
Abstract
We aimed to evaluate the efficacy of peritoneal dialysis (PD) in hypoxic–ischemic acute kidney injury (AKI) in newborns with hypoxic–ischemic encephalopathy (HIE) who underwent therapeutic hypothermia (TH). This was a retrospective study including the newborns with HIE/TH who developed hypoxic–ischemic AKI and underwent PD between January 2022 and June 2024. The blood test results obtained before starting PD were compared with the blood test results obtained just before the decision to terminate PD or, in case of death, with the final blood test results obtained before death. Twenty-one newborns were included in the study. Four (19%) of these newborns were diagnosed with moderate HIE, and 17 (81%) were diagnosed with severe HIE. The median gestational age of the patients was 38 (36–39) weeks, and the mean birth weight was 3083 ± 494 g. The median postnatal day when PD started was 3 (2–4) days and its duration was 7 (4–10) days. All patients had fluid overload as an indication for PD dialysis, and fluid overload was accompanied by hyperkalemia in 8 (38.1%) patients. After PD, blood pH, bicarbonate, and sodium values increased significantly (p ≤ 0.001, 0.009, <0.001, respectively), and potassium, phosphorus, and creatinine values decreased significantly (p ≤ 0.001, <0.001, 0.031, respectively) compared with the predialysis values. PD corrects acidosis and electrolyte imbalance and may be considered as a successful renal replacement therapy for hypoxic–ischemic AKI in neonates with HIE/TH, especially in units with limited resources.
Keywords
Introduction
Hypoxic–ischemic encephalopathy (HIE) is an important cause of morbidity and mortality, and newborns with HIE are at risk for hypoxic–ischemic multiple organ dysfunction, including acute kidney injury (AKI) (Kurinczuk et al, 2010; Jacobs et al, 2013; Coleman et al, 2022; Shah et al, 2004). The presence of hypoxic–ischemic AKI results in additional increases in morbidity and mortality in these high-risk babies (Kurinczuk et al, 2010; Jacobs et al, 2013; Coleman et al, 2022; Gupta et al, 2016; Durkan and Alexander, 2011; Selewski et al, 2013; Karlowicz and Adelman, 1995; Kaur et al, 2011; Hankins et al, 2002; Kirkley et al, 2019). AKI is associated with the severity of HIE and thus with the worst short- and long-term outcomes, such as increased duration of mechanical ventilation, length of neonatal intensive care unit (NICU) stay, in-hospital mortality, abnormal post-cooling brain magnetic resonance imaging findings, and adverse neurodevelopmental outcomes, even during the therapeutic hypothermia (TH) era (Selewski et al, 2013; Sarkar et al, 2014; Cavallin et al, 2020; Hadzimuratovic et al, 2014). In addition, long-term follow-up of survivors is important in terms of chronic kidney disease (CKD), because newborns diagnosed with AKI are at risk for CKD (Chaturvedi et al, 2017). Prediction of AKI in neonates with HIE is of utmost importance. Studies evaluating perinatal risks for AKI, the knowledge about the decline rate of serum creatinine levels in the first week of life, renal oxygen saturations measured with near-infrared spectroscopy, and the use of serum neutrophil gelatinase-associated lipocalin and cystatin C in addition to serum creatinine and urine output may help early recognition of newborns who will develop AKI and/or need renal replacement therapy (RRT) (Gupta et al, 2016; Kirkley et al, 2019; Bozkurt and Yucesoy, 2021; Chock et al, 2018; Nour et al, 2020).
TH reduces mortality and rates of neurological sequelae in newborns with moderate to severe HIE, and the decreased frequency of AKI in newborns with HIE in the TH era compared with the pre-TH era suggests that TH also has a renal protective effect (Kurinczuk et al, 2010; Jacobs et al, 2013; Nour et al, 2020; Tanigasalam et al, 2016). In the pre-TH era, the rate of AKI was reported to be as high as 72% in newborns with neonatal encephalopathy due to birth asphyxia (Hankins et al, 2002). In the TH era, the rate of hypoxic–ischemic AKI in neonates with HIE is 10–42% (Selewski et al, 2013; Kirkley et al, 2019; Sarkar et al, 2014; Cavallin et al, 2020; Bozkurt and Yucesoy, 2021; Chock et al, 2018; Nour et al, 2020; Tanigasalam et al, 2016). The difference in AKI rates between different studies is speculated to be mainly due to the differences in the AKI criteria used in the studies and the difference in neonatal care in the centers where the studies were conducted (Selewski et al, 2013; Kirkley et al, 2019; Sarkar et al, 2014; Cavallin et al, 2020; Bozkurt and Yucesoy, 2021; Chock et al, 2018; Nour et al, 2020; Tanigasalam et al, 2016). Currently, the Neonatal Modified Kidney Disease: Improving Global Outcomes (KDIGO) criteria are commonly used to define and classify neonatal AKI, but the sensitivity of the neonatal modified KDIGO criteria in neonates with HIE/TH is controversial (Coleman et al, 2022; Jetton and Askenazi, 2012; Jetton et al, 2017).
While supportive treatments such as fluid restriction and avoidance of nephrotoxic drugs are sufficient in early-stage AKI, RRT is needed in cases where advanced-stage AKI develops and supportive treatment fails. In studies evaluating newborns with hypoxic–ischemic AKI, there was a limited number of reported cases requiring RRT (Coleman et al, 2022; Selewski et al, 2013; Tanigasalam et al, 2016; Ustyol et al, 2016). The effectiveness and safety of RRT in the presence of advanced hypoxic–ischemic AKI are unknown. In this study, we aimed to evaluate the short-term efficacy of peritoneal dialysis (PD) in hypoxic–ischemic AKI in newborns with HIE who underwent TH.
Methods
This was a retrospective cross-sectional study including the newborns with HIE/TH who developed hypoxic–ischemic AKI and underwent PD between January 2022 and June 2024. Ethical approval for the study was obtained from Harran University Clinical Research Ethics Committee (date: August 26, 2024, number: 21.12.33). The study was completed in accordance with the Declaration of Helsinki as revised in 2013. Given the retrospective nature of the study, informed consent was not obtained.
TH protocol
The criteria for TH were as follows: newborns with a gestational age of ≥36 weeks and aged below ≤6 hours, a pH value of ≤7.00 or base excess (BE) value of ≤−16 mmol/L in the blood sample collected from the cord or in the blood sample collected from the baby in the first hour of life, a 10th-minute Apgar score of <5 or persisting need for resuscitation, and signs of moderate or severe encephalopathy on clinical evaluation (Akisu et al, 2018; Papile et al., 2014). Cooling to a rectal temperature of 33.5 ± 0.5°C was tried to be achieved in all newborns within the postnatal 6 hours. Rewarming to 36.5°C was started following 72-hour cooling by elevating the temperature at a rate of 0.5°C per hour. The Sarnat and Sarnat staging system was used to determine the stage of HIE (stage 1—mild, stage 2—moderate, or stage 3—severe HIE). Neonates with HIE/TH were closely monitored for hypoxic–ischemic multiple organ dysfunction.
PD indications and follow-up
The Neonatal Modified KDIGO criteria were used to diagnose and classify AKI (Jetton et al, 2017; Acute Kidney Injury Work Group, 2013). PD was applied to the patients diagnosed with stage III AKI according to KDIGO. The KDIGO criteria for stage 3 were as follows: rise in serum creatinine ≥3 times with respect to basal creatinine, or creatinine ≥2.5 mg/dL, or need for dialysis, or urinary output <0.3 mL/kg/h for ≥24 hours, or anuria for ≥12 hours. The main indications for PD in this study were fluid overload due to oliguria/auria and electrolyte imbalance in the presence of hypoxic–ischemic AKI. Fluid support was provided taking into account insensible fluid loss and ongoing fluid losses. Antipotassium treatment consisting of sodium bicarbonate, furosemide, insulin, dextrose, kayexalate, as well as calcium treatment was applied if there were electrocardiographic findings of hyperkalemia. PD was initiated in patients whose fluid overload continued despite fluid restriction and whose potassium level was above 6 mmol/L after antipotassium treatment.
Drug doses of all newborns diagnosed with AKI were adjusted, and nephrotoxic drugs were discontinued if possible. In our unit, in the presence of AKI, penicillin and cephalosporin group antibiotics were used in early sepsis, and vancomycin and cefepime or vancomycin and meropenem were used in late sepsis. The fluid intake output and weight of the newborns were closely monitored, and kidney functions, blood gases, and electrolytes were checked when necessary. A urinary catheter was placed in all newborns diagnosed with AKI to monitor urine output, and urine volumes were recorded at least eight times a day, and body weights were recorded at least two times a day.
The only available RRT modality was PD at the center where the study was conducted. Indications for PD were pathological fluid overload, refractory metabolic acidosis, and electrolyte imbalance despite medical therapy in the presence of AKI. Before deciding on PD, all supportive treatments such as fluid restriction, antipotassium therapy, and hemodynamic and respiratory support were applied (Coleman et al, 2022; Nourse et al, 2021). All PD catheters were inserted by pediatric surgeons in the NICU as a bedside procedure under sterile conditions, under sedation and analgesia, and began to be used immediately after insertion (Gerçel and Anadolulu, 2023). The initial PD fill volume was 10 mL/kg and gradually increased to 20 mL/kg as tolerated. The initial exchange duration was 60 minutes, including inflow, dwell, and drain as 15, 30, and 15 minutes, respectively. At some point, the dwell time was gradually prolonged to 90 minutes as appropriate. The exchange process was performed 8–24 times per day, depending on the newborns’ needs. The dextrose concentration of the preferred initial PD solution was 1.36%, and 2.27% or 3.86% PD solutions (Baxter Healthcare, USA) were available in our hospital to be used as needed. In the presence of weak ultrafiltration, a three-step improvement procedure was applied respectively after ruling out peritoneal leakage: (1) fill volume was increased to 20 mL/kg, (2) dwell time was reduced by 25% if the cycle time was longer than 60 minutes, and if ultrafiltration could not be increased, (3) glucose concentration was first increased to 2.27% and finally increased to 3.86% (Nourse et al, 2021). A manual gravity-based open system was used for PD. Heparin, antibiotics, or potassium chloride was added to the PD solutions according to the needs of the newborns.
The dialysis protocol was the same for all patients, but PD duration varied on a case-by-case basis. When patients started to urinate over 1 mL/kg/h, PD was discontinued by gradually reducing the number of daily PD cycles, taking into account blood urea, serum creatinine, blood gas, and electrolyte values. PD catheters of the patients, who did not have a decrease in urine output, an increase in blood urea and serum creatinine values, and acidosis or electrolyte imbalance within 48–72 hours after stopping PD, were removed in the NICU using a sterile technique.
The patients’ gestational ages, birth weights, genders, 1st and 5th min Apgar scores, cord blood gas values, HIE stages, respiratory support and inotropic needs, attenuated electroencephalography (aEEG) findings, admission blood biochemistry, and complete blood count results were recorded. Indications for PD, postnatal day when PD was started, duration of PD, PD catheter complications, other accompanying diseases, length of NICU stay, anticonvulsant drug use, and outcomes as survival death were extracted from the patients’ files. Inotrope treatments were planned individually according to echocardiography findings and the presence of accompanying diseases such as sepsis and persistent pulmonary hypertension (PPHT). Blood gas values, glucose, sodium, potassium, calcium, phosphorus, blood urea, and serum creatinine levels were assessed daily. In the study, the blood results obtained at 24 hours of life (admission), the last blood test results obtained just before starting PD and before the decision to terminate PD or in case of death, the final blood test results obtained were analyzed. All HIE/TH neonates were monitored with aEEG during the TH and rewarming periods. The aEEG recordings were grouped as normal (continuous pattern and discontinuous pattern) and abnormal (burst suppression pattern, low-voltage pattern, and isoelectric pattern). All patients underwent routine echocardiography.
Statistical analysis
The IBM Statistical Package for Social Sciences version 20.0 was used for statistical analyses. The normality was assessed using the Kolmogorov–Smirnov test, Shapiro–Wilk test, Q-Q plot, skewness, and kurtosis. Categorical variables were expressed as frequency and percentage. Normally distributed continuous variables were expressed as mean ± standard deviation and non-normally distributed variables were expressed as median (minimum–maximum). The Friedman test was used for the analysis of the continuous variables. The Durbin–Conover test was used for post hoc analysis. A p-value of <0.05 was considered statistically significant.
Results
During the study period, TH was performed on 371 newborns who had a diagnosis of HIE in our NICU. Of these patients, 130 (35%) patients were diagnosed with AKI, 69 (53%) of whom had stage 1 AKI, 40 (30.8%) had stage 2 AKI, and 21 (16.2%) had stage 3 AKI. PD was performed in the 21 (5.7%) newborns diagnosed with stage 3 hypoxic–ischemic AKI, no patient with stage 3 AKI had a contraindication for PD, and all patients who underwent PD were included in the study. The median gestational age of the patients was 38 (36–39) weeks, and the mean birth weight was 3083 ± 494 g. Four (19%) of the newborns were diagnosed with stage 2 HIE, and 17 (81%) were diagnosed with stage 3 HIE. All newborns had abnormal aEEG and were receiving inotropes, and 13 (61.9%) of them died. All patients, who died, had stage 3 HIE and comorbid diagnoses of PPHT. The median postnatal day at which PD began was 3 (2–4) days, and the duration of PD was 7 (4–10) days. All patients had fluid overload as an indication for PD dialysis, and fluid overload was accompanied by intractable hyperkalemia in 8 (38.1%) patients. Demographic and clinical characteristics of the newborns with hypoxic–ischemic AKI, who underwent PD, are presented in Table 1.
Demographic and Clinical Characteristics of Newborns with Hypoxic–Ischemic Acute Kidney Injury Who Underwent Peritoneal Dialysis (n = 21)
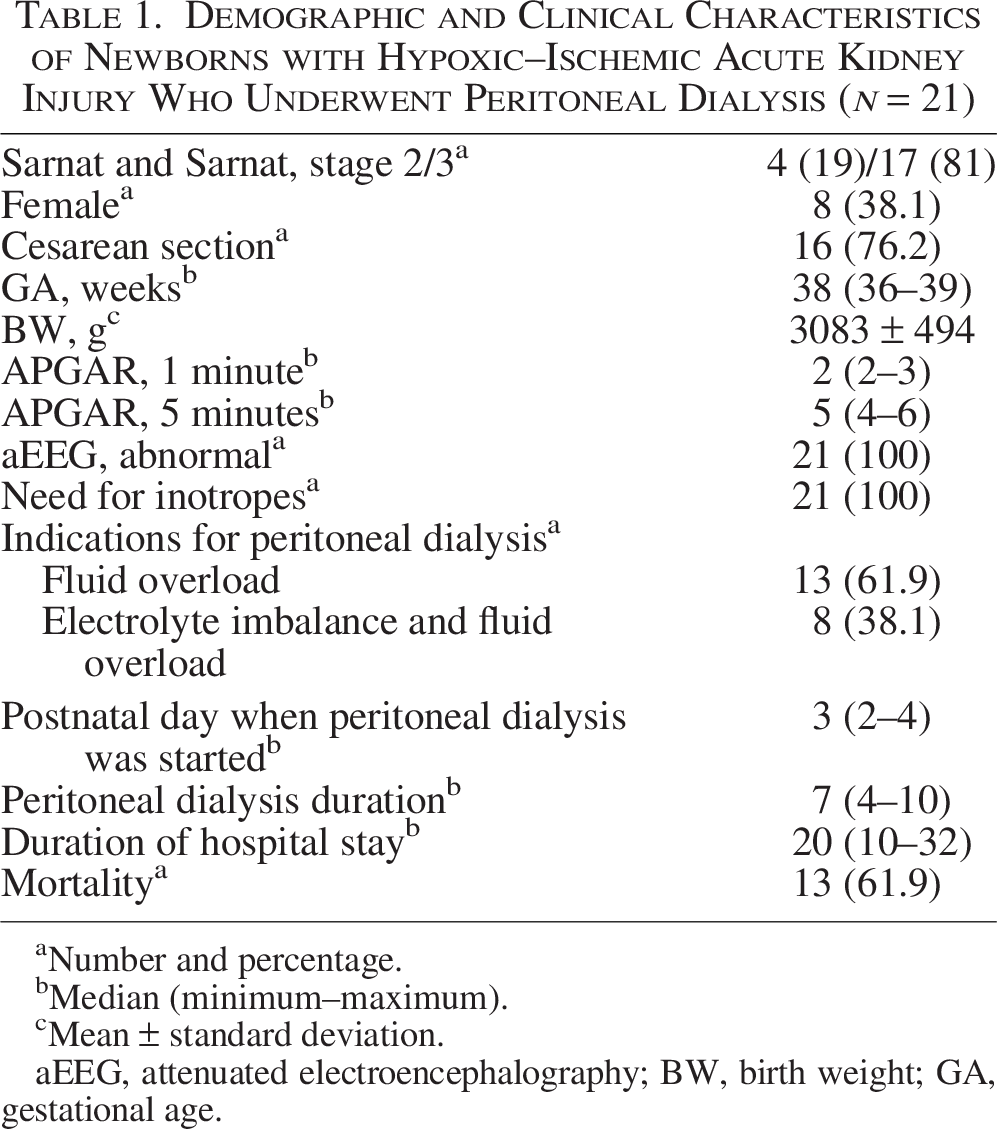
Number and percentage.
Median (minimum–maximum).
Mean ± standard deviation.
aEEG, attenuated electroencephalography; BW, birth weight; GA, gestational age.
At the time of PD, all patients were intubated and receiving systemic antibiotic therapy. PPHT was detected in 14 (66.6%) newborns, and PPHT was accompanied by pulmonary hemorrhage in one of these newborns, pneumothorax in two, and sepsis in another two newborns. Klebsiella pneumonia grew in the blood culture of these two patients, and these patients were successfully treated for sepsis during the PD period. Two (9.5%) newborns developed complications related to PD, one of which was catheter revision due to leakage of the PD catheter, and the other was Candida peritonitis. The patient with C. peritonitis required early termination of PD and the patient died. In other patients, PD was discontinued either because it was no longer needed or because the patient died. Laboratory results on admission in the newborns with hypoxic–ischemic AKI who underwent PD are presented in Table 2.
Laboratory Results on Admission in Newborns with Hypoxic–Ischemic Acute Kidney Injury Who Underwent Peritoneal Dialysis (n = 21)

Median (minimum–maximum).
Mean ± standard deviation.
Comparison of the laboratory values at the time of admission, before PD, and after PD is presented in Table 3. Post hoc analysis revealed significant differences in pH, with all pairwise comparisons showing p-values of <0.001. For BE, admission predialysis as well as admission and postdialysis comparisons were significant (p < 0.001), while predialysis and postdialysis values did not differ significantly (p = 0.074). Bicarbonate levels showed a significant increase between predialysis and postdialysis values (p = 0.009), but no significant differences were found in the other pairwise comparisons. Lactate levels showed a significant reduction between admission and predialysis and postdialysis values (p < 0.001 for both), while predialysis and postdialysis differences were not significant (p = 0.136). Sodium levels significantly changed between admission and predialysis values (p = 0.002) and between predialysis and postdialysis values (p < 0.001), while admission and postdialysis values did not differ significantly (p = 0.084). Potassium levels showed a significant reduction between admission and predialysis values (p = 0.002) and predialysis and postdialysis values (p < 0.001), but not between admission and postdialysis values (p = 0.191). Calcium levels showed significant differences only between admission and predialysis values (p = 0.014). Phosphorus levels significantly changed in all pairwise comparisons (p < 0.05 for all). Blood urea showed a significant reduction between admission and predialysis values and between admission and postdialysis values (p < 0.001 for both), but no significant change was observed between predialysis and postdialysis values (p = 0.852). Finally, creatinine levels significantly decreased across all pairwise comparisons, with p-values of <0.05 for all.
Comparison of Laboratory Values (N = 21)
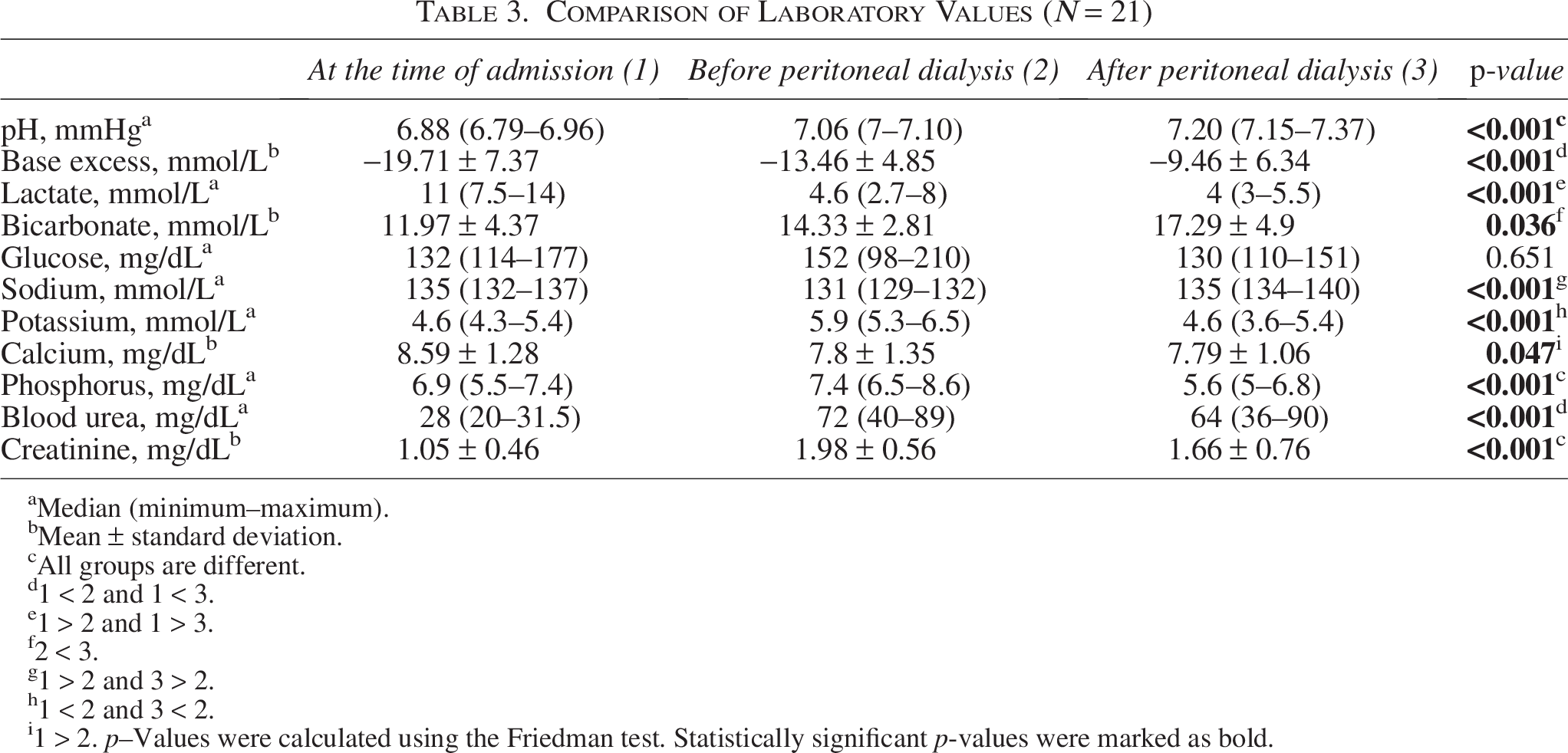
Median (minimum–maximum).
Mean ± standard deviation.
All groups are different.
1 < 2 and 1 < 3.
1 > 2 and 1 > 3.
2 < 3.
1 > 2 and 3 > 2.
1 < 2 and 3 < 2.
1 > 2. p–Values were calculated using the Friedman test. Statistically significant p-values were marked as bold.
Discussion
In this study, in which we investigated the short-term effect of PD in newborns with hypoxic–ischemic AKI and HIE who underwent TH, the rate of AKI was 35%, the frequency of need for PD was 5.7%, and the main PD indication was fluid overload. In the limited number of studies, in which we could calculate the frequency of RRT requirement in newborns with HIE/TH, we found that the frequency of RRT requirement was 2.5–3.1% (Selewski et al, 2013; Sarkar et al, 2014). The high PD requirement rate in our study may be due to the high rate of severe HIE in our NICU, since severe HIE always results in multiple organ dysfunction (Shah et al, 2004). The mortality rate in this study was 61.9%, and mortality occurred in newborns with both severe HIE and PPHT. Selewski et al. reported that the AKI rate was 38%, and the RRT rate was 3.1%, and only one in three newborns, who underwent RRT, survived (Selewski et al, 2013). Leakage and catheter-related peritonitis were the complications of PD in our study.
In our study, it was observed that pH, bicarbonate, and sodium values increased and potassium, phosphorus, and creatinine values decreased significantly after PD in newborns with AKI/HIE/TH when the last blood test results obtained just before PD was initiated and just after PD was terminated, or before death if the newborn died during PD, were compared. Since the postdialysis blood results of only four newborns were taken before the decision to terminate PD was made, because the patients died, it can be said that PD was successful in correcting acidosis and electrolyte imbalance in this patient group. On the contrary, we speculated that the high mortality rate in our patients, even if acidosis and electrolyte imbalance improved with PD, might be due to other accompanying morbidities such as severe HIE, PPHT, and sepsis. There are a few reported cases in the literature in which PD was performed due to hypoxic–ischemic AKI, and therefore, the effectiveness, safety, and short- and long-term results of PD in this patient group are not known yet (Coleman et al, 2022; Selewski et al, 2013; Tanigasalam et al, 2016; Ustyol et al, 2016; Starr et al, 2021).
There are studies investigating the predictive factors of hypoxic–ischemic AKI, appropriate diagnostic criteria, treatment method, and short- and long-term outcomes in newborns with HIE/TH (Gupta et al, 2016; Kirkley et al, 2019; Sarkar et al, 2014; Cavallin et al, 2020; Hadzimuratovic et al, 2014; Chaturvedi et al, 2017; Bozkurt and Yucesoy, 2021; Chock et al, 2018; Nour et al, 2020; Tanigasalam et al, 2016). AKI in newborns with HIE/TH was found to be associated with being outborn, intrauterine growth restriction, or having meconium-stained amniotic fluid, and low admission temperature, and baseline and 12-hour lactate levels have been suggested to predict the risk of AKI in neonates with HIE/TH (Kirkley et al, 2019; Bozkurt and Yucesoy, 2021). Renal oxygenation has been speculated to be used as an early marker of AKI in neonates with HIE/TH, and neonates with AKI have been shown to have higher renal oxygen saturations and lower renal fractional tissue oxygen extraction during cooling compared to those without AKI; this reflects impaired oxygen extraction by the injured kidney (Chock et al, 2018). In studies on hypoxic–ischemic AKI, we did not find any studies evaluating the effectiveness and safety of RRT in AKI, and we emphasized that this important problem faced by health care professionals, especially in NICUs with limited facilities, can be solved with PD, which can be applied everywhere. However, there are still too many questions to be answered regarding the timing of PD, the effect of PD on mortality and morbidity, and so forth.
Gupta et al. suggested that Neonatal Modified KDIGO criteria cannot detect all cases of early-stage AKI in HIE/TH newborns during the first week of life and that the rate of decline in serum creatinine may help identify these cases of AKI. They found that a >50% decrease in serum creatinine and/or a serum creatinine level below 0.6 mg/dL in the first week of life was associated with favorable outcomes (Gupta et al, 2016). Nour et al. showed that TH reduced the rate of AKI in neonates with HIE and showed that neutrophil gelatinase-associated lipocalin and cystatin C levels remained elevated despite improvement in serum creatinine and urine output, indicating ongoing renal damage (Nour et al, 2020). This suggested that additional markers were needed for the diagnosis of AKI and for follow-up in this patient group. Tanigasalam et al. showed that TH significantly reduced the incidence and severity of AKI and mortality in term newborns with HIE (Tanigasalam et al, 2016). Sarkar et al. found that newborns with AKI/HIE/TH had 2.9 times higher odds of abnormal postcooling magnetic resonance imaging at 7–10 postnatal days than those without AKI, even after controlling for other risk factors, demographics, and interventions associated with perinatal asphyxia (Sarkar et al, 2014). In addition, Cavallin et al. found that AKI in neonates with HIE/TH was an indicator of long-term disability or mortality (Cavallin et al, 2020). Chaturvedi et al. emphasized the importance of longitudinal follow-up of neonatal AKI cases throughout childhood for timely diagnosis and intervention for possible CKD (Chaturvedi et al, 2017). It is obvious that hypoxic–ischemic AKI is an important cause of short- and long-term morbidities and even mortality, and therefore, it would be beneficial to urgently plan multicenter and prospective studies on every aspect of this subject.
Our study has some limitations. The main limitation was that the cross-sectional retrospective design of the study did not allow us to evaluate the long-term effect of AKI on neonates with HIE/TH. The second limitation was the small sample size and lack of power analysis. The third limitation was that the metabolic test results were not evaluated in our study as some cases with HIE might have an underlying congenital metabolic disease that could affect the prognosis. On the contrary, the inclusion of the largest group of patients with hypoxic–ischemic AKI/HIE/TH, who underwent PD, was the strength of our study.
Conclusions
In conclusion, PD may be considered a successful RRT for hypoxic–ischemic AKI in neonates with HIE/TH, especially in units with limited resources. PD effectively corrects acidosis and electrolyte imbalance in these high-risk newborns without an obvious metabolic side effect. Future longitudinal studies involving large numbers of patients from multiple centers using the same definition of AKI are needed to clarify the effectiveness and safety of PD in neonates with hypoxic–ischemic AKI undergoing TH.
Authors’ Contributions
A.O.G.: Conceptualization, methodology, formal analysis, writing, original draft, review, and editing (lead). A.B.: Methodology and original draft.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.