
Abstract
The effectiveness of target temperature management (TTM) in poor-grade aneurysmal subarachnoid hemorrhage (aSAH) remains a topic of debate. In order to assess the clinical efficacy of TTM in patients with poor-grade aSAH, we conducted a systematic review and meta-analysis. This research was registered in PROSPERO (CRD42023445582) and included all relevant publications up until October 2023. We compared the TTM groups with the control groups in terms of unfavorable outcomes (modified Rankin scale [mRS] score > 3), mortality, delayed cerebral ischemia (DCI), cerebral vasospasm (CVS), and specific complications. Subgroup analyses were performed based on country, study type, follow-up time, TTM method, cooling maintenance period, and rewarming rate. Effect sizes were calculated as relative risk (RR) using random-effect or fixed-effect models. The quality of the articles was assessed using the methodological index for non-randomized studies scale. Our analysis included a total of 5 clinical studies (including 1 randomized controlled trial) and 219 patients (85 in the TTM group and 134 in the control group). Most of the studies were of moderate quality. TTM was found to be associated with a statistically significant improvement in mortality (mRS score 6) rates compared with the control group (RR = 0.61, 95% confidence interval [CI]: 0.40–0.94, p = 0.026). However, there was no statistically significant difference in unfavorable outcomes (mRS 4–6) between the TTM and control groups (RR = 0.94, 95% CI: 0.71–1.26, p = 0.702). The incidence of adverse events, including DCI, CVS, pneumonia, cardiac complications, and electrolyte imbalance, did not significantly differ between the two groups. In conclusion, our overall results suggest that TTM does not significantly reduce unfavorable outcomes in poor-grade aSAH patients. However, TTM may decrease mortality rates. Preoperative TTM may cause patients to miss the opportunity for surgery, although it temporarily protects the brain. Furthermore, the incidence of adverse events was similar between the TTM and control groups.
Introduction
Poor-grade aneurysmal subarachnoid hemorrhage (aSAH), classified as World Federation of Neurosurgical Societies grade IV and V, Hunt-Hess IV and V, or Fisher 3-4, accounts for approximately 20–30% of all aSAH cases (Etminan et al., 2019). This severe form of aSAH is associated with high fatality and disability rates of 36% and 57%, respectively (Cho et al., 2018). Although immediate microclipping surgery or endovascular intervention is implemented, the effectiveness of these treatments remains disappointingly low, ranging from only 33% to 56%. Furthermore, the postoperative mortality rate varies significantly, ranging from 28% to as high as 58% (Zhao et al., 2014). These statistics highlight the challenging and life-threatening nature of poor-grade aSAH cases. Early bleeding in the brain leads to a rapid increase in intracranial pressure, which can result in complications such as acute vasospasm, reduced cerebral blood flow, dysfunction in cerebral vascular autoregulation, and brain swelling. These complications ultimately lead to acute neurological dysfunction. The occurrence of cerebral vasospasm (CVS) and delayed cerebral ischemia (DCI) after 72 hours following the initial bleeding often indicates an unfavorable outcome. Animal models of subarachnoid hemorrhage have shown that lowering body temperature can reduce brain edema and the occurrence of DCI through various mechanisms. These mechanisms include decreased brain metabolism, clearance of harmful free radicals, regulation of neuroinflammatory responses, and inhibition of neuronal cell death (Okazaki and Kuroda, 2018). The application of targeted temperature management (TTM), which has demonstrated benefits in patients with conditions such as cardiac arrest, hypoxic-ischemic encephalopathy, and ischemic stroke, has been extensively studied in animal models (Hillerson et al., 2023). TTM involves inducing hypothermia in patients with brain injury by cooling the entire body while maintaining core temperature. This study aims to evaluate the clinical efficacy and potential adverse events of TTM in poor-grade aSAH patients. TTM can be achieved through external surface cooling, the placement of a specialized transvenous endovascular cooling catheter in the inferior vena cava, or a combination of surface and endovascular cooling (Kobata et al., 2022; Taccone et al., 2022). Although animal experimental studies have shown the benefits of TTM, these advantages have not yet been implemented in clinical practice for poor-grade aSAH patients. One possible reason for this discrepancy is that the benefits of TTM may be outweighed by the risks and complications associated with the procedure. Therefore, this study aims to conduct a systematic review and meta-analysis of existing literature.
Methods
This study was registered on July 26, 2023, in the International Prospective Register of Systematic Reviews (PROSPERO, CRD42023445582). We conducted a systematic review and meta-analysis following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Shamseer et al., 2015).
Eligibility criteria
The following inclusion criteria were used to assess eligibility: (1) prospective, retrospective, and randomized controlled trials (RCTs); (2) the outcome measured as all-cause mortality and neurological outcome; (3) the control group received the same treatment except for TTM; (4) the recorded data included information on the TTM protocol, target temperature, rewarming rate, and any adverse events. The following studies were excluded: (1) animal experiments, case reports, case series, review articles, letters, comments, abstract, meta-analysis, repeated publication of the same data set, and insufficient data; (2) intraoperative application of hypothermia; (3) describing patients with traumatic brain injury, ischemic stroke, or hypoxic-ischemic encephalopathy. The search was limited to human studies published in the English language. The study selection process is outlined in Figure 1.

Flow chart of the search and selection process.
Search strategy
Using related databases, such as Embase, PubMed, Web of Science, and Cochrane Library, we systematically reviewed the clinical studies published in full in the English language before October 2023, keywords: “severe aneurysmal subarachnoid hemorrhage”, “poor grade aneurysmal subarachnoid hemorrhage”, “high grade aneurysmal subarachnoid hemorrhage”, “therapeutic hypothermia”, and “target temperature management”. Our included studies included prospective and retrospective studies of patients with poor-grade aSAH treated with TTM. Study predetermined inclusion/exclusion criteria, outcomes, and statistical analysis parameters. The detailed search strategy is depicted in the Supplementary material.
Data extraction
Three reviewers (Y.L., Y.M.X., and Z.P.Z.) independently conducted the search, screened eligible studies, and extracted information about the study types, demographic characteristics, TTM therapeutic procedures, neurological outcomes, adverse events, and mortality. When disagreement occurred, a fourth reviewer (G.F.) assessed the literature and agreement was reached by consensus.
The following data were extracted from the selected articles: the first author’s name, year of publication, country, study design, study duration, the number of research institutes, sample size, TTM methods, target temperature, rewarming rate, location of temperature measurement, start timing of TTM, duration of TTM, time to reach target temperature, follow-up time, mortality, adverse events, and neurological outcomes.
Quality and bias assessment
Every included study underwent quality assessment with the methodological index for non-randomized studies (MINORS), containing 12 items and a global score of 24 points. A higher score indicates a better quality of primary study (Slim et al., 2003). The detailed quality assessment is depicted in Supplementary Table S1.
Outcomes
The primary endpoint was an unfavorable outcome at the last follow-up. The secondary endpoints were all-cause mortality, DCI, CVS, and adverse events. The unfavorable outcome was defined by a modified Rankin scale (mRS) of 4–6 (van Swieten et al., 1988) or the corresponding manifestation described in the primary articles. DCI was defined as the presence of focal neurological deterioration or a decrease in the Glasgow Coma Scale of at least two points and an infarction on the Computed tomography (CT) or Magnetic resonance imagining (MRI) scan that was not visible at admission or immediately following treatment (Won et al., 2022). Severe CVS was suspected when TCD velocities were >200 cm/s in the middle cerebral artery or 85 cm/s in the basilar artery (Park et al., 2021). Cardiac problems include bradycardia, tachycardia, myocardial infarction, and arrhythmia (Won et al., 2022). Electrolyte imbalance was defined as hypokalemia (potassium < 3.5 mmol/L), hyponatremia (sodium < 135 mmol/L), and hyperkalemia (potassium > 5.5 mmol/L). Pneumonia was defined as a positive chest radiograph, new purulent symptoms of at least one acute infection (temperature > 38°C, White blood cell count < 4 × 109/L or >12 × 109/L), and at least two symptoms, worsening symptoms, dry and wet rales (Kwon and Choi, 2017). In addition, adverse events were verified by the methods described in the primary articles.
Statistical analysis
Statistical analyses were conducted using Stata 17.0 (Stata Corp, College Station, TX, USA). The median was calculated for the continuity data. To evaluate the clinical efficacy of TTM, relative risks (RRs) with 95% confidence intervals (CIs) were used. The I2 statistic was applied for the analysis owing to the heterogeneity. The values of p < 0.05 or I2 value >50% indicated heterogeneity, and its origin was taken into consideration. In cases of significant heterogeneity, the random-effects model was used for the meta-analysis; otherwise, the fixed-effects model was applied. Subgroup analyses were performed based on predefined variables to identify possible sources of heterogeneity. A sensitivity analysis was conducted for each subgroup to assess the robustness of the results. The sensitivity analysis involved removing one study at a time and examining the resulting changes in pooled RRs. Publication bias severity was evaluated using Egger’s and Begg’s tests. Statistically significant results were determined using a two-tailed p-value < 0.05. If publication bias was present, the trim and fill method was used.
Results
Literature search
Our search initially identified 1081 articles. After removing duplicate literature, a total of 793 articles were found. Out of these, 748 articles were discarded due to their irrelevant titles and abstracts. Forty-five full-text articles were then assessed for eligibility, and from these, 40 published articles were excluded for various reasons. These reasons included the absence of a control group, patients with combined ischemic and hemorrhagic stroke, unclear clinical outcomes, or lack of relevant data. Finally, a total of five studies were included in our analysis. The detailed search procedure is illustrated in Figure 1.
Characteristics of included studies
Characteristics of the included studies are listed in Table 1. A total of four studies were included, consisting of one randomized controlled study and three retrospective and prospective studies. The studies were conducted in Korea (three studies), Japan (one study), and Germany (one study). One of the studies involved multiple centers. The data from 219 patients were recorded across these studies (Anei et al., 2010; Kuramatsu et al., 2015; Kwon and Choi, 2017; Rhim et al., 2022; Seule et al., 2009; Won et al., 2022). Since MINORS is derived from the randomized study quality assessment method, we used it to evaluate the quality of both randomized studies and observational studies. All five articles received higher scores, indicating a good or moderate level of evidence (Supplementary Table S1). Table 2 presents the characteristics of the TTM in the included studies. The cooling and rewarming processes varied among the different studies. Temperature measurements were taken at various locations, including the bladder, jugular vein, and esophagus. The timing of TTM initiation also varied, with intervals ranging from <8 hours to >48 hours. Two studies used the endovascular cooling method, two studies used the body surface cooling method, and one study used a combination of body surface hypothermia and endovascular cooling. The target temperature for all studies was set at 33–35°C. The cooling maintenance period for TTM ranged from >48 hours in three studies, 5 days in one study, and even 6–8 days in one study. As for rewarming rates, four studies had a rate of 0.5°C/12 h, while one study had a rate of 0.5°C/24 h. Only two studies mentioned the time taken to reach the target temperature, both being <1 hour (Table 2).
Characteristics of Selected Studies
MINORS, methodological index for non-randomized studies; mRS, modified Rankin scale; NA, not available; RCT, randomized controlled trial; TTM, target temperature management.
Cooling Characteristics of Included Studies
NA, not available.
Primary endpoint: unfavorable outcome
The effect of TTM on unfavorable outcomes was evaluated in all five studies. The meta-analysis using a random-effects model indicated that the TTM group did not significantly reduce unfavorable outcomes compared with the control group (RR = 0.94, 95% CI: 0.71–1.26; p = 0.702; Fig. 2a). There was significant heterogeneity observed (I2 = 70.8%; Pheterogeneity = 0.008; Fig. 2a). Further examination of the L’Abbe and Galbraith plots revealed that studies on unfavorable outcomes showed moderate heterogeneity (Supplementary Fig. S2a; Supplementary Fig. S3a). Sensitivity analysis for unfavorable outcomes did not identify any study with a major impact on heterogeneity (Supplementary Fig. S4a). Subgroup analysis of unfavorable outcomes based on country, study type, follow-up time, TTM methods, TTM cooling maintenance period, and rewarming rate demonstrated high heterogeneity within each subgroup, suggesting that these factors could not explain the source of heterogeneity (Fig. 3; Table 3).
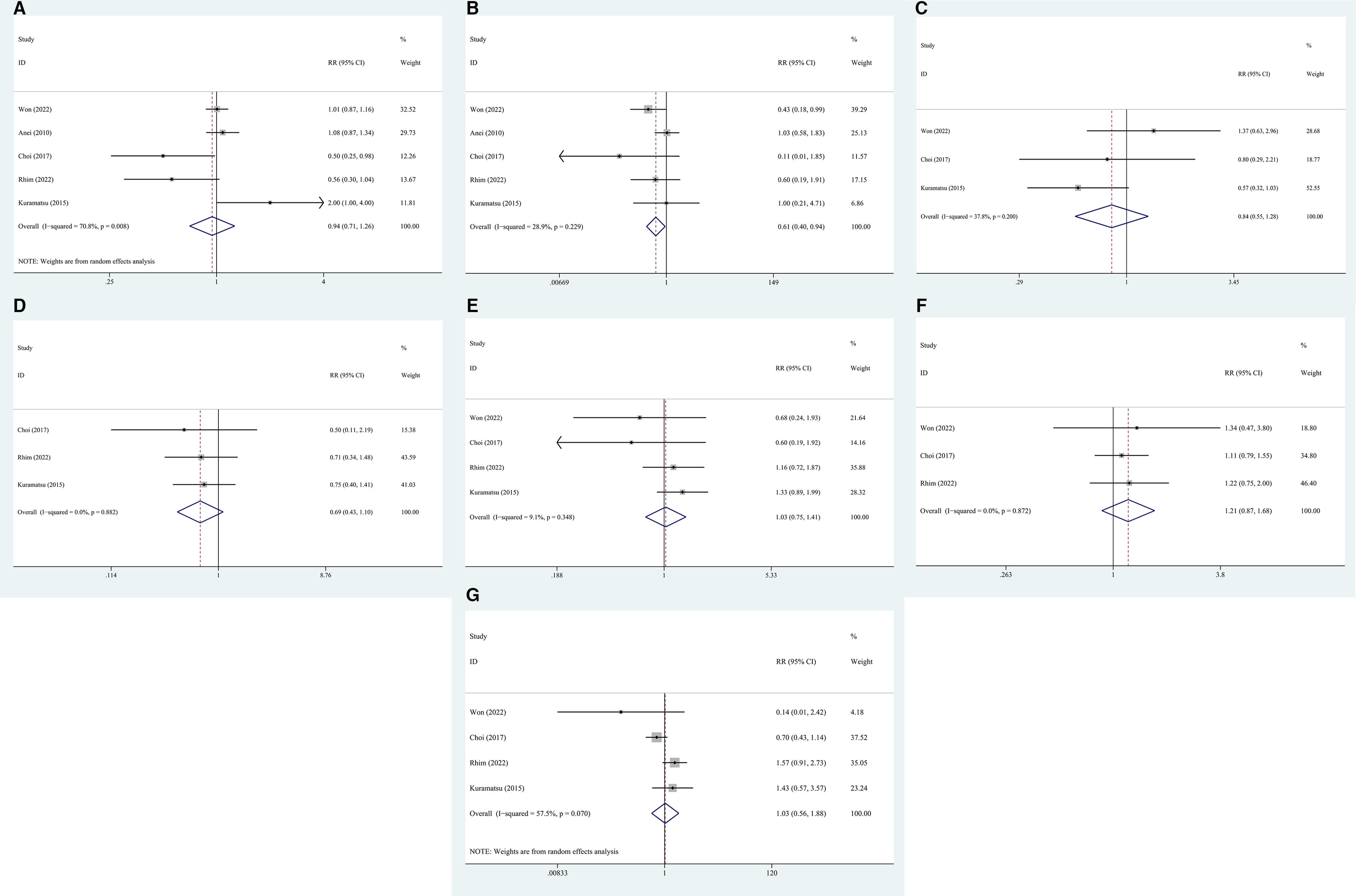
Forest plot of the RR for unfavorable outcomes and complications in patients with TTM versus controls. RR of
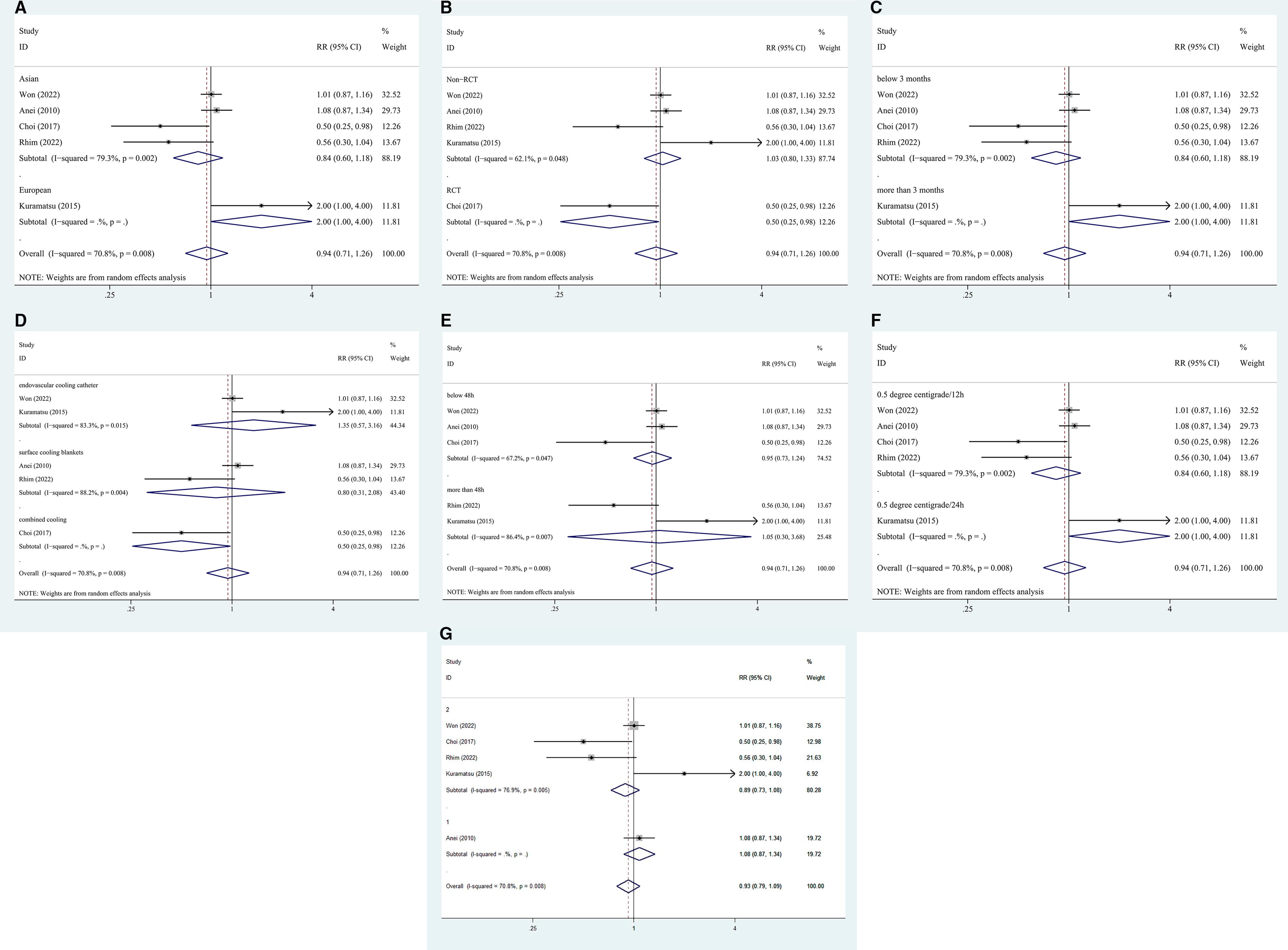
Subgroup analysis. Forest plot of the RR for unfavorable outcome in patients with TTM versus controls. RR of unfavorable outcome at follow-up stratified by
Subgroup Analyses Stratified by Country, Type of Study, Follow-Up Time, Target Temperature Management Methods, Target Temperature Management Cooling Maintenance Period, Rewarming Rate, and Start Time
CI, confidence interval; N, number of studies; RR, risk ratio.
Mortality
All five studies assessed the impact of TTM on mortality. There was no significant heterogeneity observed (I2 = 28.9%; Pheterogeneity = 0.229). A fixed-effect model was employed to determine the effect size (RR = 0.61, 95% CI: 0.40–0.94; p = 0.026; Fig. 2b), indicating that TTM significantly reduced mortality. Furthermore, a sensitivity analysis conducted by removing one study at a time demonstrated that none of the studies had a significant impact on the overall effect (Supplementary Fig. S4b).
Adverse events
Three studies compared the incidence of DCI in the TTM groups and the control groups. No significant heterogeneity was observed (I2 = 37.8%; Pheterogeneity = 0.200). A fixed-effect model was used to calculate the effect size (RR = 0.84, 95% CI: 0.55–1.29, p = 0.426; Fig. 2c), indicating that there was no significant difference between the two groups. A leave-one-out sensitivity analysis showed that no individual study significantly influenced the overall effect (Supplementary Fig. S4c).
Three studies compared the incidence of CVS events in the TTM and control groups. No significant heterogeneity was observed (I2 = 0.0%; Pheterogeneity = 0.882). A fixed-effect model was used to calculate the effect size (RR = 0.69, 95% CI: 0.44–1.10, p = 0.121; Fig. 2d), suggesting that there was no significant difference between the two groups. A leave-one-out sensitivity analysis showed that no individual study significantly influenced the overall effect (Supplementary Fig. S4d).
Four studies compared the incidence of pneumonia in the TTM group and the control group. The heterogeneity test showed I2 = 9.1% with little heterogeneity, and a fixed-effect model was used to calculate the effect size (RR = 1.03, 95% CI: 0.75–1.41, p = 0.874; Fig. 2e), indicating that there was no significant difference between the two groups. A leave-one-out sensitivity analysis showed that no individual study significantly influenced the overall effect (Supplementary Fig. S4e).
Three studies evaluated the incidence of electrolyte disturbances in both groups. The heterogeneity test showed I2 = 0%, and a fixed-effect model was used to calculate the effect size (RR = 1.21, 95% CI: 0.87–1.68, p = 0.263; Fig. 2f), indicating that there was no significant difference between the two groups. A sensitivity analysis showed that no individual study significantly influenced the overall effect size when each study was excluded individually (Supplementary Fig. S4f).
Four studies compared the incidence of cardiac complications in the TTM group with the control group. Significant heterogeneity was observed (I2 = 57.5%, Pheterogeneity = 0.07). Further examination of the L’Abbe and Galbraith plots revealed moderate heterogeneity in studies of cardiac complications. Meta-analysis using a random-effects model found no significant differences between the two groups (RR = 1.03, 95% CI: 0.56–1.88; p = 0.933; Fig. 2g). Sensitivity analysis, excluding Choi 2017, showed a pooled effect (RR = 1.18, 95% CI: 0.74–1.90, p = 0.490, I2 = 39.8%; Supplementary Fig. S5a). Similarly, excluding Rhim 2022 by sensitivity analysis showed a combined effect (RR = 0.74, 95% CI: 0.46–1.22, p = 0.238, I2 = 39.8%; Supplementary Fig. S5b). Subgroup analysis of unfavorable outcomes based on country, study type, follow-up time, TTM methods, TTM cooling maintenance period, and rewarming rate showed high heterogeneity in each subgroup, indicating that these factors could not explain the source of heterogeneity (Fig. 4; Table 3).
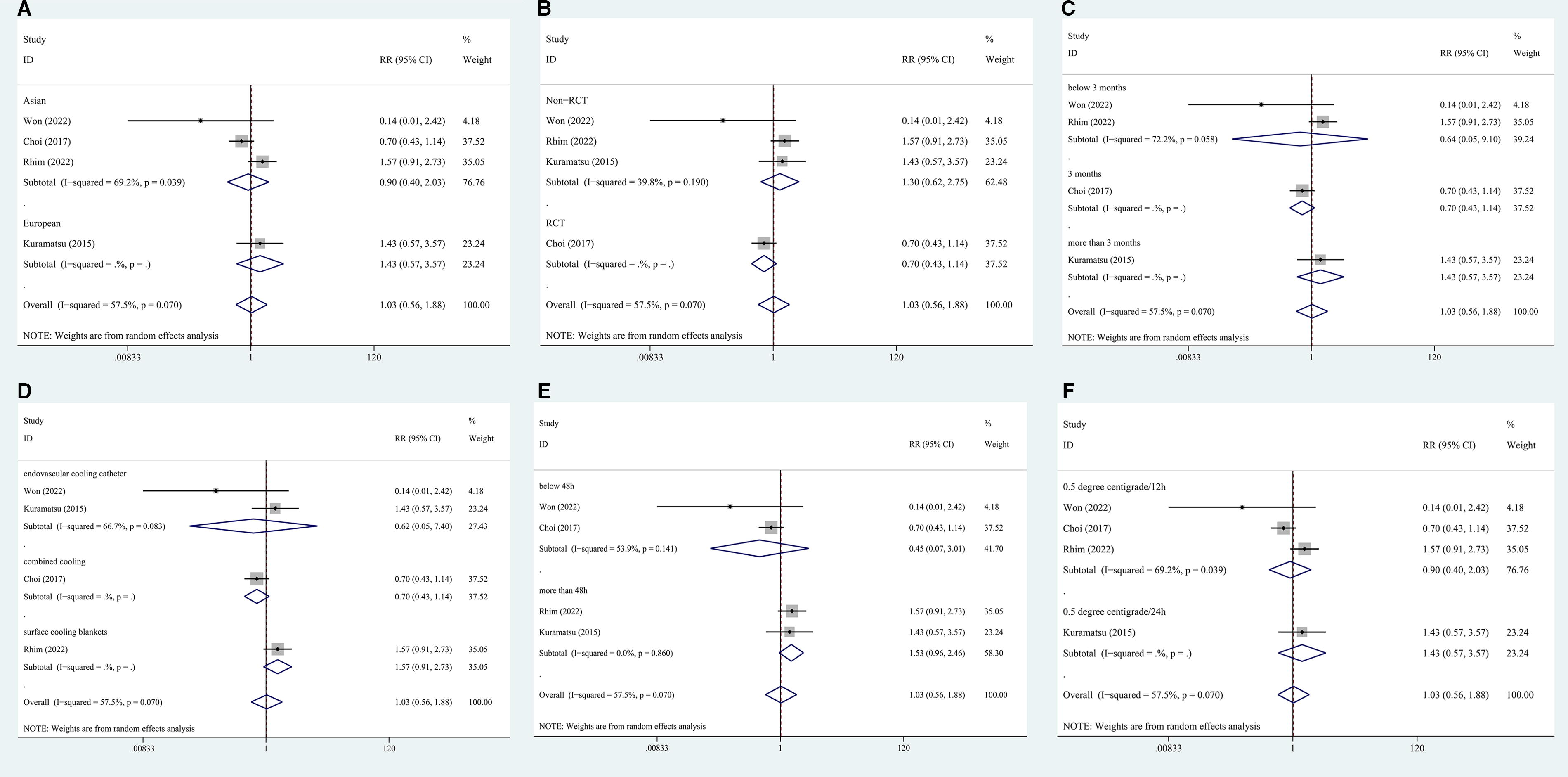
Subgroup analysis. Forest plot of the RR for cardiac complications in patients with TTM versus controls. RR of cardiac complications at follow-up stratified by
Publication bias
No significant publication bias was found for evaluating the effects of TTM on unfavorable outcomes (Begg’s test: Z = −0.24, p = 1.00; Egger’s test: t = −0.52, p = 0.64; Supplementary Fig. S1a; Supplementary Fig. S7a; Supplementary Fig. S6a) or mortality (Begg’s test: Z = 0.24, p = 0.81; Egger’s test: t = −1.37, p = 0.27; Supplementary Fig. S1b; Supplementary Fig. S7b; Supplementary Fig. S6b) or on DCI (Begg’s test: Z = 0.00, p = 1.00; Egger’s test: t = 0.61, p = 0.65; Supplementary Fig. S1c; Supplementary Fig. S7c; Supplementary Fig. S6c) or electrolyte imbalance (Begg’s test: Z = 1.04, p = 0.30; Egger’s test: t = 2.27, p = 0.27; Supplementary Fig. S1f; Supplementary Fig. S7f; Supplementary Fig. S6f) and Cardiac problem (Begg’s test: Z = −0.34, p = 1.00; Egger’s test: t = −0.37, p = 0.75; Supplementary Fig. S1g; Supplementary Fig. S7g; Supplementary Fig. S6g). But significant publication bias was found in CVS (Begg’s test: Z = 1.04, p = 0.30; Egger’s test: t = −24.84, p = 0.03; Supplementary Fig. S1d; Supplementary Fig. S7d; Supplementary Fig. S6d) and pneumonia (Begg’s test: Z = 1.70, p = 0.09; Egger’s test: t = −12.63, p = 0.01; Supplementary Fig. S1e; Supplementary Fig. S7e; Supplementary Fig. S6e). The asymmetry of CVS and pneumonia funnel plots are analyzed by the trim and fill method, and the results are still not statistically significant, and the combined results are stable (Supplementary Fig. S8).
Discussion
In this review, the overall effect of the study showed that TTM did not have a clear advantage in reducing adverse outcomes compared with the control group. However, it did significantly reduce mortality. This suggests that while TTM may not improve overall outcomes, it does have a significant impact on reducing the risk of death. We think that when aneurysm rupture and bleeding cause severe brain damage, initiating TTM as soon as possible after early surgery is the reason for reducing mortality. Preoperative TTM may cause patients to miss the opportunity for surgery, although it temporarily protects the brain. Subgroup analysis, which was stratified according to specific treatment parameters, did not identify any factors contributing to improved poor outcomes with TTM. However, randomized controlled studies and the use of combined cooling techniques did show a notable reduction in adverse outcomes. RCTs are effective in eliminating confounding factors and ensuring study quality. However, caution must be exercised when interpreting the results due to the inclusion of studies with small sample sizes. The jugular vein is commonly used as a core temperature measurement site for TTM. Previous studies have shown that endovascular cooling can quickly induce hypothermia and maintain temperature stability. However, there are potential adverse events associated with this method, such as infection, bleeding at the catheter site, and deep vein thrombosis. To mitigate these risks, alternative temperature measurement sites with similar diagnostic values, such as the bladder and esophagus, are used instead. Surface cooling techniques are safe and effective, but they may not be as rapid in inducing hypothermia compared with the intravascular cooling method. Clinical studies that combine both endovascular cooling and body surface cooling provide valuable evidence for the effectiveness of TTM in managing targeted temperature levels (Annoni et al., 2020; Badjatia et al., 2010; Keller et al., 2003; Mayer et al., 2004).
No previous reviews have been published regarding the use of TTM for the treatment of poor-grade aSAH. However, when comparing our results with previous reviews on the use of hypothermia for hemorrhagic stroke, we found that poor-grade aSAH patients treated with TTM had lower mortality rates and improved prognosis. The reason for this difference may be attributed to the fact that hemorrhagic stroke encompasses different types, such as intracerebral hemorrhage and SAH, and the previous review included patients with varying degrees of SAH severity (Yao et al., 2018). It is worth noting that our review did not include any studies examining the use of intraoperative hypothermia. This is because the short duration of intraoperative hypothermia was found to have a minimal impact on postoperative CVS and DCI (Li et al., 2016; Todd et al., 2005). Additionally, there are currently no clinical trials investigating the use of intraoperative TTM in poor-grade aSAH patients.
Currently, there are no established guidelines regarding the timing and duration of TTM in poor-grade aSAH patients. However, in theory, TTM therapy should be initiated as early as possible after the rupture of the aneurysm and continued throughout the entire period of early brain injury. Early initiation of TTM has been shown to have potential benefits in reducing brain damage and improving neurological outcomes. It is important to note that the duration of TTM should be carefully considered. Short-course TTM may not cover the critical peak times of CVS and DCI, which often occur after 72 hours (Okazaki and Kuroda, 2018). The studies reviewed in this context had a range of durations, with three studies implementing TTM for 48 hours and two studies extending it beyond that. However, an excessive duration may lead to a higher complication rate. Inadequate rewarming rates can lead to systemic vasodilation, hypotension, cerebral vasodilation, and rebound edema, resulting in increased intracranial pressure. Conversely, excessively slow rewarming rates may cause excessive hypothermia and its associated complications (Kobata et al., 2022). Currently, there is no consensus on the optimal rewarming rate and duration of TTM in poor-grade aSAH patients, although clinical studies typically use rewarming protocols of 0.5°C/12 h or 0.5°C/24 h. Further research and evidence are required to establish guidelines in this area.
The adverse reactions of TTM mainly include chills, infection, cardiac complications, electrolyte disorders, and abnormal coagulation function, with pneumonia being the most common complication. A review found that complication rates were comparable in the control and TTM groups, and there was no higher risk of any specific complication. In a study by Kuramatsu et al. (2015), out of 12 patients in the hypothermia group, 10 developed pneumonia after treatment (Kuramatsu et al., 2015). This could be attributed to age, underlying diseases weakened immune system function, and the use of sedative and analgesic drugs that suppress breathing and decrease airway protection, ultimately leading to impaired cough function and a significantly higher incidence of pneumonia. However, another study by Kwon and Choi demonstrated that optimizing the duration of hypothermia therapy with a continuously optimized TTM regimen reduced the incidence of pneumonia (Kwon and Choi, 2017).
There are several limitations to consider in this meta-analysis. Firstly, only 5 studies with a small sample size of 219 individuals were analyzed, which prevented further subgroup analysis. Secondly, the TTM regimen and the standard treatment regimen differed. Thirdly, non-English language and unpublished studies were not included, which may affect the validity of the findings. In addition, pneumonia frequently occurs in individuals with poor-grade aSAH, making it challenging to accurately assess the specific effects of TTM, due to insufficient information regarding the severity and progression of pneumonia exacerbation. However, our meta-analysis is currently the only comprehensive analysis of the efficacy of TTM in patients with poor-grade aSAH. It is important to note that due to the limited number of studies and the potential bias in observational studies, well-designed randomized trials are needed to confirm these results. Despite showing promising results in animal models of SAH, the clinical use of TTM did not demonstrate a significant reduction in unfavorable outcomes. However, based on the limited evidence available, TTM has been found to significantly reduce mortality rates. Additionally, the incidence of complications such as pneumonia, cardiac complications, and electrolyte disturbances was similar between the TTM group and the control group.
Footnotes
Authors’ Contributions
Y.L. and G.F. conceived and designed the study, drafted the article, and critically revised the article. Y.L., M.Y.X., and P.Z.Z. designed the study and collected, analyzed, and interpreted the data. Y.L., M.Y.X., and P.Z.Z. collected the data and reviewed the literature. All authors read and approved the final article.
Author Disclosure Statement
The authors declared no conflict of interest.
Funding Information
Henan Provincial Health and Wellness Commission’s Youth Project (No.: SBGJ202003008).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.