
Abstract
There are no studies examining the association between rewarming durations and neurological outcomes after extracorporeal cardiopulmonary resuscitation (ECPR) followed by targeted temperature management (TTM) for patients with out-of-hospital cardiac arrest (OHCA). This study aimed to examine the association between rewarming durations and neurological outcomes after ECPR with TTM for patients with OHCA. This was a secondary analysis of the Advanced Life Support Study Registry for Ventricular Fibrillation with Extracorporeal Circulation in Japan study, a retrospective, multicenter study. Patients with OHCA who underwent ECPR and completed a TTM of 34°C and <34°C were included. Favorable neurological outcomes (cerebral performance categories 1–2) and survival upon hospital discharge were the primary outcomes. In total, 407 patients were included, with favorable neurological outcomes upon hospital discharge in 106 patients. The numbers of patients with rewarming durations of <24 hours, 24 hours, and >24 hours were 178, 133, and 96, respectively. In the multivariable analysis, a rewarming duration of <24 hours was not significantly associated with favorable neurological outcomes [odds ratio (OR): 1.06, 95% confidence interval (CI): 0.60–1.87, p = 0.84] or survival (OR: 0.96, 95% CI: 0.58–1.57, p = 0.86) compared with that of 24 hours, and that of <24 hours was not significantly associated with favorable neurological outcomes (OR: 0.74, 95% CI: 0.40–1.71, p = 0.56) or survival (OR: 0.74, 95% CI: 0.42–1.28, p = 0.38) than that of >24 hours. A rewarming duration of <24 hours in TTM after ECPR for OHCA was not significantly associated with favorable neurological outcomes or survival than that of 24 hours or >24 hours.
Introduction
A meta-analysis of four randomized trials comparing extracorporeal cardiopulmonary resuscitation (ECPR) with conventional cardiopulmonary resuscitation (CCPR) for patients with out-of-hospital cardiac arrest (OHCA) was recently published, which concluded that ECPR compared with CCPR increased survival with favorable neurological outcomes in patients with OHCA with an initial shockable rhythm (Belohlavek et al., 2022; Hsu et al., 2021; Scquizzato et al., 2023; Suverein et al., 2023; Yannopoulos et al., 2020). Especially, the ARREST trial, which demonstrated the remarkable efficacy of ECPR, involved targeted temperature management (TTM) with a target temperature of 34°C for 24 hours (Yannopoulos et al., 2020).
TTM with mild hypothermia generally comprised three phases; the induction, maintenance, and rewarming phases (Fukuda, 2016). Regarding the rewarming phase, the ERC-ESICM guidelines published in 2021 provided no recommendation concerning the rate of rewarming for post-CA temperature control due to the lack of strong (reliable) evidence (Nolan et al., 2021). Furthermore, the optimal rate of rewarming was identified as a knowledge gap in the AHA guideline (Panchal et al., 2020). To the best of our knowledge, there are no studies examining the association between the rewarming duration and neurological outcomes after ECPR with TTM for patients with OHCA.
Thus, this study aimed to examine the association between the rewarming duration and neurological outcomes after ECPR with TTM for patients with OHCA.
Methods
The SAVE-J II study
The present study was conducted using data from the Advanced Life Support Study Registry for Ventricular Fibrillation with Extracorporeal Circulation in Japan (SAVE-J II), which contains data from 36 participating institutions in Japan between January 1, 2013, and December 31, 2018. The medical records of 2157 patients who underwent ECPR using venoarterial extracorporeal membrane oxygenation (VA-ECMO) after OHCA were included in the registry. The SAVE-J II study was registered in the Clinical Trials Registry of the University Hospital Medical Information Network and the Japanese Clinical Trial Registry (registration number: UMIN000036490), and it was approved by the institutional review board of Kagawa University (approval number: 2018–110). The study was also approved by the Institutional Ethics Committee of St. Luke’s International Hospital (approval number: 18-R188). The requirement for participants’ informed consent was waived due to the retrospective nature of this study.
Study design and participants
This was a secondary analysis of the SAVE-J II study. We included patients with OHCA who underwent ECPR and completed a TTM of 34°C and <34°C in the participating institutions between January 1, 2013, and December 31, 2018. We excluded patients with noncardiogenic cardiac arrest, return of spontaneous circulation (ROSC), upon arrival at the hospital or at the time of ECMO initiation, incompletion of TTM, target temperatures of >34°C, and unknown rewarming durations. The secondary analysis of the deidentified data was approved by the institutional review board of St. Luke’s International Hospital (approval number: 22-R097).
Data collection
The following parameters were recorded for each study participant: age, sex, presence or absence of witnessed Cardiac Arrest (CA) and bystander cardiopulmonary resuscitation (CPR), initial rhythm (shockable or not), ROSC before arrival, estimated low flow time, pupil size at arrival (4 mm), presence of the light reflex at arrival, gasping at arrival, targeted temperature of rewarming, TTM-associated complications, hospitalization days, number of days of intensive care unit (ICU) stay of survivors, number of days of hospitalization of survivors, time of death, survival and neurological outcomes at the time of hospital discharge, and complications (overcooling, electrolyte disturbance, arrhythmia, and others).
Outcome measures
The primary outcomes were favorable neurological outcomes and survival at the time of hospital discharge. A favorable neurological outcome was defined as a cerebral performance category (CPC) of 1 or 2, while an unfavorable neurological outcome was defined as a CPC of 3, 4, or 5 (Bertic et al., 2022). The secondary outcomes were the number of days of hospitalization of survivors, number of days of ICU admission for survivors, date of death, and TTM-associated complications, which included overcooling (<32°C), electrolyte disturbances [K (<3.0 mmol/L), Mg (<0.7 mmol/L), P (<0.7 mmol/L)], arrhythmia (decisions by the physician in charge), and others.
Statistical analysis
On the histogram, the group that completed rewarming at 24 hours was the most common. To compare the baseline characteristics of our study participants, we set the completion of rewarming at 24 hours as the reference point and divided patients as follows: <24 hours, 24 hours, and >24 hours. Baseline characteristics were compared using the Wilcoxon rank-sum test for continuous variables and the chi-square test for binary and categorical variables. Continuous variables are presented as medians and interquartile ranges, and categorical variables are presented as frequencies and percentages. Univariate and multivariable logistic regression analyses were performed for the primary endpoint. Multivariate analyses entailed adjustments for potential confounders [the initial rhythm (shockable), presence of witnessed CA and bystander CPR, sex, age (>65 years), estimated low flow time]. Odd ratios for the duration of the rewarming were presented according to the group of the duration of the rewarming. Furthermore, we repeated our statistical analyses after dividing the study participants into four groups using the quartiles of the rewarming rate (degree Celsius per hour). Statistical analyses were performed using JMP Version 12 statistical software (SAS Institute, Cary, NC). Participants with missing data were excluded from the analyses. A p value of < 0.05 was considered statistically significant.
Results
Of the 2157 adult patients who underwent ECPR and were enrolled in the SAVE-J II study registry, 9 were excluded due to the timing of the introduction of VA-ECMO, 1 was excluded because ECPR was discontinued after cannulation due to sustained ROSC, 342 were excluded because they suffered noncardiogenic cardiac arrest (119 were cases of acute aortic dissection or aortic aneurysm, 112 were cases of hypothermia, 51 were cases of primary cerebral disorders, 20 were infections, 14 were cases of drug intoxication, 11 were cases of trauma, 8 were cases of suffocation, 4 were cases of drowning, and 3 were cases with other external causes), 154 were excluded due to sustained ROSC before the commencement of ECPR (96 were commenced upon arrival at the hospital; 58 were commenced at the time of ECMO initiation), 323 were excluded due to the implementation of TTM, and 880 were excluded due to their targeted temperature (>34°C or unknown). In the end, 447 patients were eligible for this study. Of these 447, 40 were excluded because their rewarming durations were not available. Thus, 407 patients were ultimately included in our analysis (Fig. 1).
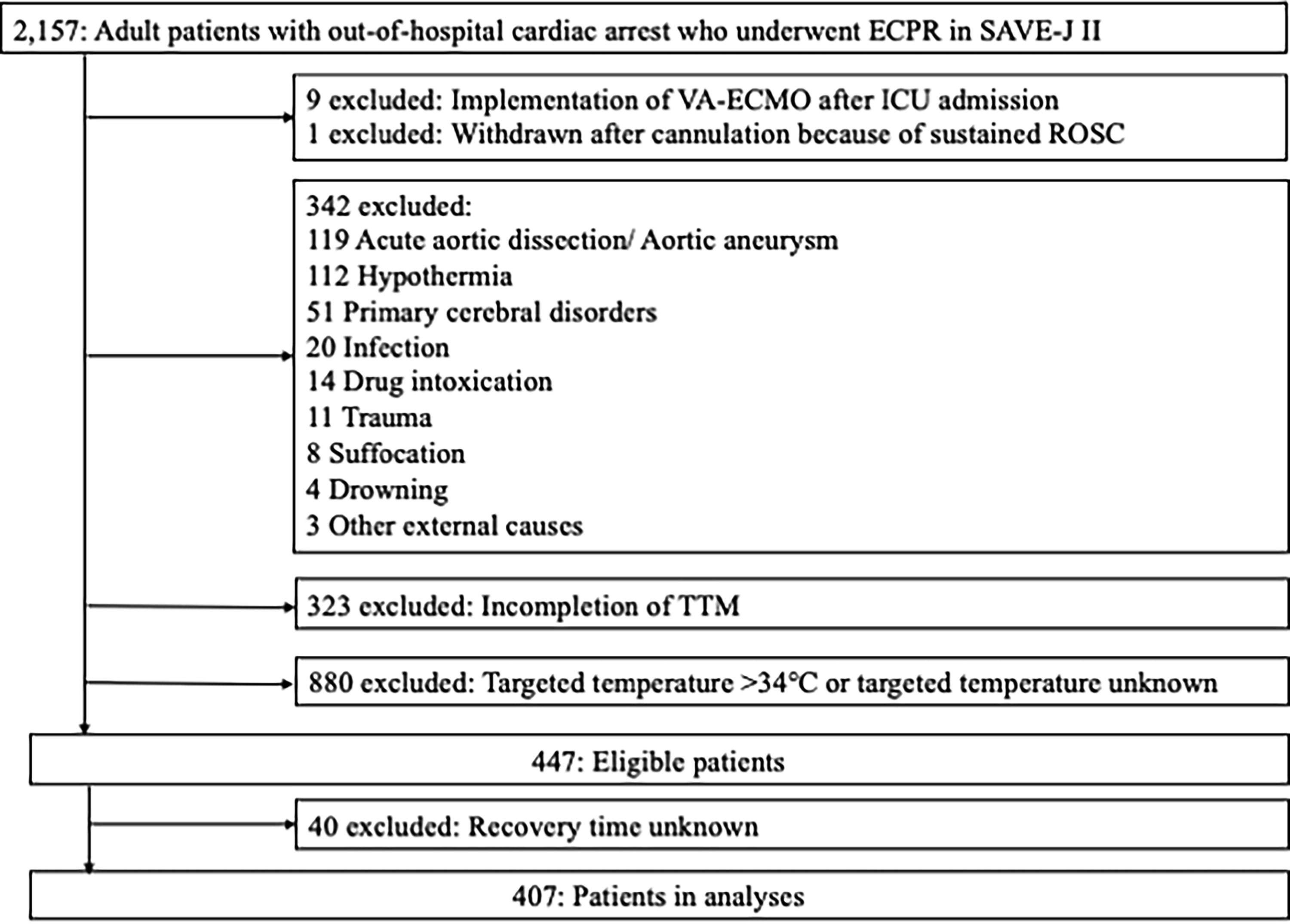
Flowchart of the participant enrollment process. ECMO, extracorporeal membrane oxygenation; ECPR, extracorporeal cardiopulmonary resuscitation; ICU intensive care unit; ROSC, return of spontaneous circulation.
Baseline characteristics of the study population
Overall, the median age was 58.0 years, and 85.0% of the patients were male. The median rewarming duration (until the target temperature of rewarming was attained) was 24 hours, and the temperatures of most of the study participants were set at 36°C (88.9%) (Table 1). Of the eligible patients, 106 (26.0%) had favorable neurological outcomes, and 211 (51.8%) were patients who survived at hospital discharge. The median hospital stay was 19 days, especially for patients who survived at the time of hospital discharge, with a median hospital stay of 34 days and a median hospital stay in the ICU of 12 days. The percentages of complications that could be inferred to be attributable to TTM were as follows: overcooling (2.7%), electrolyte disturbances (8.8%), arrhythmia (7.1%), and others (2.7%) (Table 1).
Baseline Characteristics and Outcome Data of Patients
Data are presented as the median [interquartile range] for continuous variables and N (percentage) for categorical variables.
The estimated low flow time was defined as the time from cardiac arrest to the establishment of ECMO if the cardiac arrest occurred in the ambulance and the time from calling an ambulance to the establishment of ECMO if the cardiac arrest did not occur in the ambulance.
CPC, cerebral performance category; CPR, cardiopulmonary resuscitation; ICU, intensive care unit; ROSC, return of spontaneous circulation; TTM, targeted temperature management.
Comparisons of baseline characteristics and outcomes of patients among the three groups (recovery time <24 hours, 24 hours, and >24 hours)
The baseline characteristics of patients with recovery durations of <24 hours, 24 hours, and >24 hours differed significantly in the presence of witnessed CA [<24 hours vs. >24 hours, odds ratio (OR): 1.93, 95% confidence interval (CI): 1.06–3.53, p = 0.03], estimated low flow time (<24 hours vs. >24 hours, OR: 0.75, 95% CI: 0.58–0.96, p = 0.02), and a higher target temperature of rewarming (>36.0°C, <37.6°C) (<24 hours vs. 24 hours, OR: 0.28, 95% CI: 0.13–0.62, p < 0.01) (Table 2).
Comparison of Baseline Characteristics of Patients According to the Rewarming Duration <24 Hours, 24 Hours, and >24 Hours
Data are presented as the median [interquartile range] for continuous variables and N (percentage) for categorical variables.
The estimated low flow time was defined as the time from cardiac arrest to the establishment of ECMO if the cardiac arrest occurred in the ambulance and the time from calling an ambulance to the establishment of ECMO if the cardiac arrest did not occur in the ambulance.
Estimated low flow time: the time from initiation of chest compressions to the establishment of ECPR.
CI, confidence interval; CPR, cardiopulmonary resuscitation; OR, odds ratio; ROSC, return of spontaneous circulation.
The outcomes of patients in the three groups (favorable neurological outcomes or survival at the time of discharge from the hospital) did not differ significantly; however, there were significant differences in the number of days of ICU stay of survivors (<24 hours vs. 24 hours, OR, 0.64; 95% CI: 0.47–0.89; p < 0.01, <24 hours vs. >24 hours, OR, 0.58; 95% CI: 0.40–0.83; p < 0.01) and the rate of complications with TTM (overcooling; <24 hours vs. >24 hours, p = 0.01, electrolyte disturbance; <24 hours vs. 24 hours, p < 0.01, and arrhythmia; <24 hours vs. 24 hours, p < 0.01) (Table 3) between these three groups of patients.
Comparison of Outcome According to Rewarming Duration <24 Hours, 24 Hours, and >24 Hours
Data are presented as the median [interquartile range] for continuous variables and N (percentage) for categorical variables.
CI, confidence interval; CPC, cerebral performance category; ICU, intensive care unit; OR, odds ratio; TTM, targeted temperature management.
The primary analysis
In the multivariable analysis, a rewarming duration of <24 hours was not significantly more associated with favorable neurological outcomes (OR: 1.02, 95% CI: 0.59–1.76, p = 0.96) or survival (OR: 0.86, 95% CI: 0.53–1.39, p = 0.54) than that of 24 hours, and a rewarming duration of <24 hours was not significantly more associated with favorable neurological outcomes (OR: 0.78, 95% CI: 0.42–1.44, p = 0.43) or survival (OR: 0.81, 95% CI: 0.47–1.39, p = 0.44) than that of >24 hours (Table 4).
Comparison of Unadjusted and Adjusted Associations with Favorable Outcomes (CPC 1 or 2) at Hospital Discharge and Survival to Hospital Discharge Between Rewarming Duration <24 Hours and 24 Hours and Between Rewarming Duration <24 Hours and >24 Hours
CI, confidence interval; CPC, cerebral performance category; OR, odds ratio.
The sensitivity analysis
Study participants were divided into four groups using the quartiles of the rewarming rate (°C/h) (N = 83 < 0.083, N = 105 > 0.083, ≤0.091, N = 152 > 0.091, ≤0.167, N = 61 > 0.167).
There were no statistically significant differences in primary outcomes or other outcomes, such as the length of hospital stay or TM-related complications, between patients with the rewarming rates. Only differences in the incidence of electrolyte disturbances were observed. However, the second-slowest group (>0.083 and ≤0.091) had the lowest incidence, while the second-fastest group (>0.091and ≤0.167) had the highest incidence, and there was no significant difference between the slowest (<0.083) and the fastest (>0.167) groups, resulting in inconsistent results (Table 5).
Comparison of Outcome and Complications of TTM According to Four Groups of Rewarming Rate (degree Celsius per hour)
Data are presented as the median [interquartile range] for continuous variables and N (percentage) for categorical variables.
CPC, cerebral performance category; ICU, intensive care unit; TTM, targeted temperature management.
Discussion
The results of the current study suggest that warming durations of <24 hours in TTM after ECPR for OHCA were not significantly associated with favorable neurological outcomes or survival. Also, longer warming durations did not reduce the rate of TTM-associated complications. Although no significant differences were observed, the duration of ICU stay tended to increase as the rate of rewarming was prolonged.
To the best of our knowledge, there is no study examining the warming duration in patients with OHCA receiving TTM after ECPR. Bouwes et al. retrospectively examined adult patients treated with TH after CA. In a univariate analysis, a high rewarming rate (0.5°C/h) was relatively associated with a higher risk of poor outcomes (OR: 2.61, 95% CI: 0.88–7.73, p = 0.08) (Bouwes et al., 2012). After adjustments for age and the initial rhythm, this association weakened (OR: 2.27, 95% CI: 0.69–7.46, p = 0.18). However, due to the small number of patients(N = 128) in this study and the factors adjusted for in the multivariate analysis, no firm conclusions could be drawn. In another study that included a relatively high number of adult patients with OHCA, Hifumi et al. retrospectively examined the rewarming duration [N = 328, in each rewarming group; N = 82 (<24 hours), N = 85 (≥24 hours, <44 hours), N = 80 (≥44 hours, <50 hours), N = 81(≥50 hours)] of those who underwent 34°C TTM in Japan. Multivariable analyses showed better neurological outcomes (OR: 0.89, 95% CI: 0.79–0.89, p = 0.032) and a higher survival discharge rate (OR: 0.85, 95% CI: 0.74–0.96, p = 0.012) with higher rewarming durations. However, the authors could not conclude why longer rewarming durations were associated with better outcomes and lower mortality rates, and survival bias may have strongly affected their conclusions (Hifumi et al., 2020). Thus, it is reasonable that the association between rewarming durations and outcomes, even in patients with CA without ECPR, remains unknown because of the paucity of studies on the rewarming duration. Our study had a limited number of patients who underwent ECPR; thus, patients with more severe conditions may have been included. Even in our study (which had patients in more severe conditions), slower rewarming did not improve clinical outcomes. One possible reason for this observation is that the treatment effect could not be observed due to the critical conditions of the included patients. Another possible reason is that rewarming durations may not have affected the clinical outcomes of patients who underwent both CCPR and ECPR.
Although no significant differences were observed, the duration of ICU stay tended to increase as rewarming was prolonged in this group of patients. Lascarrou et al. suggested that faster warming is unlikely to induce an exacerbation of systemic inflammation (Lascarrou et al., 2021), whereas a longer duration of TTM may lead to infections such as pneumonia, sepsis, and bacteremia (Nielsen et al., 2011). On the contrary, we could not examine the risk of outcomes and complications at different rewarming durations of <24 hours commonly used in Europe. Although this can shorten the ICU stay, it is also possible that rapid rewarming may lead to an increased rate of complications (Kim et al., 2010). Based on the results of this study, we suppose that it may be acceptable to complete rewarming within 24 hours since rewarming for >24 hours may not be beneficial. Avoiding an extended duration of rewarming beyond 24 hours may allow us to proceed to the next stage of treatment and examination. Further studies are expected to further subdivide the group of patients whose rewarming durations are <24 hours.
Limitations
Nevertheless, this study had several limitations. First, it was a retrospective study in which patients were not randomized. Second, the criteria for the induction of ECPR and the subsequent TTM protocol differed between centers. Selection bias may have occurred in each institution, affecting patient outcomes. Third, possible confounders, such as the quality of CPR and the prolonged time before CPR, were not considered due to the retrospective nature of this study. Fourth, the impact of faster rewarming was not examined in patients who were rewarmed within 24 hours. The variability in rewarming durations in patient groups was not consistent, which made it difficult to discuss the effect of much faster rewarming. Fifth, target temperature of rewarming was not a consistent value in the patient group in this study, and it remains possible that the target temperature of rewarming influenced the determination of the duration of rewarming. Sixth, although the present study focused on temperature control, there was no information on the devices used for TTM control. In particular, the degree of difficulty in TTM varied depending on the type of device used, and it is undeniable that this may have led to differences in complication (such as overcooling) rates. Finally, there were large data gaps regarding the length of hospital stay of survivors, the length of ICU stay of survivors, and the number of days of death. In particular, as mentioned above, the length of ICU stay of survivors tended to reduce with faster rewarming; however, about half of the data were lost, which means the actual results may differ.
Conclusions
In the setting of TH after ECPR for OHCA, rewarming durations of <24 hours were not significantly more associated with favorable neurological outcomes or survival than those of 24 hours or >24 hours in TTM after ECPR for OHCA. Future studies are expected to examine the appropriate rewarming duration and rate when recovery is performed within 24 hours.
Footnotes
Acknowledgments
The authors thank all members of the SAVE-J II study group who participated in this study: Hirotaka Sawano, MD, PhD (Osaka Saiseikai Senri Hospital); Yuko Egawa, MD, Shunichi Kato, MD (Saitama Red Cross Hospital); Kazuhiro Sugiyama, MD (Tokyo Metropolitan Bokutoh Hospital); Naofumi Bunya, MD, Take-hiko Kasai, MD (Sapporo Medical University); Shinichi Ijuin, MD, Shinichi Nakayama, MD, PhD (Hyogo Emergency Medical Center); Jun Kanda, MD, PhD, Seiya Kanou, MD (Teikyo University Hospital); Toru Takiguchi, MD, Shoji Yokobori, MD, PhD (Nippon Medical School); Hiroaki Takada, MD, Kazushige Inoue, MD (National Hospital Organization Disaster Medical Center); Ichiro Takeuchi, MD, PhD, Hiroshi Honzawa, MD (Yokohama City University Medical Center); Makoto Kobayashi, MD, PhD, Tomo-hiro Hamagami, MD (Toyooka Public Hospital); Wataru Takayama, MD, Yasuhiro Otomo, MD, PhD (Tokyo Medical and Dental University Hospital of Medicine); Kunihiko Maekawa, MD (Hokkaido University Hospital); Takafumi Shimizu, MD, Satoshi Nara, MD (Teine Keijinkai Hospital); Michitaka Nasu, MD, Kuniko Takahashi, MD (Urasoe General Hospital); Yoshihiro Hagiwara, MD, MPH (Imperial Foundation Saiseikai, Utsunomiya Hospital); Shigeki Kushimoto, MD, PhD (Tohoku University Graduate School of Medicine); Reo Fukuda, MD (Nippon Medical School Tama Nagayama Hospital); Takayuki Ogura, MD, PhD (Japan Red Cross Maebashi Hospital); Shin-ichiro Shiraishi, MD (Aizu Central Hospital); Ryo-suke Zushi, MD (Osaka Mishima Emergency Critical Care Center); Norio Otani, MD (St. Luke’s International Hospital); Migaku Kikuchi, MD, PhD (Dokkyo Medical University); Kazuhiro Watanabe, MD (Nihon University Hospital); Takuo Nakagami, MD (Omihachiman Community Medical Center); Tomohisa Shoko, MD, PhD (Tokyo Women’s Medical University Medical Center East); Nobuya Kita-mura, MD, PhD (Kimitsu Chuo Hospital); Takayuki Otani, MD (Hiroshima City Hiroshima Citizens Hospital); Yoshinori Matsuoka, MD, PhD (Kobe City Medical Center General Hospital); Makoto Aoki, MD, PhD (Gunma University Graduate School of Medicine); Masaaki Sakuraya, MD, MPH (JA Hiroshima General Hospital Hiroshima); Hideki Arimoto, MD (Osaka City General Hospital); Koi-chiro Homma, MD, PhD (Keio University School of Medicine); Hir-omichi Naito, MD, PhD (Okayama University Hospital); Shunichiro Nakao, MD, PhD (Osaka University Graduate School of Medicine); Tomoya Okazaki, MD, PhD (Kagawa University Hospital); Yoshio Tahara, MD, PhD (National Cerebral and Cardiovascular Center); Hiroshi Okamoto, MD, MPH (St. Luke’s International Hospital); Jun Kunikata, MD, PhD, and Hideto Yokoi, MD, PhD (Kagawa University Hospital).
Data Availability
The author should be contacted for data requests.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this article.