
Abstract
This study aims to equip clinicians with the necessary insights for identifying and managing pregnant women experiencing elevated maternal pyrexia during labor. It examines maternal and neonatal outcomes along with the factors associated with varying peak temperatures. A retrospective analysis was conducted on 319 pregnant women presenting with maternal pyrexia during labor. Participants were categorized into two groups based on peak temperature: Group A (n = 180, temperature <38°C) and Group B (n = 139, temperature ≥38°C). Basic characteristics, blood markers, and maternal and neonatal outcomes were compared between the two groups. (1) Group B exhibited a higher percentage of neutrophilic granulocytes (NE%) and C-reactive protein to lymphocyte ratio (CLR) compared with Group A (p < 0.05). (2) The rates of meconium-stained amniotic fluid, histological chorioamnionitis, hospitalization of neonates, and infections in neonates were greater in Group B than in Group A (p < 0.05). (3) Logistic regression analysis identified elevated CLR levels as a risk factor for peak temperatures exceeding 38°C, indicating that CLR could serve as a reliable predictor of maternal pyrexia above 38°C during labor. Higher maternal pyrexia peaks may exacerbate adverse maternal and neonatal outcomes, emphasizing the importance of timely clinical intervention. NE% and CLR could serve as valuable indicators for identifying underlying causes and predicting peak maternal pyrexia during labor.
Introduction
Maternal pyrexia during labor is a common clinical condition associated with significant risks to both maternal and neonatal health during the perinatal period, with incidence rates ranging from 2% to 10% (Patel et al., 2023; Towers et al., 2017). While most studies define maternal pyrexia as a temperature of ≥38°C, some studies consider a lower threshold of ≥37.5°C (Patel et al., 2023; Towers et al., 2017; Anonymous, 2019; Higgins et al., 2016; Sharpe and Arendt, 2017). Irrespective of the specific cutoff, maternal pyrexia is widely recognized as a risk factor for adverse perinatal outcomes. These complications include severe maternal and neonatal events such as cesarean delivery, postpartum hemorrhage (PPH), obstructed labor, assisted vaginal delivery, neonatal sepsis, asphyxia, and encephalopathy (An et al., 2022).
Recent studies on maternal pyrexia during labor have highlighted the effects of elevated maternal temperature on both maternal and neonatal outcomes, making it a prominent focus in perinatal research. Perspectives differ regarding the relationship between peaks of pyrexia during labor and perinatal outcomes. Previous research has indicated a correlation between neonatal outcomes and the severity of elevated maternal pyrexia during labor (Hochler et al., 2021). In this context, our aim is to elucidate the maternal and neonatal outcomes associated with different degrees of peak maternal pyrexia during labor, as well as to analyze the factors influencing these outcomes. Ultimately, we seek to assist clinicians in recognizing and effectively managing the implications of varying levels of maternal pyrexia during labor, thereby improving adverse pregnancy outcomes and enhancing neonatal prognosis.
Materials and Methods
Data selection
The study received approval from the Ethics Committee of our hospital. Comprehensive case data were gathered from 319 pregnant women diagnosed with maternal pyrexia during labor who delivered at our hospital between January 2022 and June 2024.
Diagnostic criteria
Maternal pyrexia during labor is defined as a maternal temperature of ≥37.5°C recorded between the onset of labor and delivery (Dior et al., 2014).
Histological chorioamnionitis was identified by acute inflammatory changes, characterized by the presence of more than five polymorphonuclear leukocytes per high-power field in any of the fetal membranes, amniotic membranes, chorionic villi, or umbilical cord (Holzman et al., 2007; Crum and Lee, 2007).
Inclusion and exclusion criteria for study participants
Inclusion criteria
(1) Full-term, singleton live birth; (2) availability of complete medical history; and (3) vaginal delivery with a recorded temperature ≥37.5°C during labor.
Exclusion criteria
(1) Incomplete medical history; (2) multiple pregnancies; (3) gestational age less than 37 weeks or occurrence of stillbirth; and (4) fever caused by respiratory tract infections, gastrointestinal tract infections, urinary tract infections, or similar causes.
Research methods
A total of 319 pregnant women with maternal pyrexia during labor were classified into two groups: Group A, consisting of 180 cases with a peak temperature <38°C, and Group B, comprising 139 cases with a peak temperature ≥38°C. A retrospective analysis was performed to compare basic demographic data, blood markers, and maternal and neonatal outcomes between the two groups.
Research indicators
Basic information of pregnant women
The basic information collected for the study included maternal age, body mass index (BMI), gestational week at delivery, incidence of premature rupture of membranes (PROM), pregnancy complications (such as gestational diabetes mellitus [GDM], hypertensive disorders of pregnancy [HDP], thyroid disorders, oligohydramnios, and intrahepatic cholestasis of pregnancy [ICP]). Additional data on the presence of vaginal group B streptococcal (GBS) infections, induction of labor, and administration of labor analgesia were also recorded.
Maternal blood markers
Pregnant women experiencing maternal pyrexia during labor underwent routine blood tests, including assessments of C-reactive protein (CRP). The analysis compared the white blood cell (WBC) count, percentage of neutrophilic granulocytes (NE%), neutrophil (NE) count, lymphocyte (LY) count, CRP levels, and the C-reactive protein to lymphocyte ratio (CLR) between the two groups, with CLR calculated as CRP/LY.
Maternal and neonatal outcomes
These maternal and neonatal outcomes evaluated included the mode of delivery, incidence of meconium-stained amniotic fluid, placental abruption, PPH, histological chorioamnionitis, neonatal asphyxia, neonatal hospitalization, neonatal respiratory failure, neonatal aspiration pneumonia, and neonatal infections, among other complications.
Statistical processing
Data processing and analyses were conducted using SPSS 25.0 software. Measurement data are presented as mean ± standard deviation, with a t-test employed for comparisons between the two groups. Count data are reported as the number of cases (percentage) (n [%]), and the χ2 test was used for comparisons between the groups. A p < 0.05 was considered statistically important. Additionally, multivariate logistic regression was utilized to identify effective predictors of peak maternal pyrexia during labor exceeding 38°C.
Results
Comparison of basic information between Group A and Group B
There were no statistically significant differences in maternal age, BMI, gestational week at delivery, PROM, pregnancy complications (including GDM, HDP, thyroid disorders, oligohydramnios, and ICP), vaginal GBS infection, induction of labor, or administration of labor analgesia between the two groups (p > 0.05), as detailed in Table 1.
Analysis of Basic Data of Pregnant Women Across Two Groups
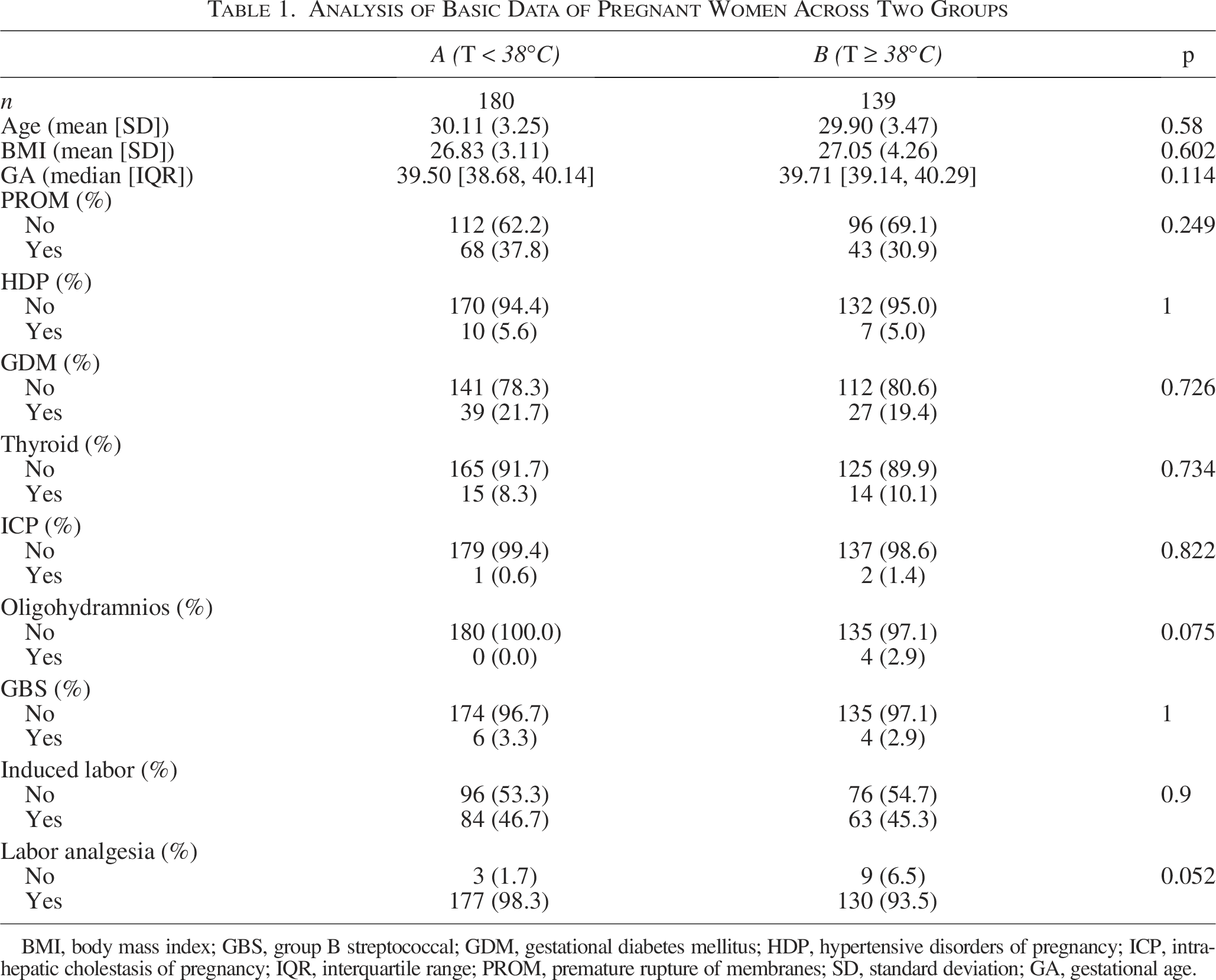
BMI, body mass index; GBS, group B streptococcal; GDM, gestational diabetes mellitus; HDP, hypertensive disorders of pregnancy; ICP, intrahepatic cholestasis of pregnancy; IQR, interquartile range; PROM, premature rupture of membranes; SD, standard deviation; GA, gestational age.
Comparison of blood markers of pyrexia in Group A and Group B
All participants underwent routine blood tests and CRP assessments at the onset of their first fever, and blood markers were compared between the two groups. The results indicated that the NE% and CLR levels in Group B were higher than those in Group A, with statistical differences (p < 0.05). However, no statistically significant differences were observed in WBC count, NE count, LY count, and CRP levels between the two groups (p > 0.05), as shown in Table 2.
Analysis of Blood Markers Associated with Maternal Pyrexia During Labor
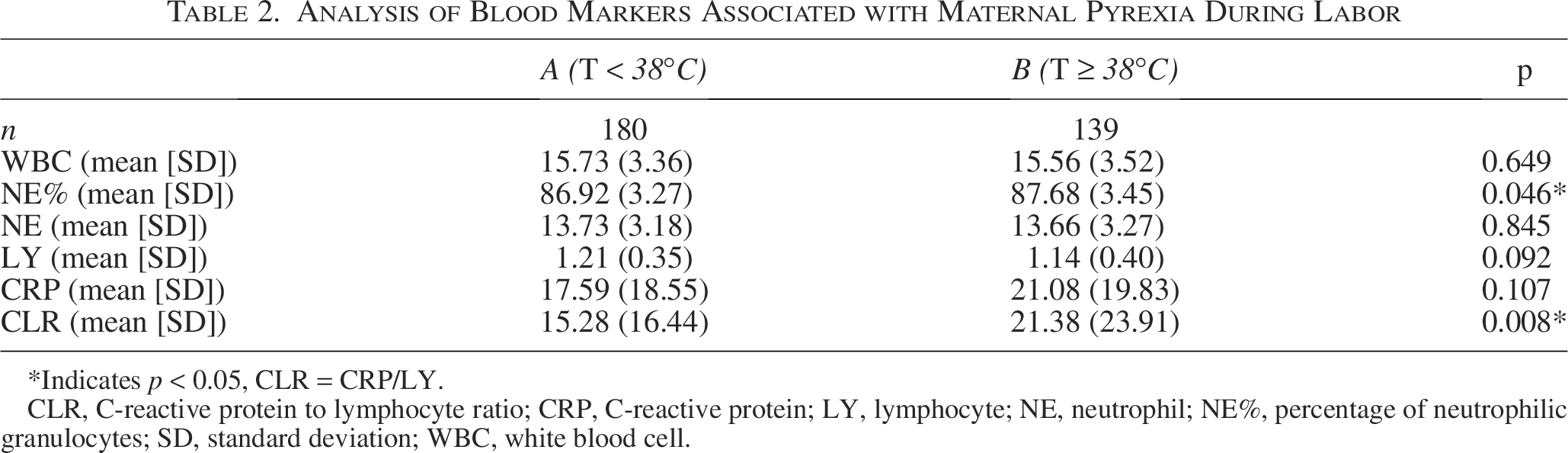
Indicates p < 0.05, CLR = CRP/LY.
CLR, C-reactive protein to lymphocyte ratio; CRP, C-reactive protein; LY, lymphocyte; NE, neutrophil; NE%, percentage of neutrophilic granulocytes; SD, standard deviation; WBC, white blood cell.
Comparison of maternal and neonatal outcomes between Group A and Group B
The analysis of maternal and neonatal outcomes revealed that the incidence of meconium-stained amniotic fluid, histological chorioamnionitis, hospitalization of neonates, and neonatal infections was significantly higher in Group B compared with Group A (p < 0.05). Conversely, there were no statistically significant differences in mode of delivery, placental abruption, PPH, neonatal asphyxia, neonatal respiratory failure, and neonatal aspiration pneumonia between the two groups (p > 0.05), as shown in Table 3.
Analysis of Maternal and Neonatal Outcomes
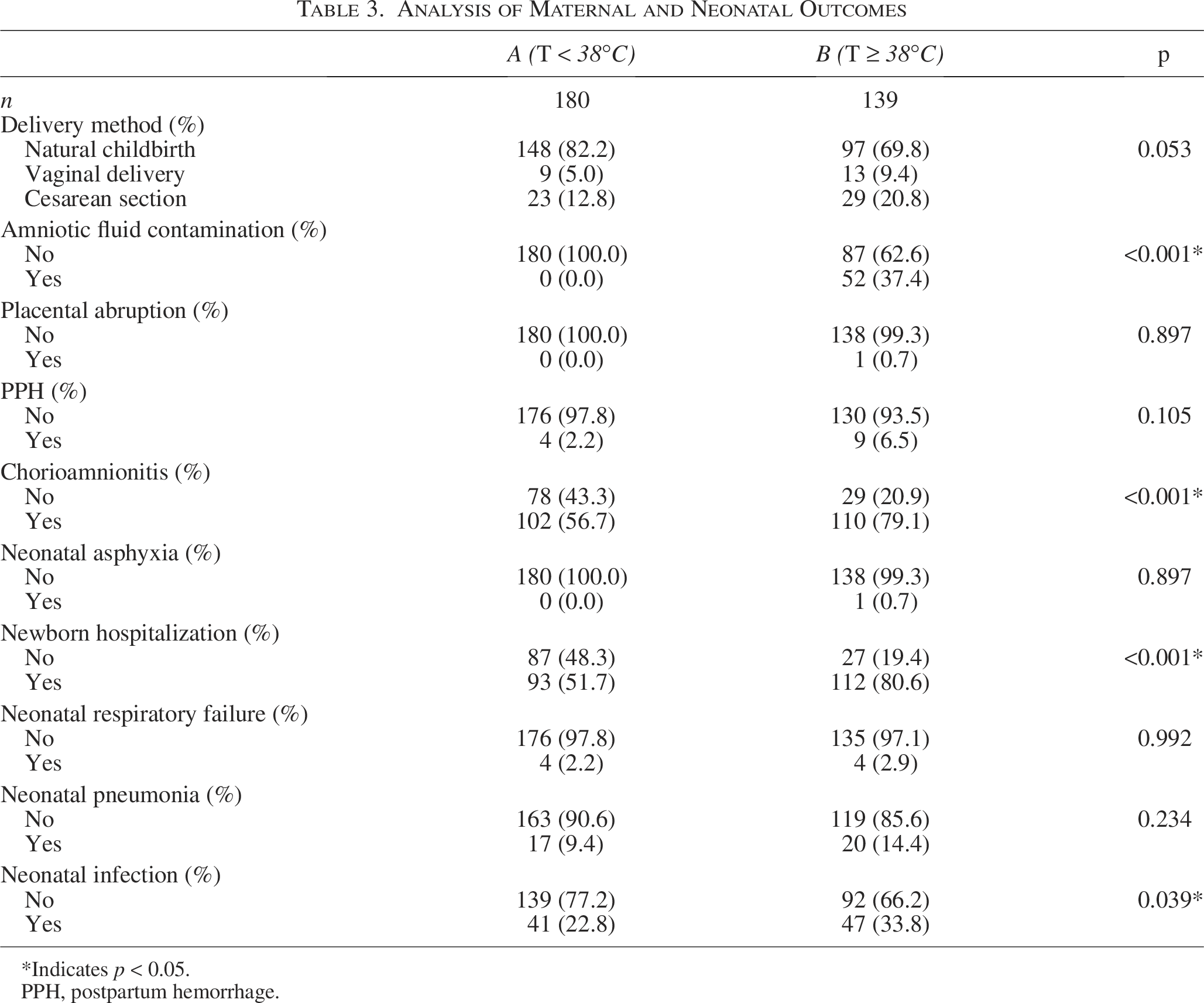
Indicates p < 0.05.
PPH, postpartum hemorrhage.
Analysis of predicting factors of maternal pyrexia during labor at ≥38°C
The comparison of maternal blood markers and maternal and neonatal outcomes indicated that the incidence of meconium-stained amniotic fluid, histological chorioamnionitis in pregnant women, neonatal hospitalization, and neonatal infections was higher in Group B than in Group A. The differences were statistically significant (p < 0.05), indicating a greater incidence of adverse outcomes for both mothers and infants in the group with peak maternal pyrexia during labor at ≥38°C.
Through univariate analysis of the blood markers in pregnant women with pyrexia, several statistically significant indicators were identified, including NE%, CLR, and LY count. Subsequent multivariate logistic regression analysis demonstrated a statistically significant in CLR between the two groups, indicating that higher CLR levels were associated with an increased risk of maternal pyrexia reaching ≥38°C. Therefore, CLR may serve as an effective predictor of peak maternal pyrexia during labor at or above 38°C, as shown in Table 4.
Multivariate Analysis of Predictors for Maternal Pyrexia (≥38°C)
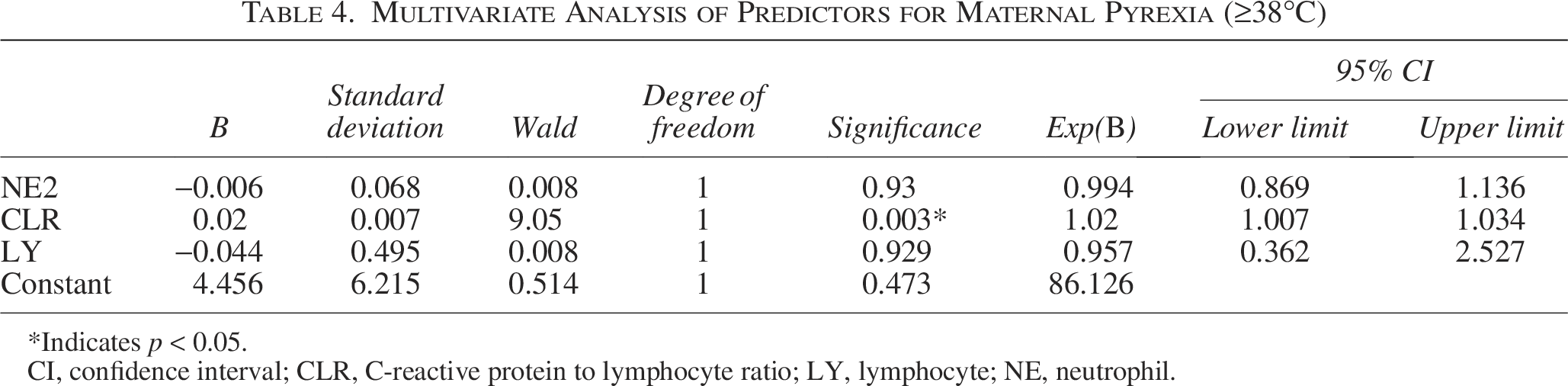
Indicates p < 0.05.
CI, confidence interval; CLR, C-reactive protein to lymphocyte ratio; LY, lymphocyte; NE, neutrophil.
Discussion
Maternal pyrexia during labor represents a considerable perinatal risk to the well-being of both mothers and infants. It has been associated with an increased likelihood of adverse maternal and neonatal outcomes, such as PPH, assisted vaginal deliveries, cesarean sections, low Apgar scores in newborns, respiratory distress, neonatal sepsis, meconium aspiration, and increased rates of admission to the neonatal intensive care unit. The fever that occurs during labor can be attributed to both infectious and non-infectious factors (Higgins et al., 2016). Infectious causes are primarily linked to reproductive system infections, such as chorioamnionitis, while non-infectious causes often relate to epidural labor analgesia, stress during labor, and other contributing elements. Adverse maternal and neonatal outcomes are predominantly linked to infectious factors (Kim et al., 2021). Furthermore, evidence suggests that both infectious and non-infectious origins of maternal pyrexia are associated with negative neonatal outcomes, including low Apgar scores, respiratory distress, hypotonia, and seizures in neonates (Curtin et al., 2015). Notably, even in the absence of infection, maternal pyrexia during labor poses a significant risk for neonatal complications, including dysplasia, encephalopathy, cerebral palsy, and neonatal fatality (Impey et al., 2008).
Previous studies have showed that the severity of pyrexia during labor correlates with maternal and neonatal morbidity; however, the results remain contentious. Hongmin et al. found that as body temperature increased, so too did the risk of histological chorioamnionitis, along with the likelihood of adverse maternal and neonatal outcomes (An et al., 2022). Maternal temperatures exceeding 38.0°C were found to be more strongly associated with negative outcomes compared with temperatures of 37.5°C. Specifically, temperatures above 39°C were identified as significant risk factors for severe neonatal morbidity and operative deliveries. Hensel et al. classified patients into three groups based on body temperature (T): no fever (T < 38°C), mild fever (38°C ≤ T ≤ 39°C), and hyperthermia (T > 39°C) (Hensel et al., 2022). They explored the relationship between the severity and duration of maternal pyrexia during labor and the associated maternal and neonatal morbidities, suggesting that the overall morbidity rate of newborns may be potentially dose-dependent on the severity of maternal pyrexia during labor.
In a study by Lieberman et al. involving 1233 singleton full-term pregnant women, it was found that the risk of cesarean section or assisted vaginal delivery tripled when the mother’s temperature reached or exceeded 38.0°C during labor (Lieberman et al., 1999). Furthermore, a small retrospective study indicated that mothers with pyrexia faced a higher risk of delivering neonates with low Apgar scores, respiratory distress, hypotonia, and the need for ventilatory support (Greenwell et al., 2012). In this study, a maternal temperature of ≥37.5°C during the period after labor and before delivery was classified as maternal pyrexia. The highest recorded body temperatures of women with pyrexia were divided into two categories: those with temperatures <38°C and those with temperatures ≥38°C. Statistical analysis showed no significant differences in baseline characteristics between the two groups, and factors related to pregnancy complications were excluded.
The incidence of contaminated amniotic fluid, histological chorioamnionitis, neonatal hospitalization, and neonatal infection rates were found to be higher in the group with body temperatures ≥38°C compared with those with temperatures <38°C. This finding suggests that elevated maternal temperatures are associated with an increased risk of chorioamnionitis and a higher likelihood of adverse neonatal outcomes. Consequently, the severity of fever is more strongly associated with chorioamnionitis and negative neonatal outcomes, aligning with findings from previous studies. Therefore, it is essential for clinicians to closely monitor and actively manage pregnant women with temperatures ≥38°C to reduce potential adverse maternal and neonatal outcomes.
Maternal hypothermia during labor is primarily indicative of dysfunction in maternal physiology, whereas maternal hyperthermia often suggests infection, particularly chorioamnionitis (Hoang et al., 2013). When such infections become severe and unmanageable, they can have a profoundly negative impact on newborns. The findings of this study reveal a higher incidence of histological chorioamnionitis among pregnant women with a maximum body temperature of ≥38°C compared with those with temperatures <38°C, suggesting that the risk of infection escalates with increasing temperatures.
In this research, routine blood tests and CRP assessments were conducted on all pregnant women at the onset of their first fever, with clinical diagnoses and treatments guided by the results obtained. The laboratory markers commonly utilized in obstetrics to evaluate inflammation include WBC, NE%, CRP, and procalcitonin (PCT). However, PCT was excluded from this study due to incomplete data.
Domestic researchers have examined the clinical utility of commonly employed serological inflammatory markers in diagnosing histological chorioamnionitis (Qian and Liu, 2020). They found that serum levels of PCT, CRP, WBC, and NE% are valuable for diagnosing histological chorioamnionitis, with the highest diagnostic accuracy achieved when these four indicators are assessed collectively. Recent studies suggest that the CLR is more sensitive and specific than other biomarkers linked to systemic inflammatory responses (Tonduangu et al., 2021).
When analyzing inflammatory markers between the two groups, no significant differences were found in WBC and CRP levels. However, NE% and CLR levels were higher in the group with body temperatures of ≥38°C compared with those with temperatures <38°C. The results from multivariate logistic regression analysis of the statistically and relatively significant indicators (NE%, CLR, and NE count) indicated that CLR exhibited a statistically significant difference between the two groups. Specifically, elevated CLR levels were associated with an increased risk of peak body temperatures of ≥38°C. Thus, CLR may serve as a reliable predictor of maternal pyrexia during labor when temperatures reach or exceed 38°C.
Conclusion
Elevated maternal pyrexia during labor, regardless of the underlying causes, can exacerbate adverse maternal and neonatal outcomes. Effective and prompt clinical management of pregnant women, particularly those with temperatures of 38°C or higher during labor, requires proactive interventions aimed at mitigating associated maternal and neonatal morbidity. The NE% and CLR are significant indicators for investigating the causes of maternal pyrexia during labor and predicting peak temperatures. These markers can be effectively leveraged to inform clinical treatment decisions.
Authors’ Contributions
Conception and design of the research: X.-F.S. and B.-Q.L. Acquisition of data: X.-F.S., P.L., Y.-L.X., and K.-H.R. Analysis and interpretation of the data: Y.-L.X. Statistical analysis: K.-H.R. and P.L. Obtaining financing: None. Writing of the article: X.-F.S. Critical revision of the article for intellectual content: B.-Q.L. All authors read and approved the final draft.
Footnotes
Acknowledgment
The authors would like to acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No external funding has been received for conducting the study.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Fujian Maternal and Child Health Hospital (2024KY208). This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.