
Abstract
Malignant hyperthermia (MH) is a rare, life-threatening condition caused by alterations in skeletal muscle calcium channels inherited through an autosomal dominant pattern. The use of specific agents in anesthesia such as inhaled anesthetics and succinylcholine can precipitate a hyperthermic crisis. Patients experience a rapid increase in muscle rigidity, secondary to skeletal muscle calcium dysregulation, leading to acute rhabdomyolysis and possible hyperthermia. Providers must have a high index of suspicion of this disease process because early diagnosis is critical to mortality reduction. Management centers around removal of the offending agent, dantrolene, and supportive care including cooling if hyperthermic. Intravascular cooling devices have been used in thermodynamic regulation after cardiac arrest and have shown to be more effective than dermal cooling techniques; however, they have not been well described in other disease processes. The following case report is the first to describe a patient suffering from MH to undergo invasive intravenous cooling in order to counteract the effects of this life-threatening disease.
Introduction
Malignant hyperthermia (MH) is a life-threatening, autosomal dominant inherited myopathy characterized by a hypermetabolic state with rapid muscle breakdown. The etiology is a defect in the ryanodine receptor, a calcium-release channel. MH occurs when patients are exposed to a specific triggering agent including inhaled anesthetics and succinylcholine. It is characterized by a marked increase in temperature that remains elevated, increasing end-tidal carbon dioxide (EtCO2), muscle rigidity, and rhabdomyolysis. If left untreated, mortality rates approach 70%. Early diagnosis and the use of dantrolene have reduced this risk to less than 5% (Rosero et al., 2009). Additionally active cooling is paramount to the treatment of recognized MH.
Case Description
A 29-year-old male, with no reported past medical history, presented to the emergency department with a chief complaint of sore throat for 5 days. His temperature was 37.2°C, heart rate was 124 beats per minute (bpm), and blood pressure was 123/82. The patient was unable to phonate and was found to have significant submental induration and tenderness with an elevated tongue. Computed tomography of the patient’s soft tissue neck demonstrated a large abscess consistent with the findings of Ludwig’s angina (Fig. 1). The patient was started on intravenous antibiotics and an otolaryngologist was consulted. After consultation, the patient was recommended surgery for incision and drainage of abscess. Due to capacity constraints in the operating room and the nature of the patient disease process, it was recommended that the patient undergoes urgent airway management while in the emergency department. A nasopharyngeal intubation was performed with a 6-0 endotracheal tube using a fiber optic scope with 100 mg of intravenous ketamine and 150 mg of succinylcholine without incident. The patient was started on fentanyl and propofol for postintubation sedation. Approximately 30 minutes after intubation, the patient’s nurse noted that the patient’s tachycardia had increased from 122 bpm to 154 bpm and the temperature had increased from 37.2°C (98.9°F) to 40°C (104°F); EtCO2 was noted to be increasing to the 60s with notable increased tachypnea over set ventilator rate. The patient was displaying muscle rigidity, and the medical team was unable to pass oral-gastric tube due to severity of the patient’s masseter muscle spasm. Urine was noted to be darkening in the Foley bag. Labs from that time revealed a mildly elevated creatinine kinase 116 units/L. Venous blood gas sampling revealed a pH of 7.28, pCO2 of 55, and HCO3 of 24. Because the patient received succinylcholine for intubation, a presumptive diagnosis of MH was made. The patient was given 175 mg of dantrolene, 2 L of cooled intravenous fluids, and 150 mg of sodium bicarbonate. The ventilator heater was discontinued and active external cooling of the patient was initiated with ice packs placed in the groin and axilla. The patient’s temperature continued to climb to 41.4°C (106.6°F) (Fig. 2). The decision was made to place a right femoral cooling catheter (ZOLL Quatro® Thermoguard XP™) for targeted temperature management (TTM) to normothermia with a goal of 37.8°C (100.4°F). Once the patient was stabilized, he was admitted to the surgical intensive care unit for further management. He later went to the operating room with ENT for abscess drainage and source control. The intravascular cooling device was discounted 24 hours after it was initiated and the patient was extubated after 3 days without any residual neurological deficit or renal dysfunction. Succinylcholine and inhaled anesthetics were added to the patient’s allergy list and was counseled on family risk and future risk of occurrence.

Computed tomography (CT) of soft tissue neck noting soft tissue swelling, discrete abscess, and air concerning for Ludwig’s angina.
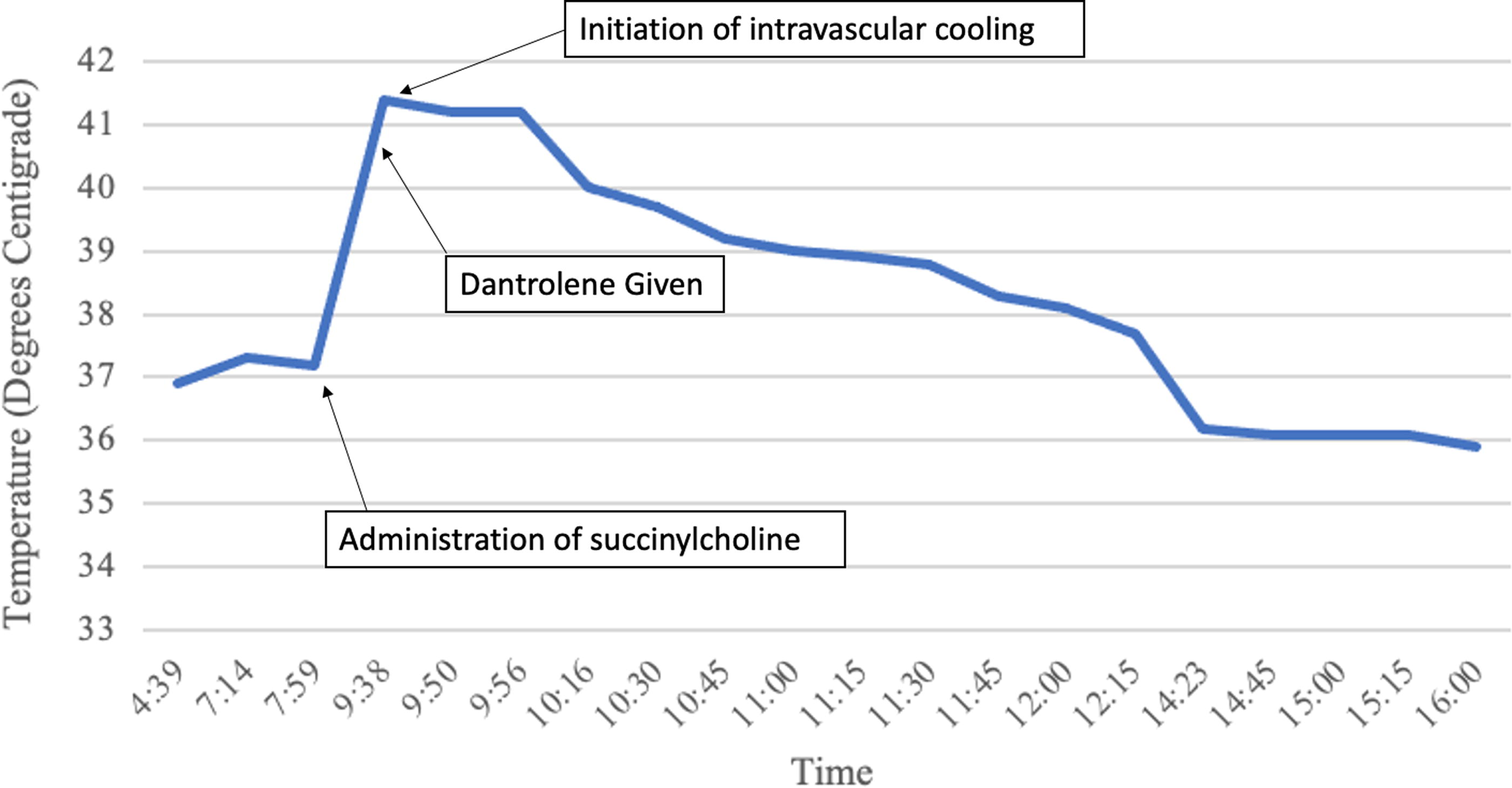
Line graph showing patient’s temperature prior to succinylcholine administration, his rapid development of hyperthermia, and correction with intravascular cooling device.
Discussion
MH is a rare life-threatening condition that requires prompt recognition and aggressive management. While the pathology of MH is not fully understood, signs most patient will exhibit changes from their preintubation vital signs such a tachycardia, increased EtCO2, and a rapid rise in core body temperature. In addition to supportive measures of crystalloid fluid administration, removing potential offending agents, and passive cooling measure, it is recommended to administer dantrolene if available. The mechanism of action of dantrolene helps stop muscle contraction by binding to ryanodine receptors and blocking further calcium release. Our patient had received dantrolene and passive cooling measures had been initiated. The offending agent could not be discontinued or reversed. His temperature continued to climb. Current guidelines for the management of MH recommend active internal cooling measures such as thoracic cavity or peritoneal packing with ice, but these patients are typically presenting in the operating room with an open cavity (Litman et al., 2019). This option was not available to us as our patient had no open cavity. It was decided that our quickest way to actively cool our patient was with the utilization of a cooling catheter (ZOLL Quatro Thermoguard XP) typically used for TTM after cardiac arrest. The use of intravascular cooling devices has shown to more effectively and rapidly bring a patient to the desired temperature faster than traditional cooling techniques (Rosman et al., 2018). During TTM for postcardiac arrest care, Rosman et al. were able to achieve a cooling rate (−0.66 ± 0.35°C/h). Reviewing the temperature curve in Figure 2, it clearly demonstrates the effectiveness of intravascular cooling in regard to core temperature control reaching the goal in 2 hours (1.75°C/h). To our knowledge, this has not been described elsewhere in the literature, but we do believe this to be an effective way to cool patients with MH when temperatures continue to climb despite other aggressive measures. We suggest that cooling catheters are an appropriate and potential life-saving intervention for patients who develop MH.
Footnotes
Authors’ Contributions
B.V.S.: conceptualization, data curation, writing—original draft, writing—review and editing, and supervision. B.J.G.: conceptualization, data curation, writing—original draft, writing—review and editing, and supervision.
Author Disclosure Statement
No conflicts of interest to disclose.
Funding Information
No funding was received for this article.