
Abstract
Cryotherapy, a therapeutic technique involving localized cooling of the body, has gained popularity for postsurgical rehabilitation. It induces a reduction in cellular metabolism, vasoconstriction, and pain relief, making it an attractive option for managing postoperative (PO) shoulder pain. This systematic review aimed to assess the effectiveness of cryotherapy in PO shoulder patients, focusing on pain, range of motion, functionality, and temperature changes. The review included six randomized clinical trials, involving a total of 233 patients who underwent various shoulder surgeries. Cryotherapy was applied using different methods, including Cryo/Cuff, Cryoton®, Polar Care 300, and ice packs. Results indicated that cryotherapy was generally effective in reducing PO shoulder pain. However, one study found no significant difference in pain outcomes between the cryotherapy group and control group. Furthermore, three studies demonstrated a decrease in intra-articular and skin temperatures with cryotherapy application. A risk of bias analysis revealed some concerns in the overall risk of bias for five studies, with one study considered to have a high risk of bias. Although publication bias assessment was not conducted due to the limited number of included studies, it was noted that the studies exhibited heterogeneity in terms of population, intervention methods, and outcome measures. In conclusion, cryotherapy appears to be a promising adjunctive treatment for PO shoulder pain, although the existing evidence has some limitations, including small sample sizes and methodological concerns. More high-quality studies are needed to establish the full extent of cryotherapy's effectiveness in PO shoulder rehabilitation, especially regarding its impact on functionality and range of motion.
Introduction
Cryotherapy, aimed at the rehabilitation process, is a set of techniques that use temperatures from 0°C to 18.3°C, with the characteristic of removing heat from the body in a localized way immediately after application (Freire et al., 2015; Kwiecien and McHugh, 2021). This cooling promotes a reduction in cellular metabolism, leading cells to decrease their metabolism and normal oxygen consumption (Bae et al., 2015; Jia et al., 2008; Wakabayashi et al., 2018).
These changes cause chain effects as they cause vasoconstriction, consequently reducing exudate in the region (Christmas et al., 2016; Khoshnevis et al., 2016; Knobloch et al., 2007; Knobloch et al., 2006). In addition, cryotherapy also promotes relief of algia by decreasing nerve conduction, increasing the threshold of painful fibers, and interrupting the cycle of spasm and pain (Filippiadis et al., 2021; Krampe et al., 2023; Ruddy et al., 2019).
With the passage of time and advances in the means of applying cryotherapy, this treatment model underwent improvements and spread throughout the world. In this sense, this therapeutic modality has been widely used in postsurgery (Levy et al., 1997; Swenson et al., 1996) and for other purposes, both by lay people and health professionals, as they are low-cost techniques with good therapeutic results and easy to apply (Lince-Deroche et al., 2018).
Cryotherapy can be used to treat lesions in different body regions (Knobloch et al., 2007; Mendes et al., 2022; Nachiyunde and Lam, 2018). One of those is the shoulder, which has a large range of motion and low stability (Best and Tanaka, 2018). Shoulder pain affects a large number of people and when it becomes chronic in cases of adhesive capsulitis, impingement syndrome, and calcified tendonitis, etc., functional incapacity and nocturnal pain are common, leading to reduced hours of sleep associated with obesity, diabetes, hypertension, and cardiovascular diseases, among other comorbidities (Barandiaran et al., 2022).
In addition to the aforementioned diseases, other conditions such as osteoarthritis, rheumatoid arthritis, glenohumeral dislocation, osteonecrosis, and fractures often require surgical interventions, especially when conservative treatment fails, and these are surgeries of various types such as acromioplasty, joint stabilization surgery, and even arthroplasty (Buck et al., 2008; Coyner and Arciero, 2018; Getz et al., 2019).
After the surgical procedure, analgesic actions are important, usually promoted by analgesics, anti-inflammatories, gabapentinoids, and even nerve blocks; however, such actions are not without risks and side effects (Huang et al., 2017; Marty et al., 2018). In this way, physical analgesic resources such as cryotherapy are used for shoulders in the postoperative (PO) period; however, their evidence is still surrounded by gaps. The motivation for developing this study arose from an interest in synthesizing data on the application and effectiveness of this therapy.
The aim of this study was therefore to carry out a review of the effectiveness of cryotherapy on shoulders in the PO period, regarding pain outcome, range of motion, functionality, and skin and intra-articular surface temperatures.
Materials and Methods
Protocol and registration
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement. It is registered with the International Prospective Register of Systematic Reviews (PROSPERO) CRD42022382413.
The search was carried out in the PubMed, Web of Science, Scopus, Embase, Lilacs, Cochrane, and Livivo databases, as well as in the gray literature through Google Scholar, OpenGrey, and the CAPES Catalog of Dissertations and Theses. The search terms are shown in Supplementary Appendix SA1, and the search took place on January 20, 2023.
Eligibility criteria
The acronym, PICOS, was used to formulate the question focused on in this study: P—population: individuals undergoing any shoulder surgical procedure; I—intervention: any type of cold therapy; C—comparison: placebo, simulated, and no treatment; O—outcomes: pain, ROM, functionality, and superficial skin and intra-articular temperatures; and S—study design: randomized clinical trials. There were no restrictions on period or language.
Inclusion criteria were PO shoulder patients undergoing any form of cryotherapy, of both sexes, and without age limit. Exclusion criteria were case studies, systematic reviews, case reports, cohort studies, literature reviews, editorials, and animal studies.
Selection of studies
Two independent reviewers (R1 and R2) selected the included articles in two phases. In the first phase (phase 1), the two reviewers assessed titles and abstracts according to the eligibility criteria; and in the second phase (phase 2), they examined the full texts and selected articles according to the same criteria as in phase 1; they then checked all the information found. In the case of disagreements, a third reviewer (R3) participated before a final decision was made in both phases.
If important data in a review were missing or unclear, contact was made with the corresponding author of the study to resolve or clarify the problem.
Data collection
Data on the characteristics of the studies (authors, year of publication, and country), sample (sample size, average age, and gender), intervention modality and protocol, evaluation times, results, and conclusions were collected. The primary outcome was pain and secondary outcomes were range of motion, functionality, and skin and intra-articular surface temperatures.
Individual assessment of the risk of bias
The risk of bias was assessed using the Cochrane ROB 2 tool by blinded reviewers, R1 and R2, with any discrepancies being resolved by R3. All the included studies were assessed in five domains: bias in the randomization process; deviations from the intended intervention; bias due to missing data; bias in measurement of outcomes; and bias in selection of reported results. Each domain had an overall score for low risk and unclear or high risk.
Assessing the risk of publication bias
To reduce the likelihood of publication bias, a thorough search was carried out without limitations to language and period and with the inclusion of gray literature (Paez, 2017). Then, the risk of publication bias could be mitigated.
Results
Selection of studies
During the study selection process, 1067 records were initially found, of which 937 were in the main indexed databases and 130 in the gray literature. The search was carried out in all the databases on the same day (Supplementary Appendix SA1).
Of the total of 1067 studies, EndNote found 291 duplicates, which were automatically excluded from the indexed literature, and a further 77 were removed manually; from the gray literature, 128 duplicate studies were excluded automatically and 122 were removed manually. Then, in a new removal of duplicates using Rayyan, a further 79 duplicates were identified, leaving 569 studies for Phase 1 (reading titles and abstracts). After a primary selection, 37 studies remained for Phase 2 (reading the full texts), and finally, 6 studies were included in this review (Fig. 1).
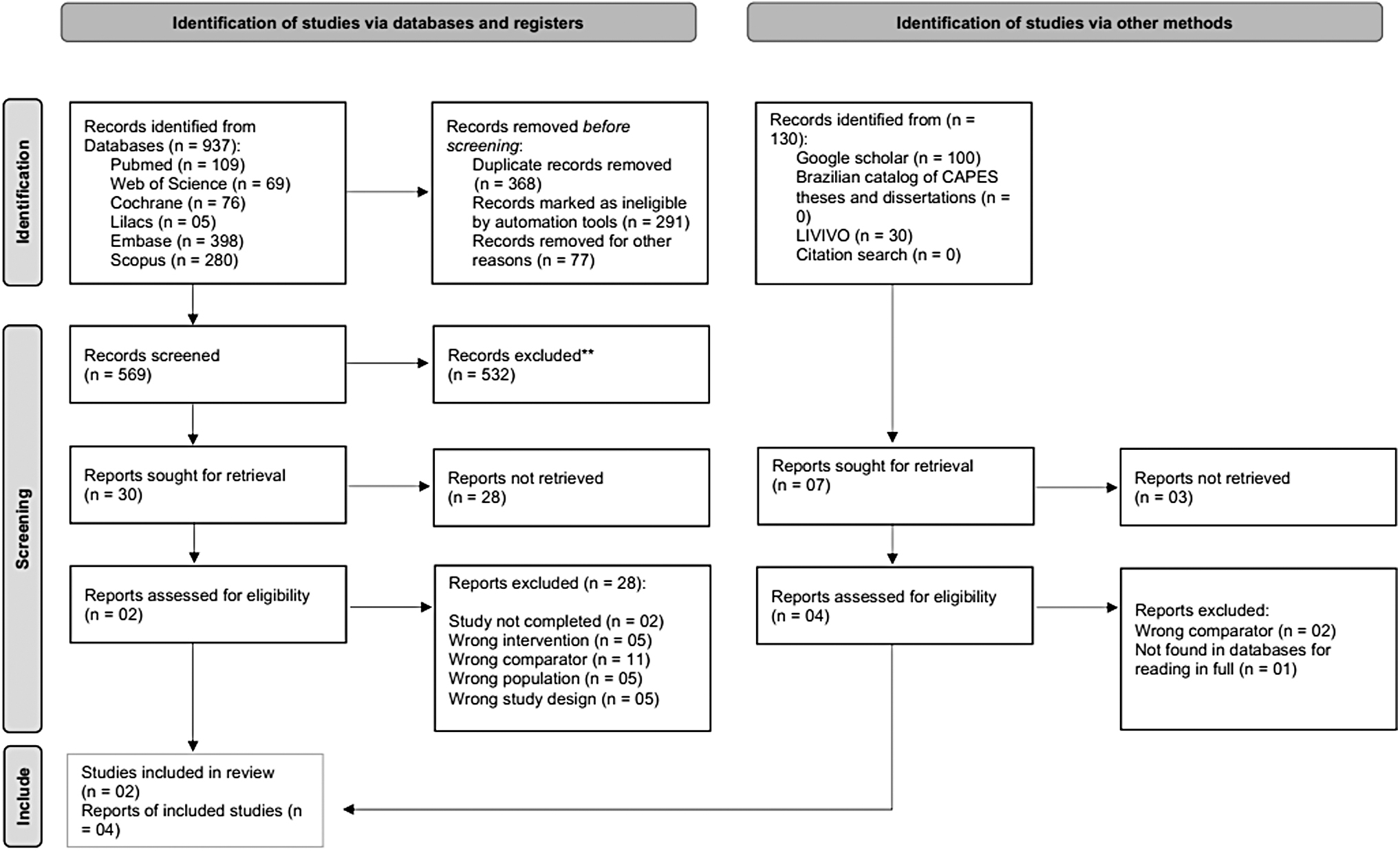
PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases, registers, and other sources. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analysis.
Results of individual studies
The individual results of this study are summarized in Table 1. For the 6 clinical trials included (Kara et al., 2020; Levy et al., 1997; Meeusen et al., 2004; Osbahr et al., 2002; Singh et al., 2001; Speer et al., 1996), the total sample comprised 233 patients: 110 with cryotherapy intervention, 93 controls without intervention, 5 placebos, and 25 with another intervention (n = 5, warm water; and n = 20, subacromial injection of lidocaine and bupivacaine).
Presentation of the Articles Included in the Systematic Review
N: total number of the sample; M: male; F: female; T0: baseline; T1: tempo 1; T2: tempo 2; T3: tempo 3; T4: tempo 4; T5: tempo 5; T6: tempo 6; EG1: experimental group 1; EG2: experimental group 2.
CG, control group; EG, experimental group; PO, postoperative; PG, placebo group; RCT, randomized clinical trial; SI, subacromial injection; VAS, Visual Analog Scale.
Four studies included an arthroscopic shoulder procedure (Kara et al., 2020; Levy et al., 1997; Meeusen et al., 2004; Osbahr et al., 2002), one study included arthroscopic and open procedures (Singh et al., 2001), and one study described the procedure as anterior shoulder stabilization, rotator cuff repair, or total shoulder replacement, but without further details (Speer et al., 1996).
Analysis of the risk of bias
This review selected 6 randomized clinical trials that met the eligibility criteria (Getz et al., 2019; Huang et al., 2017; Levy et al., 1997; Marty et al., 2018; Meeusen et al., 2004; Speer et al., 1996). Regarding the randomization process, only two studies presented low risk of bias (Singh et al., 2001; Speer et al., 1996), but all studies had low risk of bias in the domains of deviations from the planned interventions and missing data in the results.
Four studies were considered to be at low risk of bias in the domain of outcome measurement (Levy et al., 1997; Meeusen et al., 2004; Osbahr et al., 2002; Singh et al., 2001). Only one study presented a high risk of bias in the domain of selection of reported outcomes (Singh et al., 2001). In the overall result of the bias analysis, five studies were considered and some relevant problems were detected (Kara et al., 2020; Levy et al., 1997; Meeusen et al., 2004; Osbahr et al., 2002; Speer et al., 1996) and one study was considered to be at high risk of bias (Singh et al., 2001).
The summary of the risk of bias analysis is shown in Figure 2 and the graph of the domains is shown in Figure 3.
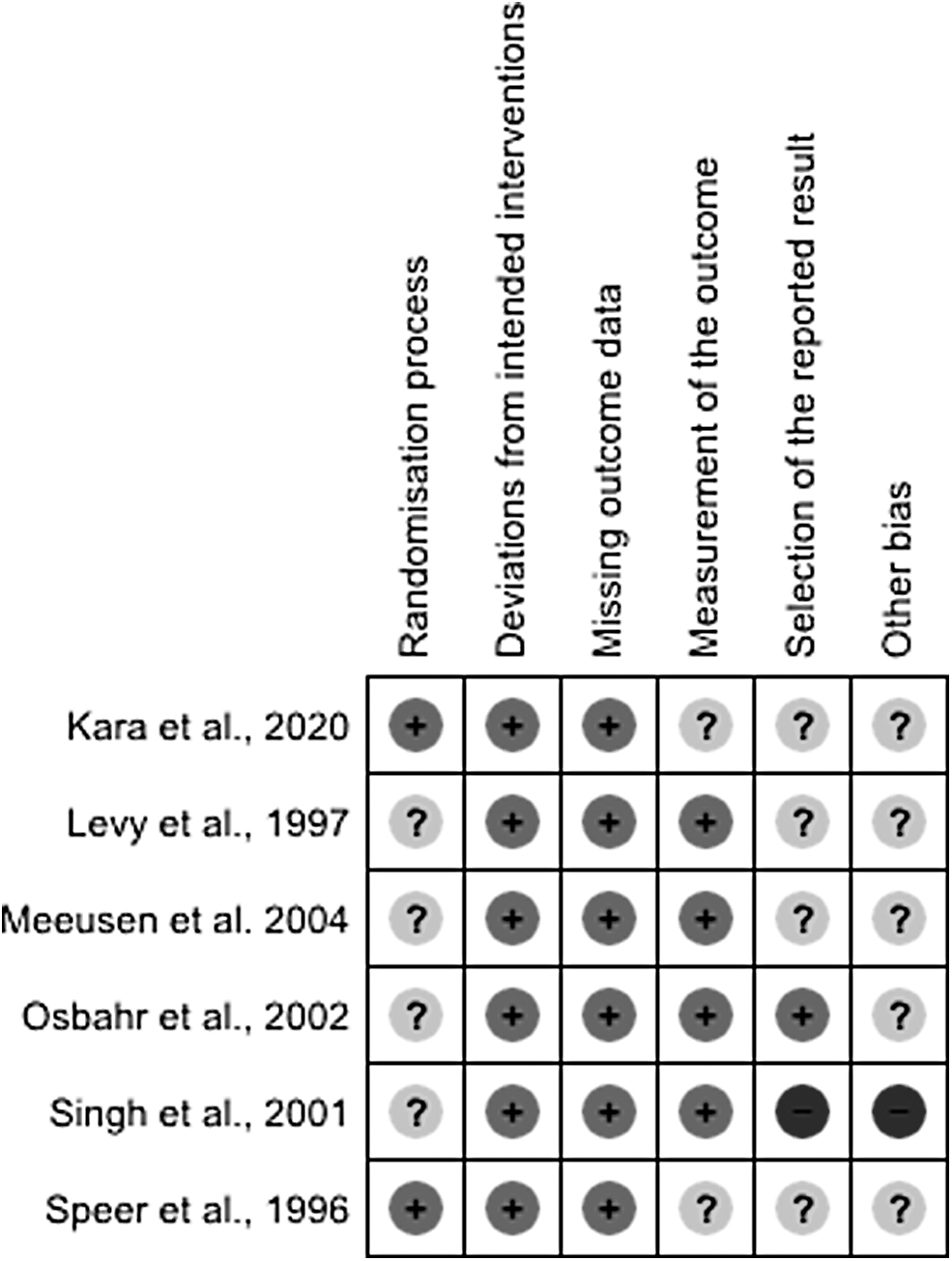
Risk of bias summary: review authors' judgments about each risk of bias item for each included study.

Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
Collection instruments
Different instruments were used to measure the outcome of this study. Only the Visual Analog Scale (VAS) was used to assess the pain outcome in the four studies that carried out this analysis (Kara et al., 2020; Meeusen et al., 2004; Singh et al., 2001; Speer et al., 1996).
Cryo/Cuff was used as an intervention in two studies (Levy et al., 1997; Speer et al., 1996), Cryoton was used in one study (Meeusen et al., 2004), Polar Care 300 was used in one study (Osbahr et al., 2002), and ice packs were used in two studies (Kara et al., 2020; Singh et al., 2001).
Outcomes
Primary outcome—pain
With regard to pain, cryotherapy has been shown to be effective in reducing frequency and severity, as well as making postsurgical recovery more comfortable (Speer et al., 1996). At the same time, other authors also found that cryotherapy has a positive effect on reducing PO pain (Meeusen et al., 2004) by reducing its intensity and frequency (Singh et al., 2001).
However, in another study, there was no significant difference between the groups that received ice packs, subacromial injections (second intervention group), and the control group (Kara et al., 2020).
Secondary outcomes—range of motion and functionality
As for range of motion and functionality, none of the articles included in this systematic review presented any method of assessing this outcome.
Secondary outcomes—intra-articular and superficial skin temperatures
With regard to intra-articular temperature, continuous cryotherapy caused a significant reduction in the temperatures of the glenohumeral joint and the subacromial space during the first 23 hours after surgery (Osbahr et al., 2002). Similarly, the intra-articular and skin temperatures in the group undergoing cryotherapy were significantly lower than in the control group (Meeusen et al., 2004).
On the other hand, in the study by Levy et al. (1997), there was no difference between the groups that did or did not receive the intervention.
Discussion
This systematic review was developed with the aim of verifying the effects of cryotherapy on pain and, secondarily, on range of motion, functionality, and skin and intra-articular surface temperatures in the shoulder in the PO period. It is known that controlling pain after surgery is crucial to ensuring rapid rehabilitation and early discharge from the hospital (Fusco et al., 2018; Ilfeld et al., 2003; Ilfeld et al., 2002; Nachiyunde and Lam, 2018), and cryotherapy has been shown to be a useful tool in reducing pain after anterior cruciate ligamentoplasty of the knee (Mendes et al., 2022).
To this end, one of the possible therapeutic modalities is cryotherapy since the technique of using cold therapy suggests a reduction in pain. Therefore, three studies included in this systematic review show effective results with the use of cryotherapy to minimize pain resulting from surgical procedures (Meeusen et al., 2004; Singh et al., 2001; Speer et al., 1996).
In a study of 20 patients who had undergone acromioplasty surgery, cryotherapy was applied using Cryoton at a temperature of −78°C for a duration of 45 seconds at high pressure (50 bar). This procedure was carried out in two different areas, one under the surface of the acromion and the other in the deltoid region, with the cycle repeated every 3 hours. The VAS was used to assess pain, and the experiment group had a significantly lower pain score when compared with the control group. According to the authors, the effectiveness of cryotherapy in reducing pain is mainly due to cutaneous and subcutaneous analgesia, which occurs when tissues are subjected to temperatures between 10°C and 15°C (Meeusen et al., 2004).
In another study, carried out with 70 patients, the individuals in the intervention group had the therapy administered by means of a cryotherapy pad for 21 days, with continuous application in the first 48 hours after surgery, during the night from the second to the seventh day, and after this period until the 21st day, only during rehabilitation exercises.
The VAS and a subjective report were used as parameters. They found that cryotherapy is an effective method for controlling PO shoulder pain. They report that the mechanism of cryoanalgesia is related to the action of increasing the pain threshold of nerve fibers and early application of this treatment promotes vasoconstriction capable of reducing hemorrhage and inflammation resulting from the surgical process (Singh et al., 2001).
Similarly, in a study of 50 individuals undergoing total glenohumeral joint replacement, open rotator cuff repair, or open shoulder stabilization, cryotherapy was applied using Cryo/Cuff immediately after the surgical procedure, and this treatment plan was followed until the 10th day of rehabilitation. Pain was assessed using a questionnaire, which included intensity and frequency, and the VAS. The worst pain experienced by the cryotherapy group was on the first PO night and it was less intense and less frequent compared with the noncryotherapy group, which was repeated on the 10th PO day (Speer et al., 1996).
However, Kara et al. (2020) found no difference between the experimental group and control group for the pain outcome, and in an analysis of 59 patients undergoing arthroscopic rotator cuff repair surgery, cryotherapy was applied using an ice pack on the affected site for 7 days. On the first 3 days, the therapy was administered with an interval of 1 hour, and on subsequent days, it was administered only three times a day, with each application lasting 1 hour. The authors argue that the lack of effect may have been due to the large muscle mass and high vascularization in this region, as well as the difficulty of applying the therapy around the shoulder.
On the other hand, three studies (Levy et al., 1997; Meeusen et al., 2004; Osbahr et al., 2002) sought to verify the efficacy of cryotherapy in reducing glenohumeral intra-articular and subacromial space temperatures, only one of which did not also evaluate the reduction in skin temperature (Levy et al., 1997) and did not observe a reduction in temperature after using Cryo/Cuff. In the other two studies (Meeusen et al., 2004; Osbahr et al., 2002), positive results were found for cooling of the skin, glenohumeral joint, and subacromial space from the comparative analysis between the group that received the intervention and a comparator group.
In the studies by Speer et al. (1996), Meeusen et al. (2004), and Singh et al. (2001), it was found that cryotherapy reduced PO shoulder pain. It is worth noting that the risk of bias in five articles (Kara et al., 2020; Levy et al., 1997; Meeusen et al., 2004; Osbahr et al., 2002; Speer et al., 1996) showed concerns in relation to the overall risk of bias, and one article was considered to have a high risk of bias (Singh et al., 2001). With regard to assessing publication bias, as the number of articles included in this systematic review was less than 10 (n = 6), it is not recommended to carry out this type of analysis.
The limitations identified in this systematic review include the heterogeneity of the primary studies in terms of population, intervention procedure, and outcome measures. In addition, a small sample size was identified, which reflects on the quality of the proposed research. Finally, it was pointed out that there was a discrepancy between the studies included in relation to the duration of the therapy (both the use of cryotherapy and the therapeutic process) and the follow-up after the intervention was administered. In view of the above, there is a clear need to develop new studies on the effectiveness of cryotherapy on the shoulder in the PO period, using other measures to assess pain, in addition to the VAS.
Although there is no consensus in the literature, there have been reports that the various forms of cryotherapy (Cryo/Cuff, Cryotron®, ice pack, and cryotherapy shoulder pad) help to significantly reduce PO shoulder pain. On the other hand, others have shown no evidence that cryotherapy is capable of reducing joint temperatures, and only superficial skin temperature was reduced.
In a different anatomical region (triceps suralis), Gillette and Merrick (Gillette and Merrick, 2018) observed a reduction in temperature by inserting thermistors 1 cm below the adipose tissue, and Long et al. (2005) found an intramuscular temperature reduction at a depth of up to 2 cm, similar to that cited by Enwemeka et al. (2002) with a reduction in temperature at a depth greater than 2 cm; such actions of cryotherapy are also reported in Mac Auley's review (Mac Auley, 2001).
However, the literature on this treatment for shoulders in the postsurgical period is still scarce, although it is always used clinically, in addition to the fact that the sample sizes were generally small and evaluation times between studies were discrepant. Therefore, there is a clear need for more studies that seek to show how cryoanalgesia is effective, as well as the relationship between the effects of cryotherapy penetration on joint and surface temperatures and its influence on the functionality and range of movement of the joint in question.
In addition, it is useful to update studies that aim to clarify whether this shoulder treatment technique is an intervention with significant results in the PO period.
Conclusions
Cryotherapy is effective in minimizing pain in the shoulder postoperatively and can be used as an adjunct to shoulder rehabilitation. However, the results suggest the need for more primary studies with a low risk of bias.
Footnotes
Authors' Contributions
A.J.B.G., G.B.H., and M.Z.G. participated in drawing up the research project, searching for manuscripts, analyzing data, and writing the manuscript. D.B., M.R.B., and G.R.F.B. participated in the preparation of the research project, data analysis, and critical review of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.