
Abstract
Despite growing evidence supporting the efficacy of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for accidental hypothermia (AH), few studies have assessed its real-world application. We aimed to describe the use and outcomes of VA-ECMO in AH patients using data from a multicenter registry. This retrospective study included adult AH patients from the Japanese accidental hypothermia network registry (J-Point registry) between April 2011 and March 2016. We analyzed patient characteristics, in-hospital data, VA-ECMO indications, and clinical outcomes for those who received VA-ECMO. Of the 537 patients in this registry, 22 received VA-ECMO, with a median age of 80 years. Severe AH was present in 18 patients, and 10 experienced cardiac arrest (CA) on hospital arrival. VA-ECMO was indicated for CA on hospital arrival (10 patients), CA after hospital arrival (5), hemodynamic instability (5), and severe hypothermia (1), with 1 case having an unclear indication. Rewarming was successful in 18 patients, and 9 survived. Survival was higher among those with CA on hospital arrival (5/10) compared with those who developed CA after hospital arrival (1/5). This study highlights the clinical application and outcomes of VA-ECMO for AH patients using multicenter registry data. Among the 22 patients who received VA-ECMO, 9 survived. Patients with CA on hospital arrival showed better survival compared with those who developed CA after arrival, emphasizing the importance of timely VA-ECMO initiation. Further research is warranted to refine patient selection, optimize initiation timing, and evaluate long-term outcomes.
Keywords
Introduction
Accidental hypothermia (AH) is defined as a drop in core body temperature below 35°C, affecting multiple organs (Brown et al., 2012). Severe hypothermia, particularly when the core body temperature falls below 28°C, significantly impacts the cardiovascular system, causing reduced cardiac output, bradycardia, life-threatening arrhythmias, and cardiac arrest (CA), which necessitate circulatory support and rewarming (Brown et al., 2012; Dow et al., 2019). A recent nationwide survey in Japan reported that 21% of patients with AH experienced severe hypothermia, with 29% of these cases resulting in death (Takauji et al., 2021), highlighting the need for improved management strategies.
Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) plays a crucial role as life support for patients with severe cardiopulmonary failure, enabling efficient gas exchange and rewarming through extracorporeal circulation. The resuscitation guidelines from the European Resuscitation Council recommend VA-ECMO for AH patients with CA or unstable hemodynamics (Lott et al., 2021). Although recent studies have increasingly reported the efficacy of VA-ECMO (Paal et al., 2022; Takauji et al., 2023; Hymczak et al., 2023), the supporting evidence remains insufficient, particularly regarding its use in AH patients with unstable hemodynamics who have not yet experienced CA.
Furthermore, VA-ECMO is highly invasive and requires specialized knowledge and skills for proper implementation. Its application in clinical settings depends on the judgment of physicians and facilities, resulting in a lack of standardized protocols. Prior studies evaluating the efficacy of VA-ECMO are subject to selection bias and may not fully reflect actual clinical practice. Moreover, the current usage of VA-ECMO has primarily been reported in single-center case series focusing on severe hypothermia (Kosiński et al., 2017), which may not adequately represent broader clinical realities. Therefore, this study aims to detail the actual application and outcomes of VA-ECMO using the multicenter J-Point registry for AH patients.
Materials and Methods
Study design, setting, and participants
This research is a secondary analysis of the J-Point registry, which was initially established as a multicenter retrospective observational study. The study methodology has been described previously (Matsuyama et al., 2018). In summary, the J-Point registry consisted of eight centers designated as critical care medical centers (CCMCs) and four non-CCMC acute-care hospitals with an emergency department (ED) across the Kyoto, Osaka, and Shiga Prefectures in Japan. The median annual volume of ED visits for each participating institution was 19,651 (with an interquartile range of 13,281 to 27,554).
The J-point registry retrospectively included patients treated for AH in EDs from April 1, 2011, to March 31, 2016, based on the International Classification of Diseases, Tenth Revision (ICD-10) code T68 (hypothermia).
This study included adult patients aged ≥18 years with AH. We excluded patients whose body temperature was unknown or >35°C. Ethical approval for this study was obtained from the Ethics Committee of Kyoto Prefectural University of Medicine (ethical approval number: ERB-C-633-1) and other institutions.
Data collection, quality control, and outcome measurement
The methodology for collecting data has been previously described in detail (Matsuyama et al., 2018). In brief, data collection was performed using a predefined uniform datasheet. Emergency physicians trained in appropriate data extraction reviewed the patient’s charts.
The baseline characteristics of the patients included sex, age, activities of daily living (ADL) before AH (independent, requiring some assistance, or requiring total assistance), location of occurrence (indoors or outdoors), and medical history (including cardiovascular diseases, neurological diseases, endocrine diseases, psychiatric diseases, malignant diseases, dementia, others). Age was categorized into three groups as follows: adults aged 18–64 years, young-old aged 65–74 years, and old-old aged 75 years and older, based on common classifications (Ministry of Internal Affairs and Communications, 2024).
Regarding in-hospital variables, the following data were collected: vital signs on arrival at the hospital (body temperature, blood pressure, heart rate, and GCS score), electrocardiogram, biochemical data (serum pH, HCO3 [mEq/L], lactate [mmol/L], potassium [mEq/L]), associated conditions, treatment procedures, and outcomes. Body temperature was classified into three groups based on the common classification of the severity of AH as follows: mild (32.0–35.0°C), moderate (28.0–31.9°C), and severe (<28.0°C) (Brown et al., 2012). In accordance with a previous study (Japanese Association for Acute Medicine, 2013), associated conditions were classified into acute medical illness (stroke, seizure, Parkinson’s disease, thyroid disease, hypoglycemia, infectious disease, acute pancreatitis, uremia, malignant disease, bowel ischemia, rhabdomyolysis, other), traumatic injury (fall (head, spine, extremity injury), motor vehicle accident, others), alcohol intoxication, drowning (indoor, outdoor), self-harm (drug, external), and other (iatrogenic, mountain incident, burn, malnutrition/infirmity, other). The diagnoses of acute medical illness were obtained from ICD-9 or ICD-10 code in the final medical summary or medical records. Rewarming procedures were categorized into two groups as follows: active external/minimally invasive rewarming (warm intravenous fluids, warm blanket, forced warm air, heating pads, and warm bath) and active internal rewarming (lavage [stomach, chest, or bladder], intravascular hemodialysis, and extracorporeal membrane oxygenation) (Brown et al., 2012). Other treatment information included use of vasopressors (dopamine, dobutamine, noradrenaline, adrenaline, and vasopressin). Outcome data collected included rewarming success, time to rewarming success, major complications during rewarming such as ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT), decline in ADL at discharge, and in-hospital death. The primary outcome was in-hospital death, while the secondary outcomes were rewarming success and major complications during rewarming.
Statistical analysis
Based on the primary outcome, the patients were categorized into survivor or nonsurvivor. Patient characteristics, in-hospital information, and outcomes were compared using the Mann–Whitney U test for continuous variables and the Fisher’s exact test for categorical variables. All p-values were two-sided, and the significance level was set at p < 0.05. The analyses were performed using Stata/MP version 17 (StataCorp, College Station, TX, USA).
Results
Figure 1 shows patient flowchart. A total of 572 patients were registered in the J-Point registry. After excluding 27 patients with a body temperature >35°C or unknown, and 8 patients younger than 18 years, 537 adult patients with AH were included. Among these, 22 patients received VA-ECMO. A total of 118 patients with severe AH were identified, of whom 18 received VA-ECMO. Among 13 patients with both severe AH and CA on hospital arrival, 8 received VA-ECMO. In addition, among 41 patients with severe AH who were hemodynamically unstable but did not experience CA, 7 were treated with VA-ECMO.

Patient flow of this study. AH, accidental hypothermia; J-Point, Japanese accidental hypothermia network; VA-ECMO, veno-arterial extracorporeal membrane oxygenation.
Table 1 shows the patient characteristics stratified by survival status. Sixty percent of the patients were male, and the median age was 80 years. Forty percent of the patients were classified as adults, while 50% were classified as old-old. Eighty percent of the patients were independent in their ADL, and over 70% experienced the onset indoors. Approximately 90% of the patients were exposure to cold. Twenty percent had no known underlying medical conditions.
Patient Characteristics According to Survival Status
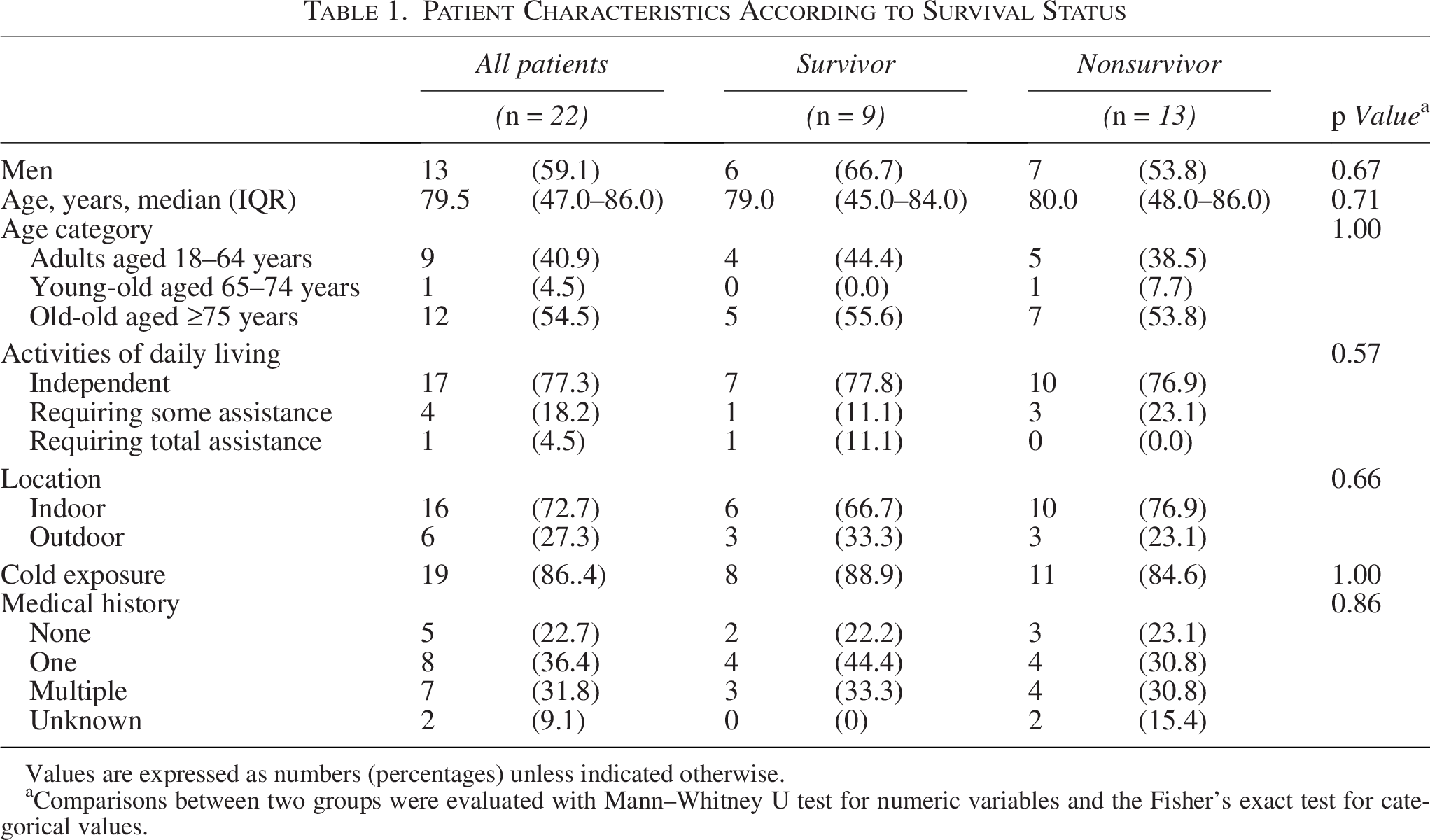
Values are expressed as numbers (percentages) unless indicated otherwise.
Comparisons between two groups were evaluated with Mann–Whitney U test for numeric variables and the Fisher’s exact test for categorical values.
Table 2 shows in-hospital data stratified by survival status. The median body temperature was 26°C, with severe hypothermia observed in 80% of the patients. In the survivor group, all patients had severe hypothermia. There were 10 patients with CA and 7 patients without CA but with hemodynamic instability. Among the nine survivors, five had CA on arrival, three had hemodynamic instability, and one had stable hemodynamics. The pH and HCO3 levels were significantly higher in the survivor group, while there were no significant differences in lactate and potassium levels. There were eight patients with acute medical illness, one patient with trauma, and three patients each with alcohol intoxication, drowning, and three patients with self-harm.
In-Hospital Data According to Survival Status
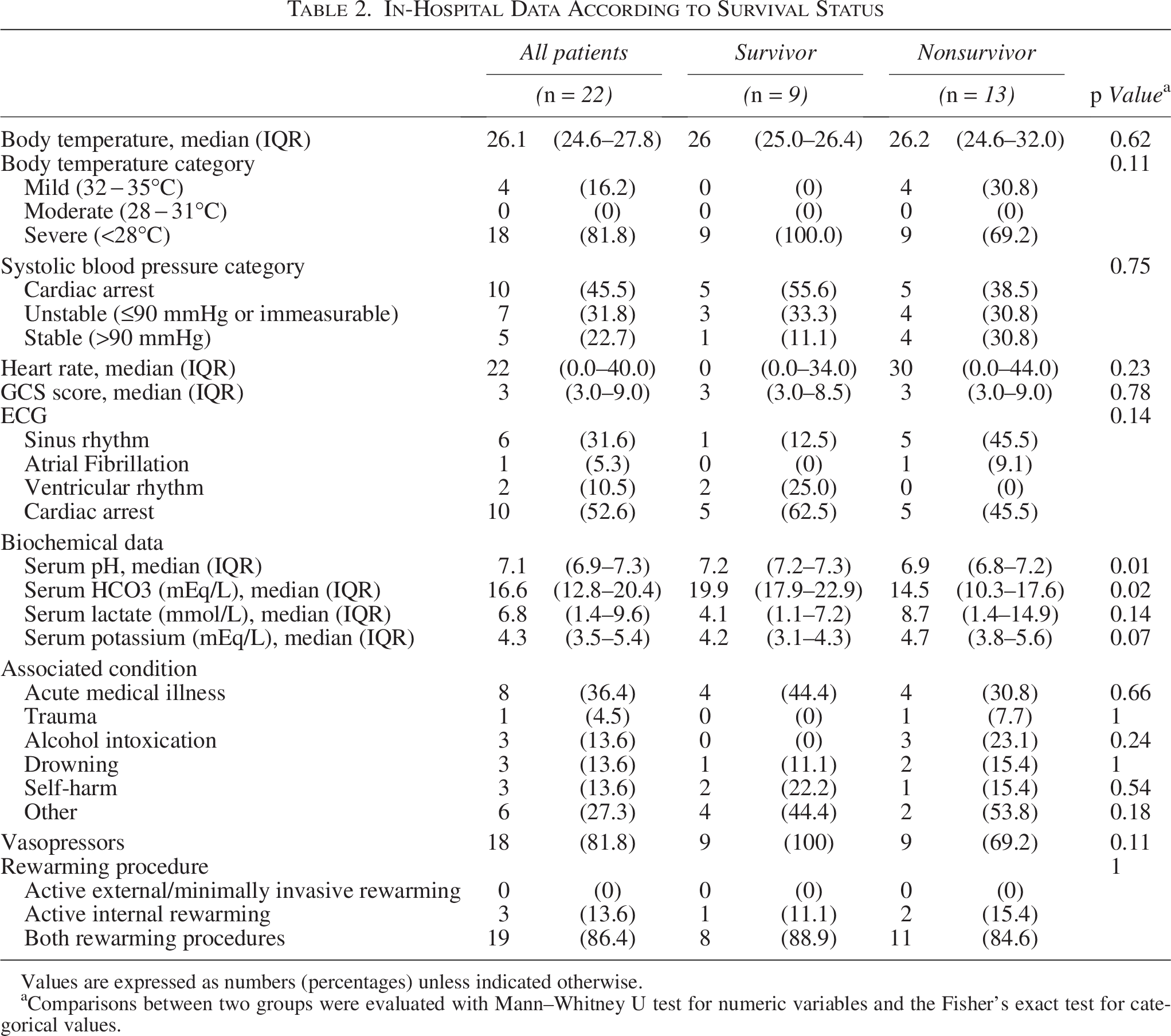
Values are expressed as numbers (percentages) unless indicated otherwise.
Comparisons between two groups were evaluated with Mann–Whitney U test for numeric variables and the Fisher’s exact test for categorical values.
Table 3 provides detailed information on 22 patients who received VA-ECMO. The ages of patients ranged from their early 20s to late 80s, with the youngest survivor being in the early 20s and the oldest in the late 80s. The male survivor in his late 80s required total assistance in ADL. Six cases occurred outdoors, including three cases of drowning, one case of alcohol intoxication, one case of sepsis, and one case of water intoxication. The lowest body temperature recorded was 21°C, with survivors having a minimum temperature of 23.4°C and a maximum of 27.9°C. The lowest pH, HCO3, and highest lactate and potassium levels in the survivor group were 7.12, 14.9 mEq/L, 9.6 mmol/L, and 5.4 mEq/L, respectively. VA-ECMO was indicated for 10 cases of CA at hospital arrival, 5 cases of transition to CA at ED, 5 cases of hemodynamic instability, 1 case of rewarming, and 1 case of unknown indication. In the survivor group, indications included five cases of CA, one case of transition to CA, and three cases of hemodynamic instability. Nine patients achieved rewarming but eventually died. Major complications included VF/VT in eight patients and bleeding in four patients.
Summary of Patients Who Underwent VA-ECMO
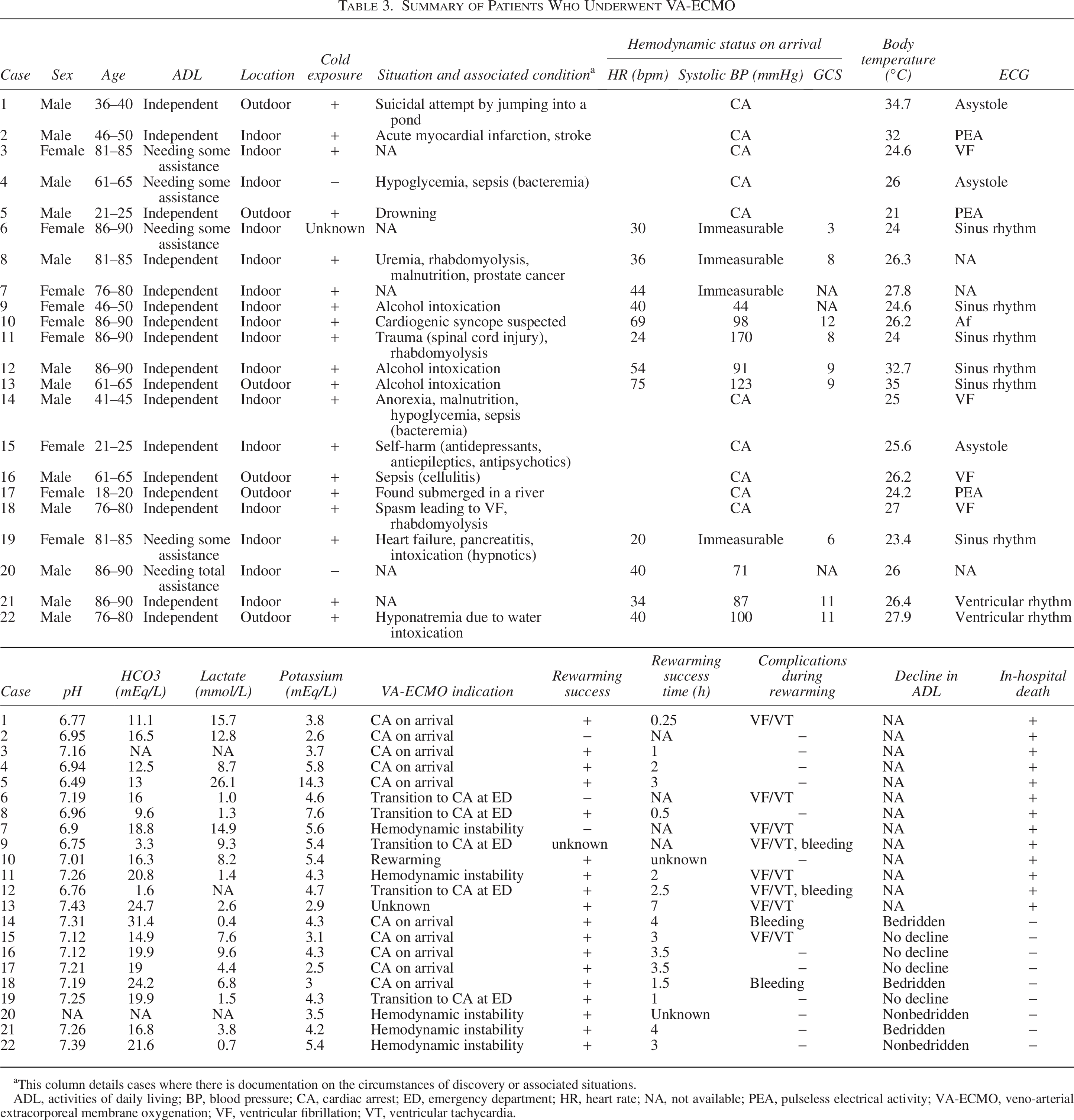
This column details cases where there is documentation on the circumstances of discovery or associated situations.
ADL, activities of daily living; BP, blood pressure; CA, cardiac arrest; ED, emergency department; HR, heart rate; NA, not available; PEA, pulseless electrical activity; VA-ECMO, veno-arterial extracorporeal membrane oxygenation; VF, ventricular fibrillation; VT, ventricular tachycardia.
Discussion
Among the 537 patients with AH in this registry, the average age of those who underwent VA-ECMO was 80 years. Among the 22 patients who received VA-ECMO, rewarming was successful in 18, with 9 survivors. The indications for VA-ECMO were CA on hospital arrival in 10 patients, transition to CA after hospital arrival in 5, hemodynamic instability in 5, severe hypothermia in 1, and in 1 case, the indication was unclear. Previous studies on the use of VA-ECMO in patients with AH in clinical practice are primarily based on case reports (Kosiński et al., 2017; Ledoux and Saint Leger, 2020). This study, utilizing a multicenter registry, provides more diverse information on cases where VA-ECMO was implemented.
The overall rate of VA-ECMO use in AH patients was 4.1% (22/537), similar to the 2.9% reported in a previous Japanese study (Takauji et al., 2021). The proportion of severe patients with AH was 22.0% (118/537), consistent with the previous study’s 21.9%. Of the 118 severe patients with AH, 18 (15.3%) received VA-ECMO, which was in line with the 10.3% reported in the prior study (Takauji et al., 2021). Among severe patients with AH and CA, who are considered the most suitable candidates for VA-ECMO, the VA-ECMO rate was 61.5% (8/13), higher than the 42.4% in the previous study, and the survival rate was 62.5% (5/8), also exceeding the 36% previously reported (Ruttmann et al., 2007). For severe patients with AH and hemodynamic instability, for whom the indication for VA-ECMO requires more cautious assessment, the VA-ECMO rate was 17.1% (7/41), although a direct comparison with previous studies was difficult. The survival rate was 42.9% (3/7), lower than the 65.9% and 69.2% reported in other studies (Takauji et al., 2023; Kosiński et al., 2017).
In this study, most indications for VA-ECMO were related to hemodynamic instability, including CA. While resuscitation guidelines recommend VA-ECMO for patients in CA, they advise a more cautious approach when considering it for patients with hemodynamic instability but no CA (Lott et al., 2021; Panchal et al., 2019). In this study, three out of five patients with hemodynamic instability but no CA survived. Prognosis appeared to vary depending on whether the CA occurred before hospital arrival or after hospital arrival. Among the 10 patients with CA on arrival, 5 survived, while 4 out of 5 patients who transitioned to CA after hospital arrival died. In patients who transitioned to CA after hospital arrival, it is possible that a lack of preparation resulted in delays in establishing VA-ECMO. For patients with hemodynamic instability, it may be prudent to have VA-ECMO on standby should CA occur.
Well-known predictors of poor prognosis include pH and potassium, which serve as surrogate markers of organ damage resulting from reperfusion injury, ischemic tissue damage, cellular lysis, and metabolic acidosis (Takauji et al., 2021; Ledoux and Saint Leger, 2020; Ruttmann et al., 2007; Pasquier et al., 2018; Saczkowski et al., 2018). In fact, in this study, patients who did not survive tended to have lower pH and higher potassium levels. These findings suggest that in cases where rewarming was achieved yet survival was not, organ damage may have become irreversible by the time rewarming was completed. The time until organ damage becomes irreversible likely varies depending not only on the severity of hypothermia, but also on individual patient conditions. Although blood tests in the ED have limitations, they may still be useful as supplementary tools when determining the indication for VA-ECMO.
In this study, the median age was 80 years, which is older compared with previous studies; however, it was consistent with studies conducted in Japan (Takauji et al., 2023; Kosiński et al., 2017; Ledoux and Saint Leger, 2020). This may reflect Japan’s aging society, where old-old account for 20% of the population (Statistics Bureau, Ministry of Internal Affairs, 2024). The resuscitation guidelines do not specify an age cutoff for VA-ECMO indication in patients with AH (Lott et al., 2021; Panchal et al., 2019). Although some studies identify ≥75 years or poor ADL as predictors of poor prognosis (Takauji et al., 2021; Pasquier et al., 2018), the oldest survivor in this study was a male in his late 80s who required full assistance with ADL, and another survivor was a 95-year-old male (Carlsen et al., 2017). When considering the initiation of VA-ECMO, decisions may not need to be based solely on age, as other factors such as the initial evaluation and other poor prognostic factors are also important.
This study has several limitations. First, differences in the criteria for VA-ECMO initiation and operational protocols across facilities may have influenced the results. However, in most cases, the indication for VA-ECMO followed established resuscitation guidelines. Second, this study lacked information regarding time to VA-ECMO initiation. While the time to rewarming success was available, the time to VA-ECMO initiation is likely to have a greater impact on prognosis. Third, there was a lack of data on long-term outcomes. This study only assessed in-hospital mortality, without information on long-term survival.
Conclusion
This study evaluated the use of VA-ECMO for AH patients using multicenter registry data. Among the 22 patients who received VA-ECMO, 9 survived. Patients with CA on hospital arrival showed better survival compared with those who developed CA after arrival, emphasizing the importance of timely VA-ECMO initiation. Further research is warranted to refine patient selection, optimize initiation timing, and evaluate long-term outcomes.
Authors’ Contributions
T.S. had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis. Study concept and design: T.S. and T.M. Acquisition, analysis, and interpretation of data: All authors. Drafting of the article: T.S. and T.M. Critical revision of the article for important intellectual content: All authors. Statistical analysis: T.S., Y.M., and T.M. Obtained funding: Y.O. Study supervision: T.M. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors express their profound gratitude to all members of the J-Point registry group for their valuable contribution.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
Y.O. received a research grant from the ZOLL Foundation (2022) and overseas scholarships from the Japan Society for Promotion of Science (202360092), the FUKUDA Foundation for Medical Technology (20220613), and the International Medical Research Foundation (20221001). These organizations have no role in conducting this study.