
Abstract
The application value of mechanical thrombectomy (MT) in acute large-vessel occlusion cerebral infarction has been confirmed, but considering the poor prognosis of large-core infarction (LCI), the current guidelines and practices are based on anterior circulation small-core infarction. Reducing the perioperative complications of thrombectomy in LCIs is the key to saving more patients previously considered unsuitable for thrombectomy. Patients with acute anterior circulation cerebral infarction who were admitted to Suining Central Hospital of Sichuan Province from January 2022 to December 2023 and whose Alberta Stroke Program Early Computed Tomography Score value was 3–5 (the score range was 0–10, and the lower the score was, the larger the infarct area) or whose infarct core volume was ≥70 mL and who received MT were enrolled consecutively. The patients were grouped based on whether they were treated with mild hypothermia (mild hypothermia treatment group vs. conventional treatment group). Patients who were evaluated preoperatively for large-core cerebral infarction and underwent mild hypothermia treatment were performed immediately after MT. The clinical data of the patients were collected. The primary outcome events were the incidence of cerebral hernia within one week after the operation and the rate of requiring decompressive craniectomy (%). The secondary outcome was the modified Rankin scale (mRS) score at 90 days (the score range was 0–6, and the higher the score was, the greater the degree of functional disability). A total of 64 patients were included. Twenty-nine patients were assigned to the mild hypothermia treatment group, and 35 patients were assigned to the conventional treatment group. There was no significant difference in the baseline data between the two groups. The proportions of cerebral hernia and the need for decompressive craniectomy within one week after the operation were significantly lower in the mild hypothermia treatment group than in the conventional treatment group (31% vs. 57.1%, odds ratio [OR] 0.338, 95% confidence interval [CI] 0.120–0.948; p = 0.037). The proportion of patients who underwent decompressive craniectomy in the mild hypothermia treatment group was significantly lower (13.8% vs. 42.8%, OR 0.213, 95% CI 0.061–0.745, p = 0.011). There was no significant difference in the mRS score between the two groups at 90 days (4.31 ± 1.75 vs. 4.48 ± 1.57, p = 0.456) or in the proportion of patients with a good prognosis (mRS 0–3) between the two groups (OR 0.569, 95% CI 0.18–1.793, p = 0.333). Mild hypothermia treatment can reduce the incidence of early cerebral hernia and the need for decompressive craniectomy in patients with acute large-core cerebral infarction after MT; this treatment can be used as an important adjuvant treatment after thrombectomy for LCI, but may not change the long-term prognosis.
Keywords
Introduction
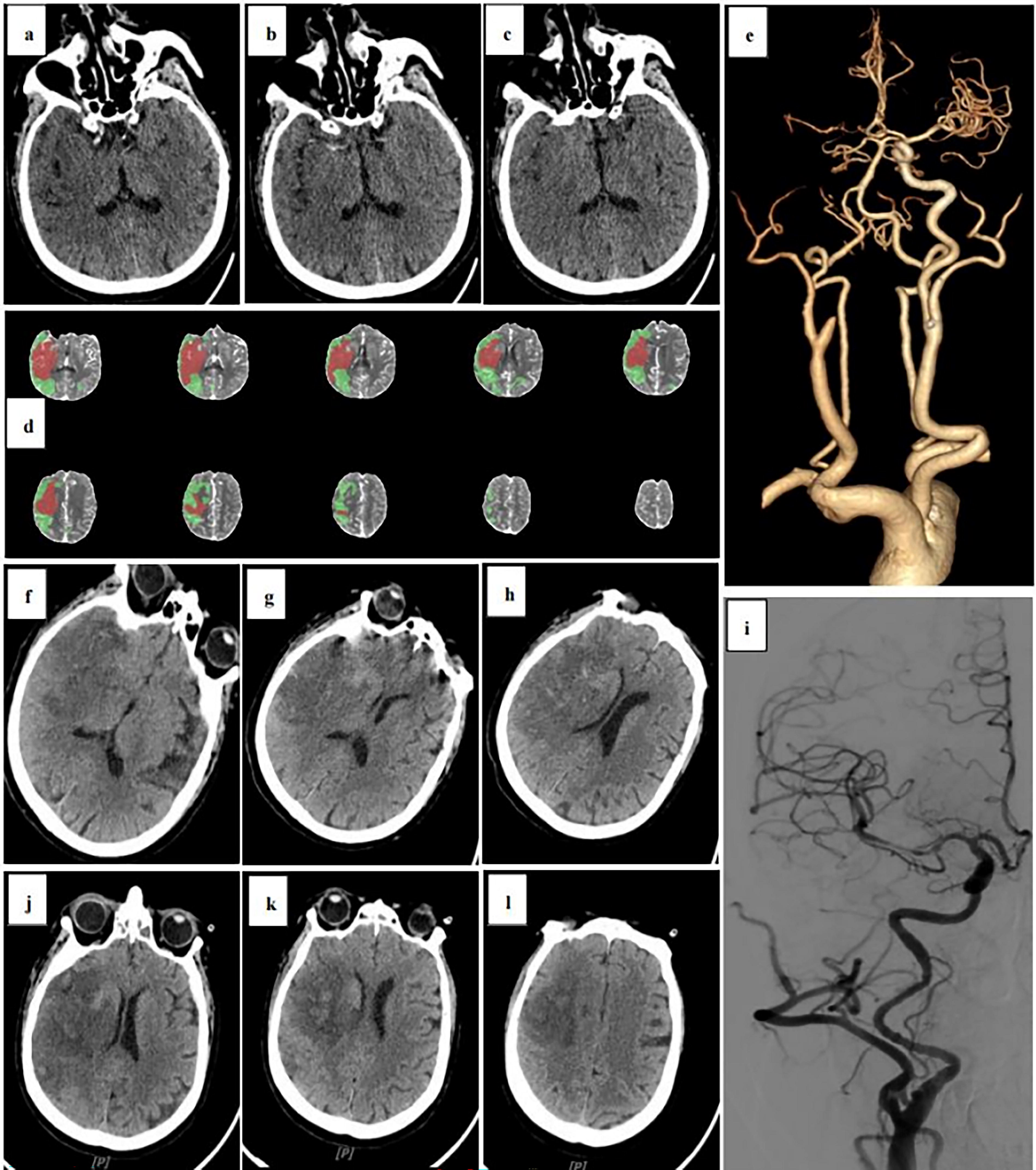
It is generally believed that the reperfusion effect of a large-core infarction (Migdady et al., 2023) (LCI) with an Alberta Stroke Program Early Computed Tomography Score (ASPECTS) <6 or an infarction volume greater than 70 mL is poor and that mechanical thrombectomy (MT) yields more complications (Chen et al., 2019; Leslie-Mazwi et al., 2021). Thus, there are few studies on MT in patients with low ASPECTS values. Recently, published studies have confirmed the effectiveness of MT in patients with low ASPECTS values, indicating that patients with ASPECTS 3–5 who receive MT treatment have a significantly higher rate of a good prognosis, but the rate of intracranial hemorrhage is greater. At our center, dyna computed tomography (CT) performed immediately after the recanalization of occluded vessels revealed extensive extravasation of contrast media in the LCI area. Such patients have a high probability of postoperative hemorrhage and excessive brain edema, leading to a high incidence of cerebral hernia (Wu et al., 2023). Reducing the incidence of brain edema and cerebral hernia during the perioperative period of MT can significantly decrease the mortality rate of patients in the acute phase and reduce the risk of decompressive surgery. Therefore, we attempted to use mild hypothermia for the treatment of these patients and achieved good curative effects.
Methods
Research design
This was a single-center, retrospective cohort study. The study was designed according to the 1964 Declaration of Helsinki and its subsequent amendments or similar ethical standards. Due to the retrospective nature of our study, our institutional review committee exempted informed consent. The study protocol was reviewed and approved by the Medical Research Ethics Committee of Suining Central Hospital, and the IRB approval number is KYLLKS20240071.
Patients
Patients aged 18–80 years with acute ischemic stroke admitted to our hospital between January 2022 and December 2023 had a National Institute of Health Stroke Scale (NIHSS) score ranging from 6 to 31 (the score range was 0–42, and the higher the score was, the more severe the neurological impairment) and a modified Rankin scale (mRS) score ranging from 0 to 1 before the onset of the disease (completely asymptomatic or symptomatic but without obvious disability and able to complete regular work before onset). Acute internal carotid artery (ICA) and/or middle cerebral artery (MCA) occlusion was determined by computed tomography angiography (CTA) or magnetic resonance angiography (MRA). The imaging criteria were an ASPECTS value of 3–5 or a multimodal imaging evaluation of the core infarction [defined as CT perfusion imaging regional cerebral blood flow (rCBF) <30% or MRI apparent diffusion coefficient (ADC) <620*10−6 mm2/s] volume ≥70 mL or a CT/MRI mismatch ratio (Tmax >6 seconds/core infarction volume) >1.2. All medical records were signed by patients or their legally authorized representatives with informed consent. The exclusion criteria were as follows: unstable vital signs (including uncontrollable hypertension), history of acute intracranial hemorrhage, intracranial hemorrhage or severe traumatic brain injury, intracranial tumors or giant aneurysms, bleeding tendency [platelet count <100*109/L, receiving low molecular weight heparin treatment within 24 hours, oral anticoagulants and international normalized ratio (INR) >1.7 or Prothrombin time (PT) >15 seconds, using thrombin inhibitor within 48 hours], high or low blood glucose (<2.8 mmol/L or >22.22 mmol/L), incomplete medical history, and bilateral or multiple vascular occlusions.
Grouping and intervention
According to the guidelines for ischemic stroke (Winstein et al., 2016), patients with indications for intravenous (IV) thrombolysis received thrombolysis with alteplase (rt-PA, onset time within 4.5 hours, 0.9 mg/kg body weight) or urokinase (onset time 4.5–6 hours, 1–1.5 million units) and bridged IV thrombolysis with thrombectomy. According to the patient’s condition, the best endovascular treatment, including stent thrombectomy, aspiration, and balloon dilatation, was selected (Bendszus et al., 2023). All patients achieved effective reperfusion modified Thrombolysis in Cerebral Infarction [(mTICI) 2 b/3], and all were admitted to the neurological intensive care unit for close observation and given the following standard medical treatment: blood pressure was controlled between 120∼140/60∼90 mmHg according to the baseline blood pressure, and reexaminations via cranial CT and cerebrovascular imaging transcranial Doppler [(TCD), MRA, CTA, or digital subtraction angiography (DSA)] were conducted within 24 hours. For patients in the mild hypothermia treatment group, a semi-conductor cooling blanket was used to cool the whole body, an ice cap was worn on the head, and the anal temperature was monitored at the same time. The anal temperature was set at 32–35°C, and the temperature reached the predetermined range within 5 hours (Khellaf et al., 2019). For the mild hypothermia treatment group, the introduction of mild hypothermia was initiated at the same time for all patients with acute large core infarcts undergoing mechanical thrombolysis, which was immediately upon return to the neurointensive care unit after completion of the mechanical thrombolysis procedure.
Outcomes
The general baseline data of the included patients included age, sex, admission NIHSS score, ASPECTS, previous medical history (atrial fibrillation, previous stroke), cardiovascular risk factors (hypertension, diabetes, smoking), occlusion site, time of receiving mild hypothermia treatment, etc. The main outcome events were the incidence of cerebral hernia within one week after the operation and the rate of requiring decompressive craniectomy (%). The purpose of this study was to determine whether mild hypothermia treatment could reduce the incidence of postoperative cerebral hernia, perioperative mortality, and the rate of unplanned reoperations. The secondary outcome was the 90-day mRS score. There was a difference in the proportion of patients with a good prognosis (mRS 0–3) between the two groups. Another aim of this study was to determine whether there was a difference in the 90-day prognosis between the two groups. The 90-day mRS score was obtained through telephone follow-up by our stroke health manager.
Statistical analysis
SPSS Statistics (version 27.0.1.0, 64 bit, IBM) software was used for the data analysis. The count data are expressed herein as the number of patients and percentage (%). The χ2 test was used for comparisons between groups, and odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. When the number of expected events was less than 5, Fisher’s exact probability method was used. Normally distributed measurement data are expressed as &x ± s, and comparisons between groups were performed by t tests. The data with a skewed distribution are expressed as the median and interquartile range (IQR), and comparisons between groups were performed with the Mann–Whitney U test. p < 0.05 was considered to indicate statistical significance.
Results
Baseline characteristics
A total of 72 patients with LCIs were included in the study, and 8 patients who had incomplete data, were lost to follow-up, or experienced acute death 3 days after surgery, including 3 patients in the mild hypothermia treatment group and 5 patients in the conventional treatment group, were excluded (Fig. 1). The baseline demographic and clinical characteristics of the two groups were similar. The median age of the patients in the mild hypothermia treatment group was 73 years (IQR 64.5–78.5), and the median age of the patients in the conventional treatment group was 71 years (IQR, 56–78). The mild hypothermia treatment group included 13 males and 16 females, whereas the conventional treatment group included 16 males and 19 females. The median NIHSS score was 15 in the mild hypothermia treatment group (IQR, 12.5–18.5) and 17 in the conventional treatment group (IQR, 14–21). There was no difference in the number of occlusive sites between the two groups. There was no significant difference in the baseline data between the included patients (p > 0.05). The prevalence rates of hypertension, diabetes, and previous stroke in the mild hypothermia treatment group were greater than those in the conventional treatment group, whereas the prevalence rates of previous smoking and atrial fibrillation in the mild hypothermia treatment group were less than those in the conventional treatment group, but the differences were not statistically significant (p > 0.05). The baseline data and clinical characteristics of the patients are shown in the Table 1.

Flow of patients through this study. The Alberta Stroke Program Early Computed Tomography Score (ASPECTS) ranges from 0 to 10, with lower values indicating greater infarction. National Institutes of Health Stroke Scale (NIHSS) scores range from 0 to 42, with higher scores indicating a greater neurological deficit.
Baseline Characteristics of the Patients
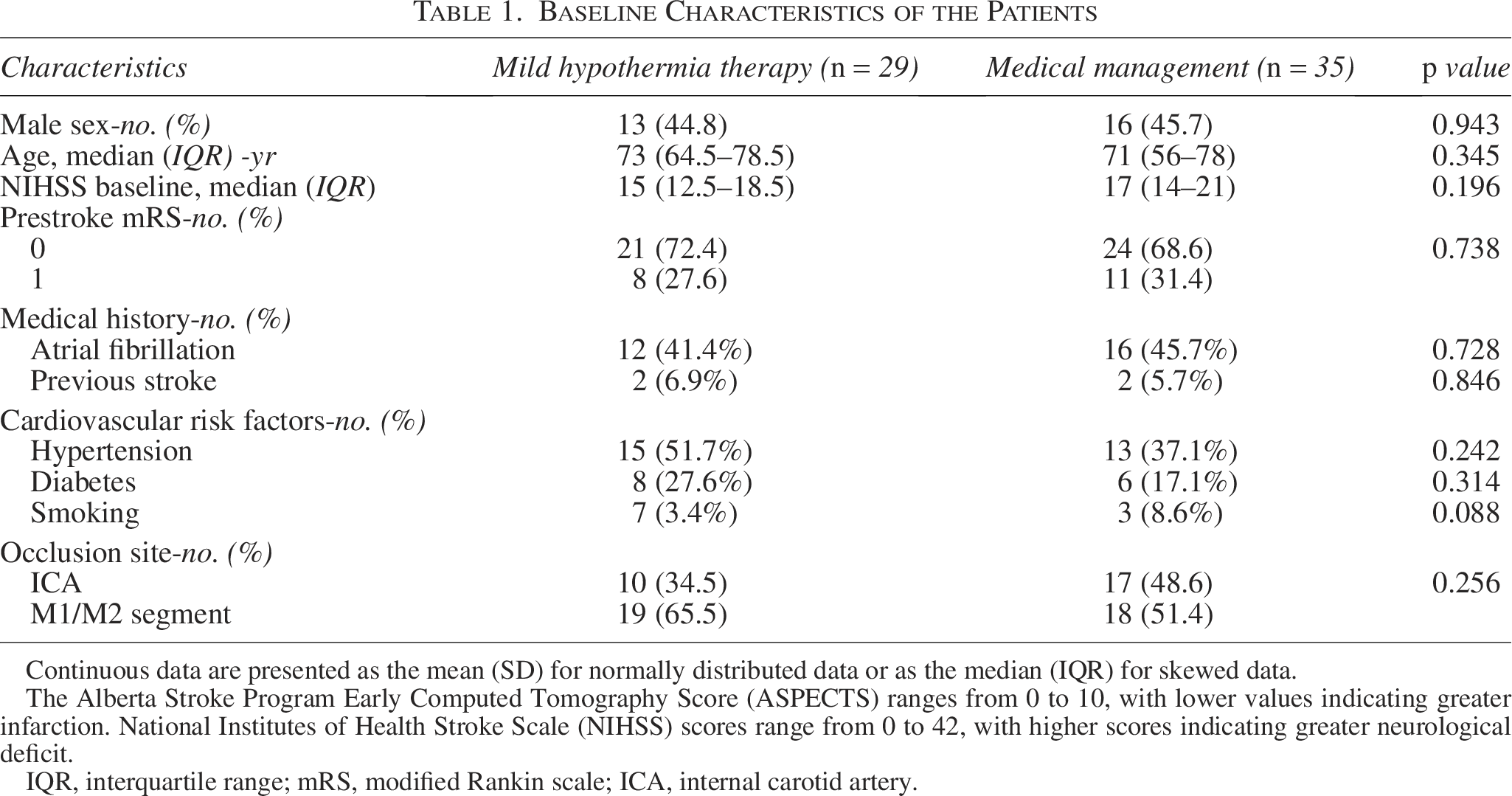
Continuous data are presented as the mean (SD) for normally distributed data or as the median (IQR) for skewed data.
The Alberta Stroke Program Early Computed Tomography Score (ASPECTS) ranges from 0 to 10, with lower values indicating greater infarction. National Institutes of Health Stroke Scale (NIHSS) scores range from 0 to 42, with higher scores indicating greater neurological deficit.
IQR, interquartile range; mRS, modified Rankin scale; ICA, internal carotid artery.
Outcomes
The primary outcome end point was cerebral hernia after thrombectomy requiring decompressive craniectomy. In the mild hypothermia treatment group, a total of 29 patients with LCIs underwent MT, of whom nine patients developed large-area brain edema/hernia after the operation, requiring decompressive craniectomy, accounting for 31%. In the conventional treatment group, 35 patients with LCIs underwent thrombectomy, and 20 patients developed cerebral hernias, accounting for 57.1% (OR 0.338, 95% CI 0.120–0.948, p = 0.037). The proportion of patients receiving decompressive craniectomy in the mild hypothermia treatment group was lower (13.8% vs. 42.8%, OR 0.213, 95% CI 0.061–0.745, p = 0.011). The difference between the two groups was statistically significant (p < 0.05), indicating that mild hypothermia treatment can reduce the risk of cerebral hernia and the need for decompressive craniectomy in patients with MT (Fig. 2). The 90-day mRS scores of the two groups were as follows: the median mRS score of the mild hypothermia treatment group was 4 (IQR, 4–6), the median mRS score of the conventional treatment group was 4 (IQR, 3–6), and the difference was not statistically significant (p = 0.678). The 90-day prognosis (mRS 0–3) was 20.7% in the mild hypothermia treatment group and 31.4% in the conventional treatment group (OR 0.569, 95% CI 0.180–1.793, p = 0.333). There was no significant difference between the two groups (p > 0.05) (Table 2). The overall long-term mortality of MT in patients with LCI is approximately 30%. Although MT can reduce the incidence of perioperative cerebral hernia and early mortality, it has no effect on the long-term prognosis (Fig. 3). According to the subgroup analysis, there were differences between the two groups in age, occlusion site, NIHSS score, and ASPECTS distribution, and the infarct core volumes were similar, but some ratio efficiencies were limited (including OR = 1).
Mild Hypothermia Therapy after Mechanical Thrombectomy (MT) for Acute Ischemic Stroke with Large Infarction.
Primary and Secondary Outcomes

Z value for Mann–Whitney U test.
95% CI, 95% confidence interval; IQR, interquartile range; mRS, modified Rankin scale.

Distribution of the modified Rankin scale score at 90 days. A modified Rankin scale score of 0 indicates no symptoms; a score of 1 indicates no clinically significant disability (patients are able to perform usual work, leisure, and school activities); a score of 2 indicates slight disability (patients are able to look after their own affairs without assistance, but are unable to carry out all previous activities); a score of 3 indicates moderate disability (patients require some help, but are able to walk unassisted); a score of 4 indicates moderately severe disability; a score of 5 indicates severe disability (patients are bedridden and require constant care); and a score of 6 indicates death.
Subgroup analysis of the primary outcome of postoperative cerebral hernia included age less than 70 years, site of occlusion, initial NIHSS score less than 16, distribution of ASPECTS values in the 3–5 range, and whether the core infarct volume was greater than 70 mL. Studies have shown that mild hypothermia treatment seems to result in a lower incidence of cerebral hernia in people over the age of 70 years than in younger individuals. In addition, patients with an ASPECTS value of 5 had better outcomes after mild hypothermia treatment, which may be related to a decreased infarct volume. The effectiveness of the remaining subgroup analysis was insufficient in this study, and there no difference was found (Table 3).
Subgroup Analyses of Postoperative Brain Herniation
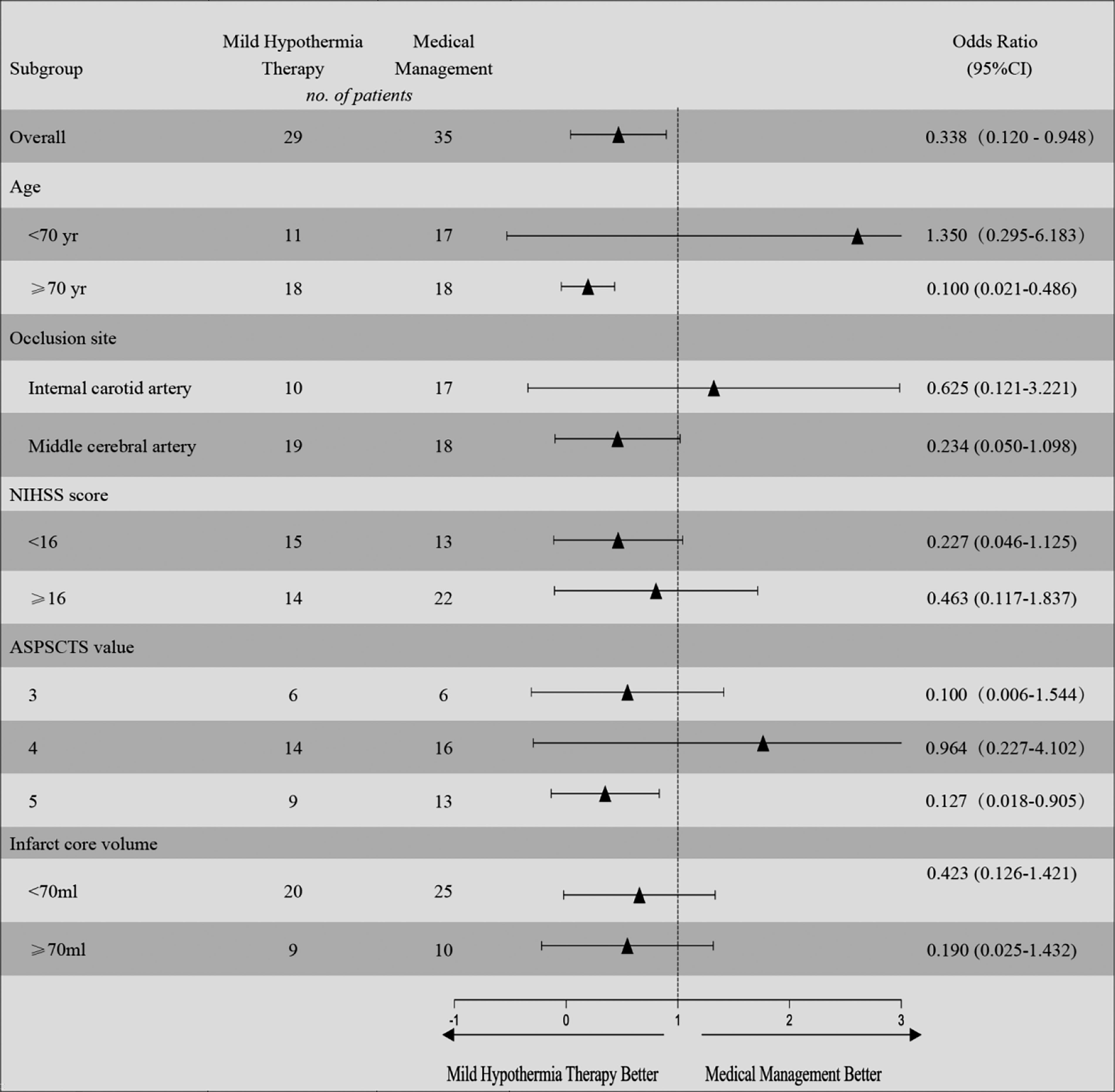
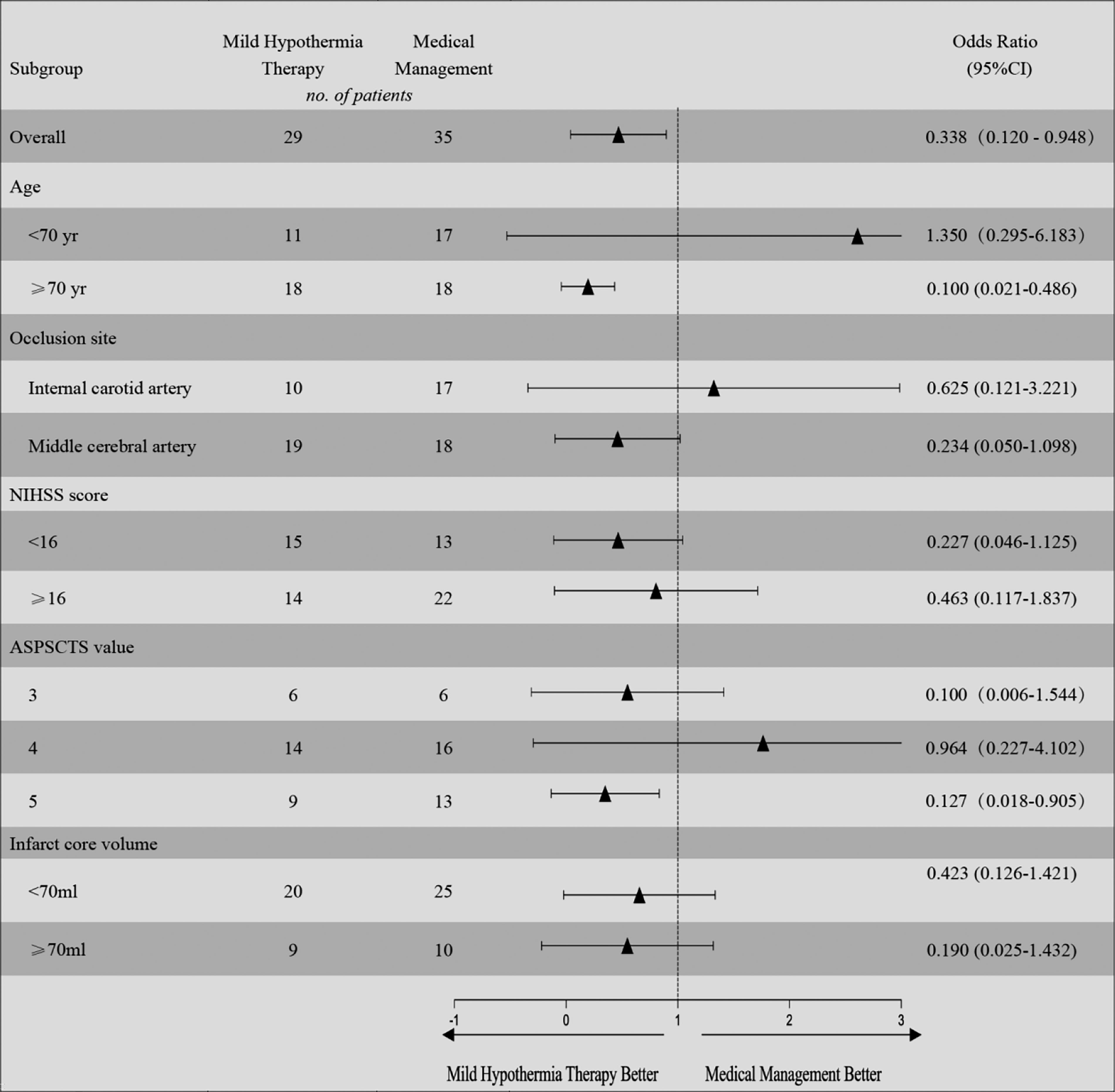
Studies have shown that mild hypothermia treatment seems to yield a lower incidence of cerebral hernia in people over the age of 70 years than in younger individuals. In addition, patients wisth an ASPECTS value of 5 had better outcomes after mild hypothermia treatment, which may be related to a decreased infarct volume. The effectiveness of the remaining subgroup analyses was insufficient in this study, and no difference was found.
95% CI, 95% confidence interval; ASPECTS, The Alberta Stroke Program Early Computed Tomography Score; NIHSS, National Institutes of Health Stroke Scale.
Discussion
There are few reports on the treatment of mild hypothermia after LCI. Considering the important value of mild hypothermia in patients with traumatic brain injury, we innovatively combined intravascular therapy with mild hypothermia treatment in patients with acute cerebral infarction and conducted observations. Our study showed that after LCI, thrombectomy combined with mild hypothermia treatment can reduce the incidence of postoperative cerebral hernia and decompressive craniectomy and reduce the mortality of patients in the acute perioperative period and can be used as an important auxiliary treatment for LCI after thrombectomy. Considering the high overall mortality (20 − 30%) in patients with acute LCI, mild hypothermia treatment does not seem to improve the long-term prognosis of these individuals (Goyal et al., 2016). Our study revealed that regardless of whether mild hypothermia treatment was used, the median mRS score of patients with LCIs after thrombectomy at 90 days was 4, and the score in the upper quartile was 6 (death). The proportion of patients with a good prognosis (mRS 0–3) in the mild hypothermia treatment group was lower than that in the conventional treatment group, but the difference was not statistically significant. Further subgroup analysis revealed that mild hypothermia treatment seemed to lead to a lower incidence of cerebral hernia in people over 70 years old than younger individuals. Patients with an ASPECTS value of 5 had better outcomes after mild hypothermia treatment, which may be related to a decreased infarct volume.
Acute ischemic stroke is associated with a high rate of death and disability. The key to treatment is to open the blocked vessels as soon as possible to save the ischemic penumbra. IV thrombolysis and intravascular therapy are the main methods used (Mendelson and Prabhakaran, 2021). IV thrombolytic therapy has a clear benefit in the treatment of acute ischemic stroke, but the strict time limit limits its curative effect. Since 2015, the DAWN Clinical Trials (Nogueira et al., 2018) and DEFUSE 3 Clinical Trials (Albers et al., 2018) studies have extended the intravascular treatment time to 24 hours and improved the treatment efficiency for acute large-vessel occlusion stroke. It is generally believed that the reperfusion effect of LCIs with ASPECTS <6 or infarction volumes greater than 70 mL is poor, which is a contraindication for emergency endovascular treatment. However, in clinical practice, such patients still have a good prognosis 90 days after endovascular treatment (Sarraj et al., 2019). Three recent randomized trials included patients with ASPECTS 3–5 or ASPECTS 0–2 within 24 hours of onset and occlusion of the intracranial segment of the ICA or M1/M2 segment of the MCA with an infarct core volume greater than 70 mL. The study revealed that the 90-day mRS score of patients in the endovascular treatment group was significantly better compared with patients in the best medical treatment group, providing the highest evidence-based medical evidence for endovascular treatment of patients with LCIs and serving as the basis for endovascular treatment of LCIs in the anterior circulation (Huo et al., 2023; Sarraj et al., 2023; Yoshimura et al., 2022). Some studies even included the MT of patients with extremely large infarction cores, indicating that patients with ASPECTS values of 0–2 can still be screened for a mechanical therapy benefit from thrombectomy (Almallouhi et al., 2024).
Animal experiments have shown that hypothermia is a powerful neuroprotective agent and has been proven to improve many destructive effects of cerebral ischemia (Krieger and Yenari, 2004). In acute myocardial infarction, mild hypothermia (32–35°C) can reduce ischemia–reperfusion injury and infarct size, which has a cardioprotective effect. The possible mechanisms include enhancing the ability of mitochondria to respond to oxidative stress, improving the structural integrity of cells, and reducing apoptosis (Berg et al., 2023). There are few studies on mild hypothermia in the treatment of acute cerebral infarction. A meta-analysis of 2071 patients in 26 randomized controlled trials showed that thrombolysis combined with mild hypothermia can produce better therapeutic effects than thrombolysis alone, which may be due to the reduction in patients’ neurological dysfunction and inflammatory reaction levels, indicating that mild hypothermia has a protective effect on acute cerebral infarction (Guo et al., 2022).
Limitations
There are several limitations in our study. First, this was a retrospective cohort study, which may be associated with the risk of data loss or selection bias (Kelly et al., 2022). To reduce such risks, we attempted to fully include the research subjects, clarify the grouping basis, and perform one-on-one follow-up to reduce the rate of loss to follow-up. Second, this was a single-center study, and the selection of patients and the technique of the operator may have biased the results.
Conclusion
In conclusion, our study showed that mild hypothermia after thrombectomy in patients with acute LCI can reduce the incidence of acute cerebral hernia and decompressive craniectomy, although it cannot improve the long-term prognosis.
Authors’ Contributions
G.T. and J.W.: Original draft, review and editing (equal), J.D., L.L., C.H., and F.P.: Methodology, formal analysis. W.X.: Conceptualization (lead), review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Hospital-level scientific research topics in Suining Central Hospital (2021y39), Sichuan Province, China.