, with a mild increase observed in four cases following cooling. Interestingly, one cooled sample showed significant overexpression of HSP.
The intraoperative mild cooling approach we explored in this study aimed to protect patients from the oncological side effects of tumor removal. Cooling appeared to reduce tumor invasion and local adhesion while possibly enhancing tumor cell resistance to cooling-induced apoptosis through the activation of YB-1, NCAD, HIF, and mild overexpression of HSP. Reduced invasive functions of cells may have potential benefits in preventing invasion and metastasis of remaining cellular residues from resected tumors. The activation of HSP and YB under cooling conditions may induce oxidative stress in cancer cells, contributing to their resistance to apoptosis. The observed increase in YB but not HSP in our study calls for more detailed investigations to understand the precise role of intraoperative mild cooling in activating environmental stress responses (Table 5).
Summarized Data of Down or Upregulation Expression of Transcriptomes
This study had some limitations; our device was not able to lower the temperature for 12°C. We did not assess the levels of inflammatory cytokines, which may have a crucial role in cancer cells behavior. Our sample size was limited, and this study was a proof of concept of the hypothermic-induced alteration of key proteins in invasion and metastasis of cancer cells. We investigated different types of tumors in different sizes to prove the hypothermal effect on cancer cells regardless of their size or types.
These findings open up intriguing possibilities for further research on the application of controlled hypothermia in cancer surgical regions to keep tumors in a hypoactive state during surgery. Future investigations are needed to clarify the role of cooling in reducing tumor invasion and to understand the long-term effects of MMP2/9 and CDH downregulation. Additionally, further studies are required to better elucidate the role of intraoperative mild cooling in activating environmental stress and its impact on HIF and GLUT-1 expression in cancer cells' glycolytic pathways.
Conclusion
Intraoperative mild cooling resulted in downregulation of key proteins playing a role in invasion and metastasis. However, the observed increase in YB-1 and N-Cad expression underscores the need for caution in the application of cooling strategies, as they may trigger adaptive responses in cancer cells. This study lays the groundwork for further research and optimization of intraoperative mild cooling as an innovative approach to cancer treatment. Additional investigations will be crucial in fully understanding the complexities of cooling-induced transcriptome alterations and their implications for long-term patient outcomes.
Consent for Publication
All authors give their consent for the publication of this manuscript.
Authors' Contribution
M.A. and S.R.M. devised the original study design. N.T., A.N., K.N., and A.G. performed the data collection. A.G. performed statistical analyses. N.T., A.N., K.N., A.G., and M.A. interpreted the results. A.N. and K.N. wrote the article.
Author Confirmation Statement
Dr. Tavassoli and Dr. Rouhollah Miri are from Tehran University of Medical Sciences (Tehran, Iran); Dr. Ghahremani, Dr. Namakin, Dr. Naserghandi, and Dr. Abdolahad are from University of Tehran (Tehran, Iran); and Dr. Namakin and Dr. Naserghandi are from Shahid Beheshti University of Medical Sciences (Tehran, Iran), all where education and research are the primary functions.
Ethical Approval and Consent to participate
All patients gave their informed consent according to an ethical approved protocol by the institutional review board of Tehran University of Medical Sciences (IR.TUMS.IKHC.REC.1401.449)
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Tehran University of Medical Sciences, Tehran, Iran.