
Abstract
Temperature control is the only neuroprotective intervention suggested in current international guidelines for patients with return of spontaneous circulation after cardiac arrest, but the prevalence of temperature control therapy, temperature settings, and outcomes have not been clearly reported. We aimed to investigate changes over 7 years in provision of temperature control treatment among out-of-hospital cardiac arrest (OHCA) patients in Kanto region, Japan. Data of all adult OHCA patients who survived for more than 24 hours in the prospective cohort studies, SOS-KANTO 2012 (conducted from 2012 to 2013) and SOS-KANTO 2017 (conducted from 2019 to 2021), in Japan were included. We compared the prevalence of temperature control and the proportion of mild (≥35°C) and moderate (from 32°C to 34.9°C) hypothermia between the two study groups. We also performed a Cox regression analysis to evaluate 30-day mortality adjusted by temperature control therapy (none, moderate hypothermia, or mild hypothermia), age, sex, past medical history, witnessed status, bystander cardiopulmonary resuscitation, initial rhythm, location of arrest, and dataset (SOS-KANTO 2012 or 2017). We analyzed data from 2936 patients (n = 1710, SOS-KANTO 2012; n = 1226, SOS-KANTO 2017). Use of temperature control was lower (45.3% vs. 41.4%, p = 0.04), moderate hypothermia was lower (p < 0.01), and mild hypothermia was higher (p < 0.01) in SOS-KANTO 2017 compared with SOS-KANTO 2012. The survival rate was significantly higher for patients with mild (p < 0.01) and moderate (p < 0.01) hypothermia compared with those who did not receive temperature control therapy. Overall, the incidence of moderate hypothermia decreased and that of mild hypothermia increased and the use of temperature control decreased between the two studies conducted 7 years apart in the Kanto area, Japan. Temperature control management might improve survival of patients with OHCA.
Introduction
Among patients with return of spontaneous circulation (ROSC) after cardiac arrest (CA), postanoxic brain damage is one of the most serious complications (Lemiale et al., 2013). Temperature control is the only neuroprotective intervention suggested in the current international guidelines (Sandroni et al., 2022).
The concept of temperature control therapy after CA has changed drastically over the decades. Hypothermia was first used after CA in 1958, and guidelines published by the International Committee on Resuscitation (ILCOR) in 2005 suggested that therapeutic hypothermia after CA was effective (Bonaventura et al., 2016).
The 2010 American Heart Association (AHA) guidelines and the 2013 European Resuscitation Council (ERC) guidelines recommend that the temperature of patients with ROSC after out-of-hospital CA (OHCA) caused by ventricular fibrillation should be controlled at 32–34°C. The targeted temperature management trials published in 2013 and other studies reported that targeted hypothermia might not be more effective than targeted normothermia (Bonaventura et al., 2016; Nielsen et al., 2013).
In the 2020 AHA guidelines and 2021 ERC guidelines, temperature control targeting a temperature from 32°C to 36°C was recommended for all post-CA patients, regardless of initial rhythm, and the 2020 Japan Resuscitation Council (JRC) guidelines include a similar recommendation (Japan Resuscitation Council, 2020; Nolan et al., 2021; Panchal et al., 2020).
These changes likely influenced patient management after CA in the real world (Tagami et al., 2016), but the prevalence of temperature control therapy, temperature settings used, and outcomes have not been consistently reported. The aim of the current study was to compare the provision of temperature control treatment among OHCA patients using data from two multicenter prospective studies conducted over 7 years in the same region of Japan.
Methods
Ethical considerations
The present study adhered to the principles of the Declaration of Helsinki and was approved by the ethics committee at the Nippon Medical School Tama Nagayama Hospital (reference number 597). Our analysis did not include personal identifying information of patients, so the requirement for informed consent was waived.
Study design and population
This study was one of the predefined themes of SOS-KANTO 2017, a multicenter prospective study performed in the Kanto region of Japan. The SOS-KANTO study was supported by the Kanto Regional Group of the Japanese Association for Acute Medicine.
The previous studies were conducted to collect prehospitalization records of all-cause CA patients who were transported to participating hospitals by trained emergency medical service (EMS) providers and who were admitted to participating hospitals. The Kanto region is situated in the middle part of Japan, and the area is about 32,000 square kilometers. The population in this area is about 41 million, that is, over 30% of the population in Japan.
The database includes information about patients' on-scene vital signs, patients' background, initial rhythm documented by EMS, the cause of OHCA, hospital arrival time, vital signs upon arrival at the hospital, treatments in the hospital, onset time of OHCA, neurological outcome, and mortality (SOS-KANTO Study Group, 2015; SOS-KANTO Study Group, 2015; Tanaka et al., 2016).
All adult OHCA patients who were enrolled in SOS-KANTO 2012 and 2017 were included. Patients <18 years old, patients who died within 24 hours of CA, and patients with missing discharge date information were excluded. The studies were conducted from January 2012 to March 2013 for the SOS-KANTO 2012 study and from September 2019 to March 2021 for the SOS-KANTO 2017 study.
Definitions and data collection
CA was defined as the absence of a pulse and normal breathing (Jacobs et al., 2004). We used the term “temperature control,” aiming for targeted hypothermia and targeted temperature management, because the ILCOR Advanced Life Support Task Force recently adopted the term (Sandroni et al., 2022).
Neurological outcomes at discharge from hospital were defined using the cerebral performance category (CPC) score, as follows: (1) good performance; (2) moderate disability; (3) severe disability; (4) vegetative state; and (5) death (Jacobs et al., 2004; Tagami et al., 2012). We grouped CPCs 1 and 2 as favorable outcomes and CPCs 3, 4, and 5 as poor outcomes in accordance with previous studies (Jacobs et al., 2004; SOS-KANTO 2012 Study Group, 2015; SOS-KANTO Study Group, 2015; Tagami et al., 2012).
The temperature control targets in the SOS-KANTO 2012 study were “hypothermia” and “avoid hyperthermia” and the numeric target temperature range was from 32.0°C to 38.5°C. In contrast, the SOS-KANTO 2017 study used only “temperature control” and the numeric target temperature range was from 32°C to 36°C.
Therefore, on the basis of previous studies, we defined the targeted temperature for moderate hypothermia as being from 32°C to 34.9°C and that for mild hypothermia as being ≥35°C for the current study (Düggelin et al., 2021; Granfeldt et al., 2021; Nolan et al., 2021; Sanfilippo et al., 2021).
Outcome measures
The main outcome measures were the prevalence of temperature control treatment and the proportion of mild and moderate hypothermia. Secondary outcome measures were 30-day mortality and the proportion of favorable outcomes at 1 month.
Statistical analysis
We compared patients' background and covariates between the SOS-KANTO 2012 and SOS-KANTO 2017 study groups. Results are expressed as median (interquartile range [IQR]) for non-normally distributed data. Continuous variables were analyzed using Student's t-test or the Mann–Whitney U test, and categorical variables were analyzed using the chi-square test or Fisher's test, as appropriate. We then compared outcomes between the two groups based on initial rhythm.
Moreover, we performed multiple imputation to decrease the bias caused by incomplete data: each missing value was replaced with a set of five plausible substitute values, and one model was created by statistical inference with the results of the five imputed datasets (Janssen et al., 2010; Little et al., 2012).
Finally, we conducted a survival analysis using Cox proportional hazards regression analysis. We chose covariates that were independently associated with mortality, according to previous studies, as follows: temperature control therapy (none, moderate hypothermia, or mild hypothermia), age, sex, past medical history, witnessed status, bystander cardiopulmonary resuscitation (CPR), initial rhythm, location of arrest, and database (SOS-KANTO 2012 or 2017) (Al-Dury et al., 2020; Kim et al., 2023; Mathew et al., 2021).
A p-value of ≤0.05 was considered to indicate statistical significance. All data were analyzed using SPSS software (version 28; IBM Corp., Armonk, NY).
Results
Among 16,452 patients in the SOS-KANTO 2012 study and 9909 patients in the SOS-KANTO 2017 study, 2936 adult patients who survived at least 24 hours after admission were included in our analysis (n = 1710, SOS-KANTO 2012; n = 1226, SOS-KANTO 2017) (Fig. 1).

Patient selection.
Patients' demographic information is presented in Table 1 and Supplementary Table S1. There were no statistically significant differences in age (68 years [IQR: 57–79] vs. 70 years [IQR: 56–79]; p = 0.14), sex (p = 0.59), or the cause of CA (p = 0.29). However, the proportion of patients with ischemic heart disease was higher (6.6% vs. 10.6%; p < 0.01) and baseline activities of daily living in patients with disability were higher (p < 0.01) in the SOS-KANTO 2017 group compared with the SOS-KANTO 2012 group.
Patient Demographics and Clinical Characteristics upon Hospital Admission
Data are provided as the number of positive observations/total number of observations (%) or as median (IQR). For each variable, the number of missing observations can be obtained as the difference between the total number of patients in each phase and the total number of observations.
Lactate was measured in 1344 patients in the SOS-KANTO 2012 study and in 459 patients in the SOS-KANTO 2017 study.
Arterial blood gas was measured in 1607 patients in the SOS-KANTO 2012 study and in 463 patients in the SOS-KANTO 2017 study.
Others included any ECGs of the patients with return of spontaneous circulation after cardiac arrest.
ACS, acute coronary syndrome; ADL, activities of daily living; BE, base excess; CA, cardiac arrest; ECG, electrocardiogram; GCS, Glasgow Coma Scale; Hb, hemoglobin; HCO3, bicarbonate; IQR, interquartile range; K, potassium; PaCO2, partial pressure of carbon dioxide; PaO, partial pressure of oxygen; PEA, pulseless electrical activity; VF, ventricular fibrillation; VT, ventricular tachycardia; WBC, white blood cells.
Table 2 shows the patients' prehospital information and EMS procedures. Defibrillation by a citizen and bystander CPR were more often performed in SOS-KANTO 2017 than in SOS-KANTO 2012 (34.4% vs. 44.2%; p < 0.01; 48.6% vs. 54.7%; p < 0.01, respectively). For prehospital treatments by EMS, intravenous access, epinephrine administration, and airway management were more successful in SOS-KANTO 2017 than in SOS-KANTO 2012 (27.1% vs. 42.1%, p < 0.01; 21.3% vs. 31.4%, p < 0.01; and p < 0.01, respectively).
Prehospital Patient Demographics and Clinical Characteristics
Data are provided as the number of positive observations/total number of observations (%) or as median (IQR). For each variable, the number of missing observations can be obtained as the difference between the total number of patients in each phase and the total number of observations.
Others included any ECGs of the patients with return of spontaneous circulation after cardiac arrest.
CPR, cardiopulmonary resuscitation; EMS, emergency medical service; IQR, interquartile range; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation; VF, ventricular fibrillation; VT, ventricular tachycardia.
The percentage of patients undergoing temperature control was lower in the SOS-KANTO 2017 group compared with SOS-KANTO 2012 group (45.3% vs. 41.4%; p = 0.04) (Table 3). Focusing on initial rhythm, the proportion of patients undergoing temperature control in the SOS-KANTO 2012 group did not differ from that in the SOS-KANTO 2017 group among patients with a shockable rhythm on scene (68.9% vs. 66.4%; p = 0.46).
In-Hospital Treatments
Data are provided as the number of positive observations/total number of observations (%).
For each variable, the number of missing observations can be obtained as the difference between the total number of patients in each phase and the total number of observations.
ECMO, extracorporeal membrane oxygenation; PCI, percutaneous coronary intervention.
Conversely, temperature control was performed less often in the SOS-KANTO 2017 group than in the SOS-KANTO 2012 group among patients with a nonshockable rhythm (39.5% vs. 32.0%; p < 0.01).
Similar trends for temperature control target range were observed in all groups, including those with a shockable or nonshockable rhythm (Fig. 2). The proportion of moderate hypothermia was lower and that of mild hypothermia was higher in the SOS-KANTO 2017 group compared with that in the SOS-KANTO 2012 group (p < 0.01 and p < 0.01, respectively).

Prevalence of moderate and mild hypothermia, 30-day mortality, and favorable outcomes at 1 month, focusing on initial rhythms.
In addition, 30-day mortality in the SOS-KANTO 2012 group was not different from that in the SOS-KANTO 2017 group for all patients, patients with a shockable rhythm, and patients with a nonshockable rhythm (47.5% vs. 50.0%, p = 0.19; 29.1% vs. 34.8%, p = 0.11; and 67.4% vs. 66.3%, p = 0.67, respectively).
The results of the survival analysis using a Cox proportional hazards model to evaluate mortality, adjusted by temperature control therapy (none, moderate hypothermia, or mild hypothermia), age, sex, past medical history, witnessed status, bystander CPR, initial rhythm, location of arrest, and dataset (SOS-KANTO 2012 or 2017), are shown in Figure 3 and Table 4.
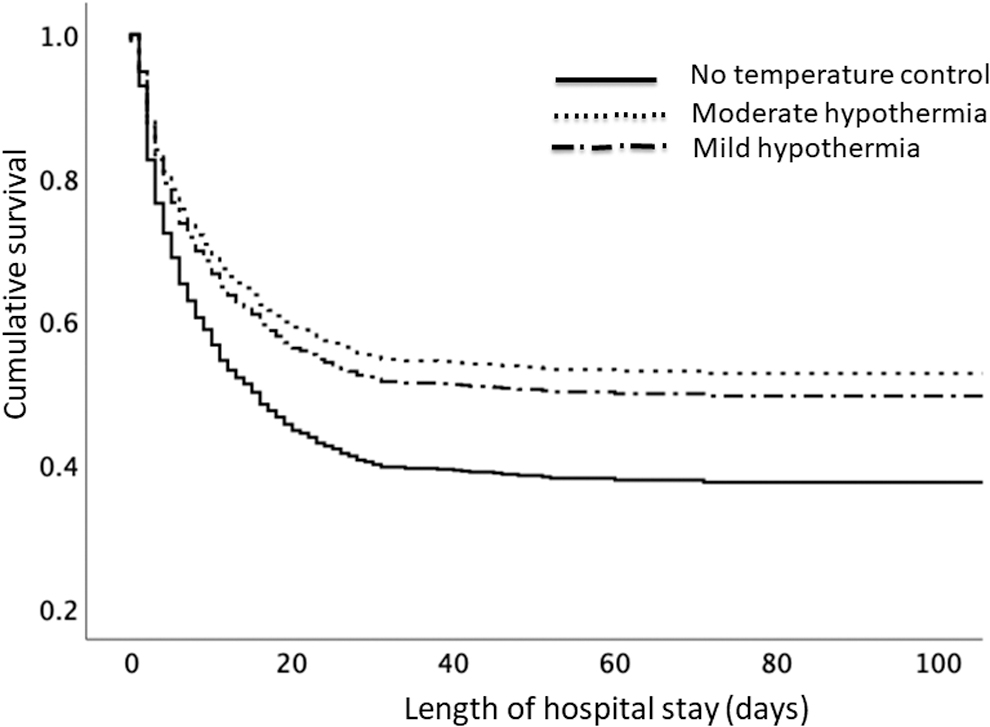
Survival analysis using Cox regression among patients with OHCA. OHCA, out-of-hospital cardiac arrest.
Cox Regression Analysis of the Risk of 30-Day Mortality Among Out-of-Hospital Cardiac Arrest Patients After Multiple Imputation
CI, confidence interval; CPR, cardiopulmonary resuscitation.
After adjusting for the dataset (SOS-KANTO 2012 or 2017), the survival rate was significantly higher for patients with mild hypothermia than for those who did not receive temperature control therapy (hazard ratio [HR], 0.73; 95% confidence interval [CI], 0.62–0.86; p < 0.01). Similarly, the survival rate was significantly higher for patients with moderate hypothermia than for those who did not receive temperature control therapy (HR, 0.66; 95% CI, 0.57–0.76; p < 0.01).
Discussion
The results of the current study indicated the following changes in neuroprotective treatment for post-CA patients: the proportion of moderate hypothermia was lower and that of mild hypothermia higher in the SOS-KANTO 2017 group compared with the SOS-KANTO 2012 group.
This significant change might reflect the revised guidelines for CA patients. Previous reports demonstrate that adherence to resuscitation guidelines improves outcomes (Hessulf et al., 2020; Honarmand et al., 2018; McEvoy et al., 2014). The ERC, AHA, and JRC guidelines published in 2020 and 2021 were revised to further emphasize post-CA care and to accept normothermia and hypothermia (Japan Resuscitation Council, 2020; Nolan et al., 2021; Panchal et al., 2020).
Technically, in the real world, maintaining normothermia is easier than adhering to a hypothermia protocol (Düggelin et al., 2021). This means that the temperature control target after CA tends to be higher and closer to normal body temperature. The results of our study suggest that resuscitation guideline revisions likely changed doctors' prescribing behavior in Japan and the guidelines had a substantial effect on clinical treatment.
Survival analysis showed that survival rates of patients who received mild or moderate hypothermia were significantly higher than those who did not receive temperature control treatment after adjusting for the data source (SOS-KANTO 2012 or 2017) and other variables that were independently associated with mortality. This result supports the efficacy of temperature control therapy compared with no temperature management.
Recent studies on temperature control therapy emphasize not only the comparison of targeted temperatures (33°C vs. 36°C) but also comparison between hypothermia and normothermia (Dankiewicz et al., 2021; Düggelin et al., 2021; Nielsen et al., 2013; Sanfilippo et al., 2021). However, our study classified the target temperature into moderate or mild hypothermia, and we did not assess normothermia; therefore, we cannot determine the ideal targeted temperature. Further studies are required to evaluate the optimal temperature to target for OHCA patients.
We also examined the effects of different prehospital treatments administered by EMS personnel, who have an important role in a chain of survival for patients with OHCA (Ong et al., 2018). Among our adult patients who survived at least 24 hours after ROSC, successful intravenous access, epinephrine administration, and airway management by EMS employees before arrival at the hospital occurred more often in the SOS-KANTO 2017 group than in the SOS-KANTO 2012 group.
The medical control protocol for OHCA patient management in the Kanto region did not change much during each study period; therefore, these results indicate that EMS provider skills have improved.
Limitations
There are some limitations in this study. First, the current study was a cohort design with a post hoc analysis using a multicenter database survey. However, sampling at the participating hospitals was not randomized or population based.
Second, the mild hypothermia group defined in our study must have included patients with normothermia. Besides, there is no standard definition of moderate hypothermia and mild hypothermia, and the definitions of the terms in the current study were its own, so we could not directly compare the results of this study with others.
Finally, the databases did not include information about do-not-resuscitate orders, indications for temperature control, or the reasons why doctors decided upon a targeted temperature.
Conclusions
The current study shows a clear trend for implementing temperature control after CA in Japan. Moderate hypothermia was lower, mild hypothermia was higher, and the proportion of temperature control was lower in the SOS-KANTO 2017 trial (2019–2021) compared with the SOS-KANTO 2012 trial (2012–2013). Our results support the efficacy of temperature control therapy for OHCA patients.
Footnotes
Authors' Contributions
C.T. was involved in conceptualization, methodology, analysis, and writing—original draft preparation. T.T., F.N., M.K., N.K., H.Y., S.A., M.T., and K.U. were involved in supervision and writing—reviewing.
Ethical Approval and Consent to Participate
The ethics committee at the Nippon Medical School Tama Nagayama Hospital approved the present study (reference number 597). Because we analyzed anonymous data, the requirement for written informed consent was waived.
Availability of Data and Materials
The data used in this study are available from the SOS-KANTO 2017 study group. However, restrictions apply to the availability of these data, which were used under the license for the current study, and thus, they are not publicly available. Data are available from the authors upon reasonable request and with the permission of the SOS-KANTO 2017 study group.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.