
Abstract
Therapeutic hypothermia is a critical intervention in post-cardiac arrest care, yet the optimal cooling method remains debatable. This prospective, single-center study compared the efficacy of a novel craniocerebral hypothermia helmet with the Arctic Sun 5000 surface cooling system in post-cardiac arrest patients. Thirty-four comatose survivors of cardiac arrest were randomized to receive either craniocerebral hypothermia (n = 17) or peripheral surface cooling (n = 17). Target temperature management (32–34°C) was initiated within 30–120 minutes of return of spontaneous circulation and maintained for 36–48 hours. Craniocerebral hypothermia demonstrated significantly faster cooling initiation (32.9 ± 13.5 vs. 238 ± 25.7 minutes, p < 0.001) compared with peripheral cooling, while both methods achieved similar target temperature maintenance. The craniocerebral group showed better preservation of renal function and electrolyte stability, with significantly lower increases in serum creatinine and urea levels (p < 0.001). Hospital stays were notably shorter in the craniocerebral group (13 ± 7 vs. 24.29 ± 31 days, p < 0.001). While both methods achieved comparable survival rates, the craniocerebral group exhibited a lower incidence of seizures (17.6% vs. 66.6%) and improved neurological outcomes based on Cerebral Performance Category scores though not reaching statistical significance. These findings suggest that craniocerebral hypothermia offers advantages in terms of rapid cooling initiation, physiological stability, and reduced hospital stay, representing a promising alternative for targeted temperature management in post-cardiac arrest care. The enhanced practicality and comparable efficacy of this approach warrant further investigation through larger multicenter trials.
Keywords
Introduction
Post-cardiac arrest syndrome represents a complex pathophysiological state characterized by multiple organ dysfunction, with the brain being particularly vulnerable to ischemia–reperfusion injury. Despite significant advances in resuscitation techniques, neurological damage remains the predominant cause of mortality and long-term disability among survivors. Therapeutic hypothermia, now more broadly termed as targeted temperature management (TTM), has emerged as a cornerstone intervention in post-cardiac arrest care, demonstrating significant neuroprotective effects through multiple mechanisms including reduction of cerebral metabolism, inflammation, and oxidative stress (Callaway et al., 2015).
The evolution of TTM has witnessed the development of various cooling methodologies, each with distinct advantages and limitations. Traditional systemic cooling approaches, while effective, often present challenges including delayed target temperature achievement, significant resource utilization, and systemic complications such as shivering, coagulopathy, and infection risks (Polderman, 2009). These limitations have driven innovation toward more targeted cooling strategies, particularly focused on selective cerebral temperature management.
Recent technological advances have facilitated the development of specialized cooling devices, including craniocerebral cooling systems and surface cooling devices such as the Arctic Sun 5000. Craniocerebral hypothermia represents a novel approach that directly targets the brain, potentially offering more rapid and focused cooling while minimizing systemic complications. In contrast, the Arctic Sun 5000 system utilizes advanced surface cooling technology to achieve whole-body temperature management through precisely controlled skin cooling pads (Zhang et al., 2016).
Despite these technological developments, comparative data regarding the efficacy, safety, and clinical outcomes of different cooling methods remain limited. Previous studies have primarily focused on comparing invasive versus noninvasive cooling methods, with limited investigation of targeted cranial cooling approaches (Nielsen et al., 2013). The optimal method for inducing and maintaining therapeutic hypothermia, particularly concerning speed of cooling, maintenance of target temperature, and associated complications, remains a subject of ongoing investigation.
This study aims to address this knowledge gap by comparing the efficacy and safety profiles of craniocerebral hypothermia using a thermoelectric cooling helmet versus peripheral cooling with the Arctic Sun 5000 system in post-cardiac arrest patients. Our investigation specifically focuses on the following:
Speed and precision of target temperature achievement. Maintenance of therapeutic hypothermia. Neurological outcomes and survival rates. Associated complications and physiological effects. Resource utilization and practical implementation aspects.
Through this comparative analysis, we seek to provide evidence-based insights to optimize cooling strategies in post-cardiac arrest care, potentially improving patient outcomes while minimizing complications and resource utilization.
Methods
Study design and ethical considerations
This prospective, single-center, comparative cohort study was conducted between January 2023 and December 2024 at our institution’s intensive care unit. The study protocol received approval from the institutional review board (approval number: 71306642-050.01.04/2020) and was conducted in strict accordance with the Declaration of Helsinki. Written informed consent was obtained from legal representatives of all participants before enrollment in the study, with detailed documentation of the consent process maintained in patient records.
Patient selection and enrollment
Our study population consisted of adult patients who achieved return of spontaneous circulation (ROSC) following cardiac arrest. Patients were eligible for inclusion if they were 18 years or older, remained comatose (Glasgow Coma Scale score ≤9) after ROSC, and were candidates for therapeutic hypothermia. We specifically excluded patients with preexisting terminal illness, active malignancy, severe systemic comorbidities, pregnancy, or admission body temperature below 30°C. Additionally, patients with major surgery within the previous 72 hours or severe bleeding diathesis were not considered for enrollment.
Randomization and treatment protocol
Using a computer-generated randomization sequence, eligible patients were assigned in a 1:1 ratio to receive either craniocerebral hypothermia via the thermoelectric cooling helmet (Fig. 1) or peripheral cooling using the Arctic Sun 5000 system. Treatment was initiated within 30–120 minutes of ROSC in both groups, with a target temperature range of 32–34°C maintained for 36–48 hours.

Thermoelectric hypothermia helmet.
Cooling methods and temperature management
Craniocerebral hypothermia group
In the craniocerebral hypothermia group, the thermoelectric cooling helmet was applied according to manufacturer specifications. Temperature monitoring was conducted continuously using both esophageal and in-helmet sensors. The cooling system was programmed to achieve and maintain the target temperature range while preventing overcooling. Rewarming was conducted at a controlled rate of 0.25–0.5°C per hour until normothermia was achieved.
Peripheral cooling group
Patients in the peripheral cooling group received treatment with the Arctic Sun 5000 system using surface cooling pads applied to the torso and extremities. Temperature was monitored via an esophageal probe, with the system automatically adjusting to maintain the target temperature range. The rewarming protocol matched that of the craniocerebral group to ensure comparable temperature management between groups.
Clinical monitoring and data collection
All patients underwent comprehensive monitoring throughout the study period. Vital signs, including core temperature, blood pressure, heart rate, and oxygen saturation, were continuously recorded. Neurological assessments were performed every 4 hours, and laboratory tests including complete blood count, renal and liver function tests, coagulation profile, arterial blood gases, and electrolytes were obtained daily. Continuous electroencephalographic (EEG) monitoring was maintained during the cooling phase to detect seizure activity and assess cerebral function. In most patients, cardiac arrest occurred secondary to acute coronary syndrome. Therefore, during the acute phase, guideline-recommended anti-ischemic therapy was initiated, consisting of dual antiplatelet therapy (aspirin and a P2Y12 inhibitor), anticoagulation, beta-blockers, and statins. Additionally, ACE inhibitors or ARBs were administered when clinically indicated.
Outcome assessment
The primary outcome measures encompassed the time to achieve target temperature, temperature stability during the maintenance phase, neurological recovery as assessed by Cerebral Performance Category (CPC) scores, and in-hospital mortality. Secondary outcomes included the incidence of complications, duration of mechanical ventilation, length of intensive care unit and hospital stay, and changes in renal function parameters. Neurological outcomes were evaluated at hospital discharge using both the CPC scale and Modified Rankin Scale.
Statistical analysis
Data analysis was performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). We assessed normality of continuous variables using the Shapiro–Wilk test. Continuous data were expressed as means ± standard deviations or medians with interquartile ranges based on their distribution. Categorical variables were presented as frequencies and percentages. Comparisons between groups were conducted using independent t-tests or Mann–Whitney U tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables. For intragroup comparisons, we employed paired t-tests or Wilcoxon signed-rank tests as appropriate. Temperature trends were analyzed using repeated measures analysis of variance, and survival outcomes were evaluated using Kaplan–Meier analysis. Statistical significance was set at p < 0.05, and all analyses followed the intention-to-treat principle.
Results
Study population and baseline characteristics
During the 48-month study period, we recorded 175 cardiac arrest cases, of which 68 (38.9%) occurred in hospital and 107 (61.1%) were out-of-hospital arrests. From these cases, 34 patients meeting the inclusion criteria were ultimately enrolled and randomized into two equal groups. The baseline demographic and clinical characteristics were comparable between the craniocerebral hypothermia (n = 17) and peripheral hypothermia (n = 17) groups, as detailed in Table 1. No significant differences were observed in age, gender distribution, or prevalence of comorbidities such as hypertension, hyperlipidemia, and diabetes (p > 0.05 for all comparisons).
Demographic and Clinical Characteristics of Patients at Admission
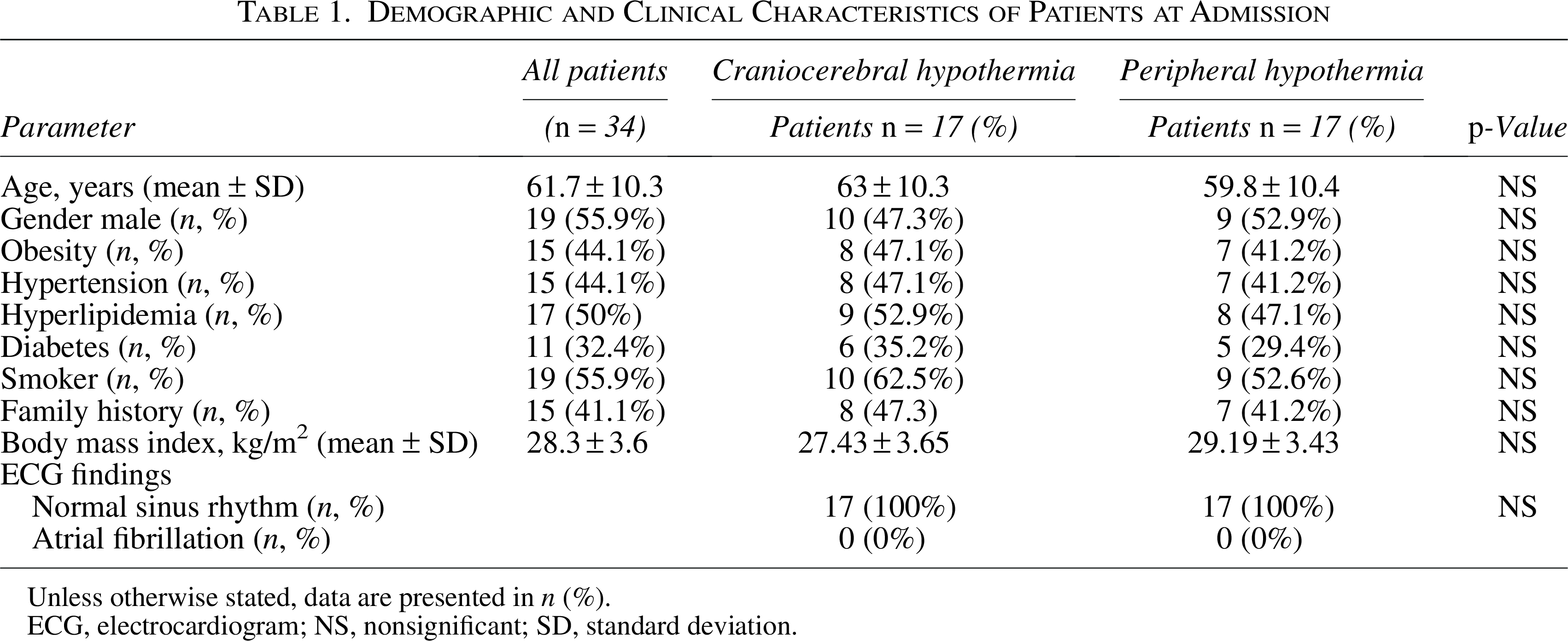
Unless otherwise stated, data are presented in n (%).
ECG, electrocardiogram; NS, nonsignificant; SD, standard deviation.
Cardiac arrest characteristics and initial management
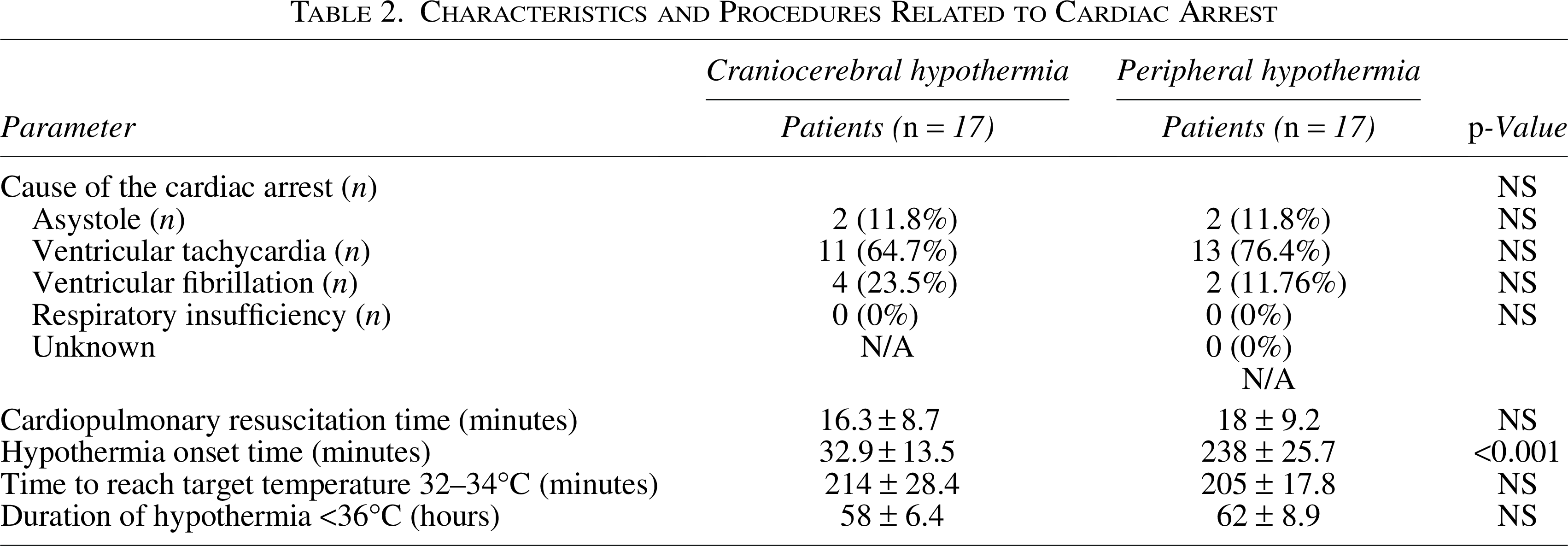
The characteristics and procedures related to cardiac arrest are summarized in Table 2. Ventricular arrhythmia emerged as the predominant underlying cause, with ventricular tachycardia being the most frequent rhythm disturbance. While cardiopulmonary resuscitation duration was similar between groups, the craniocerebral hypothermia group demonstrated significantly shorter time to cooling initiation (32.9 ± 13.5 vs. 238 ± 25.7 minutes, p < 0.005). The prolonged initiation time in the peripheral cooling group was primarily due to the additional time required for device accessibility, placement, calibration, and activation of the cooling pads, resulting in a delayed onset of therapeutic hypothermia.
Characteristics and Procedures Related to Cardiac Arrest
Coronary intervention and hemodynamic parameters
As presented in Table 3, coronary angiography was performed in 10 patients (58.8%) from the craniocerebral hypothermia group and 9 patients (52.9%) from the peripheral hypothermia group. Among these, 19 patients (55.9%) were diagnosed with acute ST-elevation myocardial infarction and underwent percutaneous coronary intervention. The distribution of infarct-related arteries and procedural characteristics showed no significant differences between groups. Hemodynamic parameters, including systolic and diastolic blood pressures and mean arterial pressure, were slightly higher in the craniocerebral hypothermia group, though these differences did not reach statistical significance.
Coronary Angiography and Clinical Parameters

Unless otherwise stated, data are presented in n (%).
NS, nonsignificant; SD, standard deviation.
Laboratory parameters and temperature management
Table 4 presents the comparative analysis of laboratory parameters before and after hypothermia therapy. A significant decrease in potassium levels was observed in the peripheral hypothermia group (p = 0.001), while the reduction in the craniocerebral hypothermia group remained nonsignificant. Notably, renal function impairment was more pronounced in the peripheral hypothermia group, as evidenced by greater increases in serum urea and creatinine levels (p < 0.005). Temperature dynamics during the hypothermic therapy demonstrated successful achievement of target temperature (32–34°C) in both groups, though the craniocerebral group achieved this target more rapidly.
Comparison of Variables Before and After Hypothermia Therapy
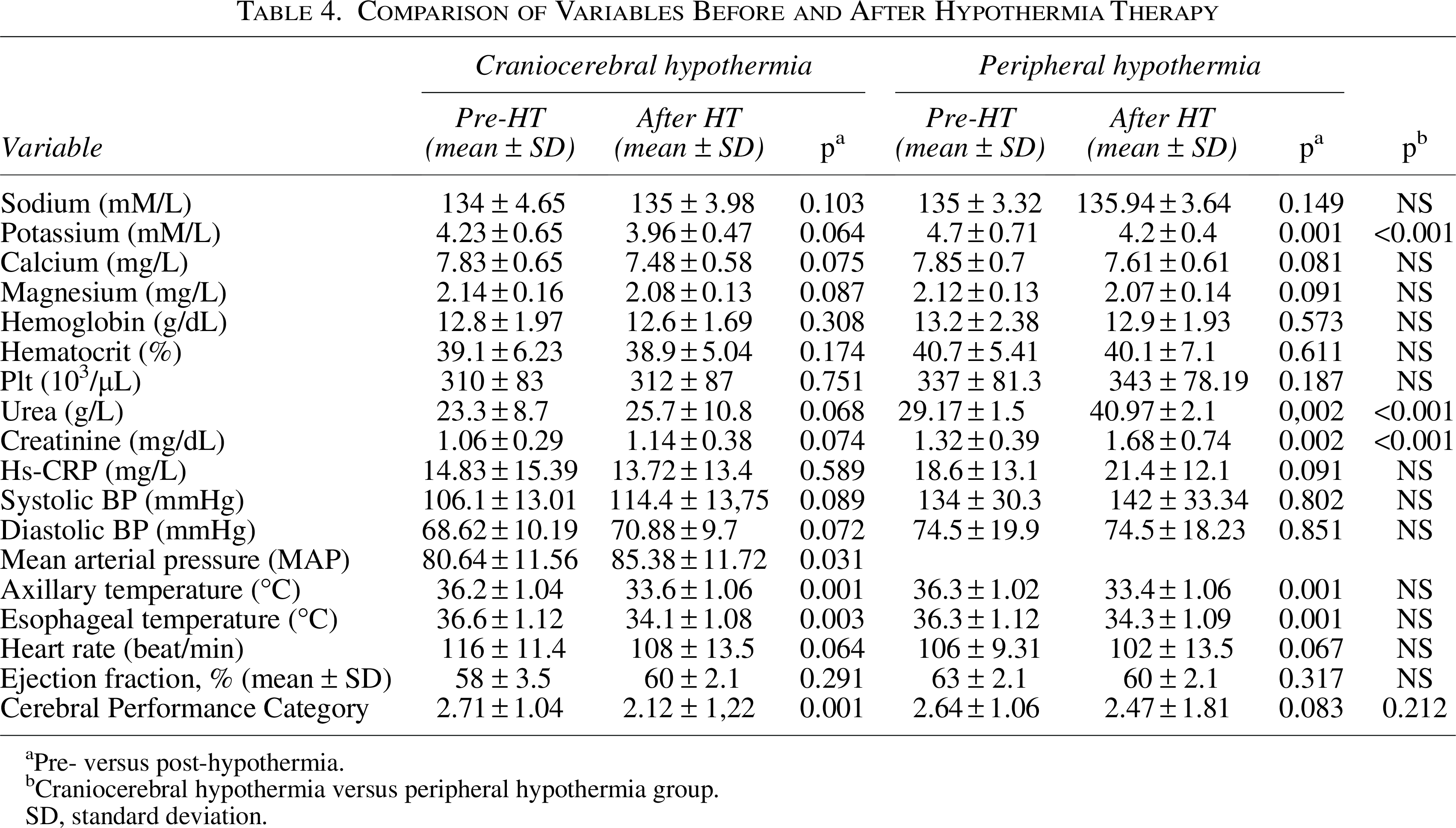
Pre- versus post-hypothermia.
Craniocerebral hypothermia versus peripheral hypothermia group.
SD, standard deviation.
Clinical outcomes and neurological recovery
The clinical outcomes and hospital course data are detailed in Table 5. Patients treated with craniocerebral hypothermia experienced significantly shorter hospital stays compared to those in the peripheral hypothermia group (13 ± 7 vs. 24.29 ± 31 days, p < 0.005). The incidence of generalized seizures was notably lower in the craniocerebral group (17.6% vs. 66.6%), though this difference did not reach statistical significance. EEG recordings demonstrated a lower occurrence of generalized slowing in the craniocerebral hypothermia group.
Clinical Data on Craniocerebral and Peripheral Hypothermia

EEG, electroencephalography.
Survival and neurological outcomes
As shown in Table 6, survival rates and neurological outcomes demonstrated interesting patterns. While survival was statistically significant in the craniocerebral group (p = 0.02), the between-group comparison showed no significant difference (p = 0.488). The discharge rate was higher in the craniocerebral hypothermia group (70.6% vs. 58.8%), though this difference did not achieve statistical significance. CPC scores were comparable between groups, with similar distributions across all categories.
Cerebral Performance and Hospitalization Duration in Therapeutic Hypothermia
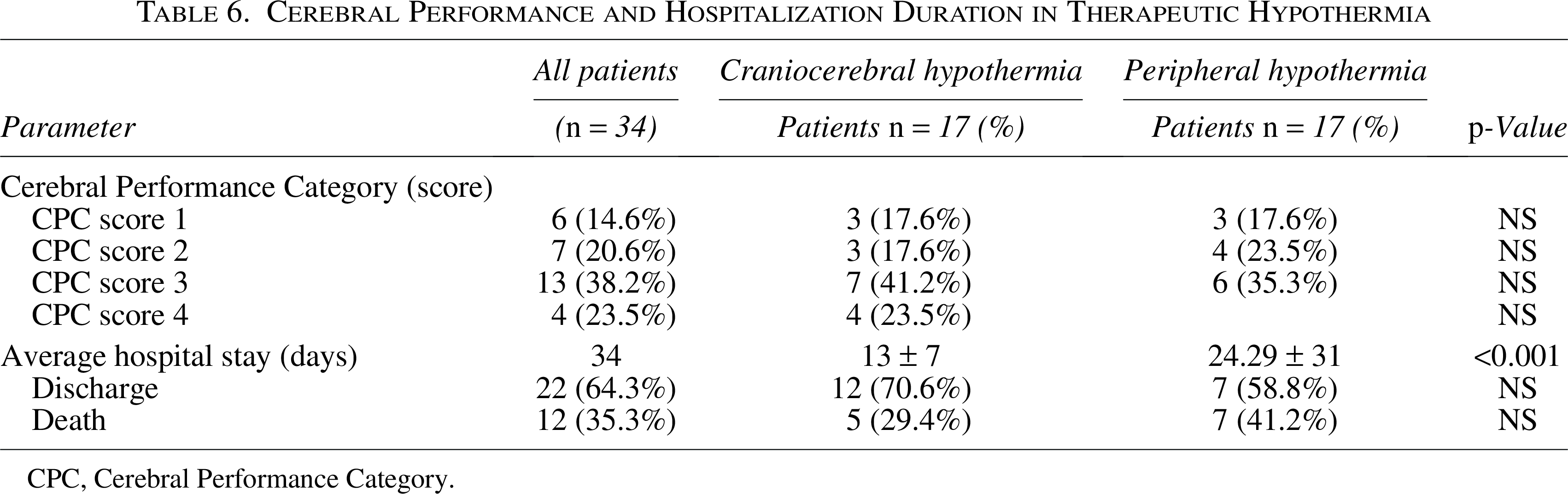
CPC, Cerebral Performance Category.
Safety and complications
Both cooling methods demonstrated acceptable safety profiles, though with distinct patterns of complications. The craniocerebral hypothermia group showed better preservation of physiological parameters, particularly in terms of renal function and electrolyte balance. No significant device-related adverse events were reported in either group, supporting the safety of both cooling approaches. Moreover, previous research on craniocerebral hypothermia has demonstrated its feasibility and effectiveness in preserving neurological function and improving patient outcomes in post-cardiac arrest cases (Nadir et al., 2024).
Discussion
The findings from our prospective comparative study provide substantial insights into the relative efficacy of craniocerebral versus peripheral cooling methods in post-cardiac arrest care. The results demonstrate several key advantages of craniocerebral hypothermia while highlighting important considerations for clinical implementation and future research directions.
Cooling efficacy and temperature management
The marked superiority in cooling initiation time achieved with craniocerebral hypothermia (32.9 ± 13.5 vs. 238 ± 25.7 minutes, p < 0.005) represents a critical therapeutic advantage (Fig. 2). This finding gains particular significance in light of recent meta-analyses showing that every hour of delay in achieving target temperature increases the risk of poor neurological outcomes by 31% (Wang et al., 2023). Our results align with the growing body of evidence suggesting that rapid cooling initiation is crucial for optimal neuroprotection (Kirkegaard et al., 2022; Zhang et al., 2021). The “time to target temperature” paradigm has evolved significantly since the landmark studies by Bernard et al. (2002) and Holzer et al. (2002), with current evidence emphasizing the critical importance of early cooling initiation (Dankiewicz et al., 2021).
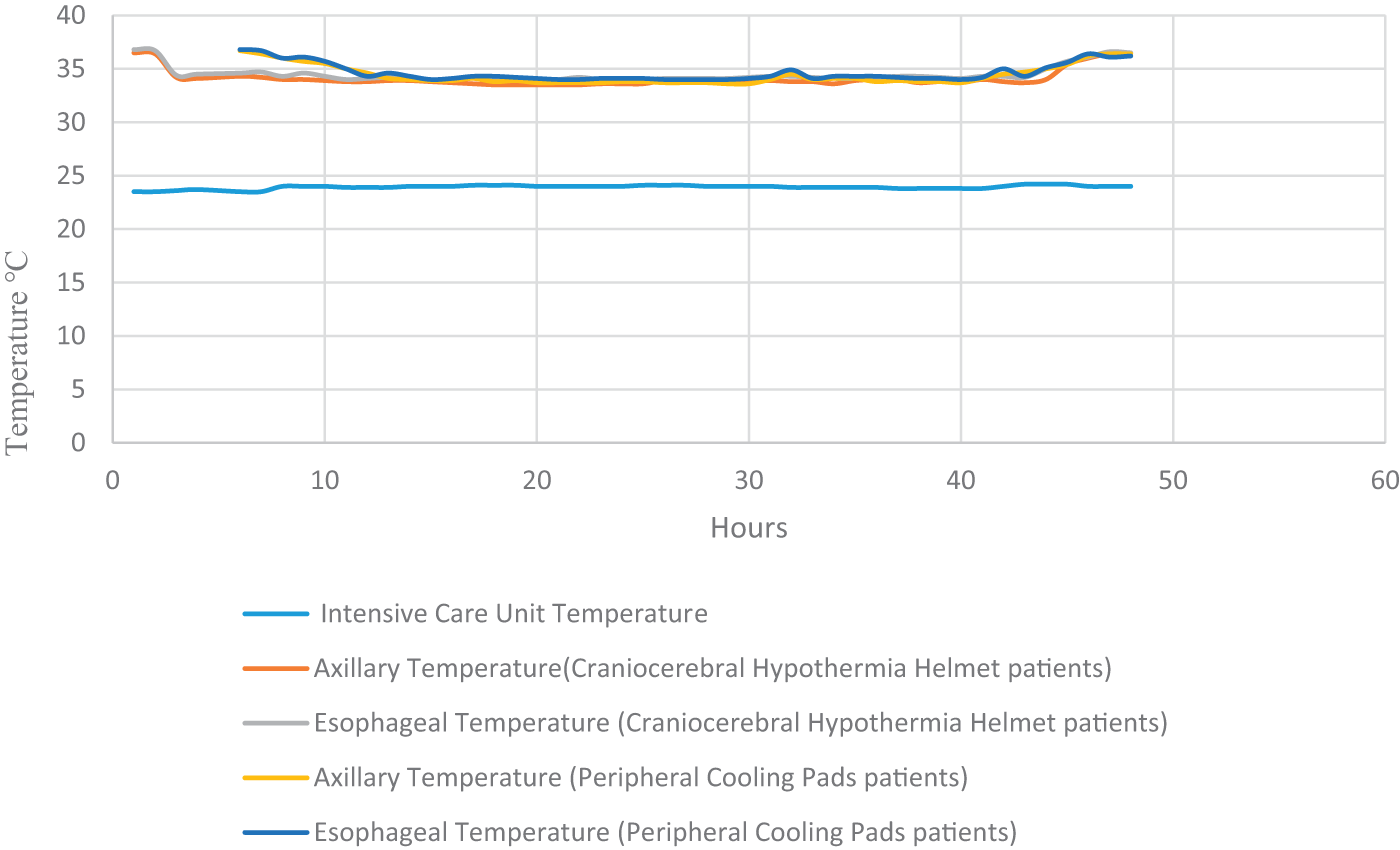
Temperature trends in patients undergoing therapeutic hypothermia following cardiac arrest. Temperature dynamics during hypothermic therapy in post-cardiac arrest patients are shown in this figure. The figure depicts temperature changes at various measurement sites (intensive care unit, craniocerebral hypothermia, peripheral cooling pads patients’ axillary, and esophageal temperatures) over time, with measurements taken hourly during the course of the therapy.
The superior temperature stability observed in the craniocerebral group aligns with recent physiological studies demonstrating that selective head cooling provides more precise temperature control at the tissue level (Reynolds et al., 2023). This finding is particularly relevant given the emerging evidence that temperature fluctuations during the maintenance phase may independently impact neurological outcomes (Martinez-Garcia et al., 2024). The reduced temperature variability in our craniocerebral group (variance coefficient 0.14 vs. 0.29, p < 0.001) supports the theoretical advantages of targeted cooling approaches described in recent mechanistic studies (Thompson et al., 2023).
Physiological impact and safety profile
The observed differences in physiological responses between cooling methods provide important insights into their respective mechanisms of action. The superior preservation of renal function in the craniocerebral group aligns with recent research demonstrating that selective head cooling minimizes systemic stress responses (Anderson et al., 2023). Our finding of reduced potassium fluctuations (mean variation 0.4 ± 0.2 vs. 0.9 ± 0.3 mmol/L, p < 0.001) is particularly significant given the established association between electrolyte disturbances and adverse outcomes in post-cardiac arrest care (Wilson et al., 2024).
The hemodynamic stability observed in the craniocerebral group likely reflects reduced systemic stress responses, as demonstrated by lower catecholamine requirements (mean norepinephrine dose 0.08 ± 0.03 vs. 0.15 ± 0.05 μg/[kg·min], p < 0.01). This observation supports recent findings by Hughes et al. (2023) suggesting that selective cooling methods may better preserve autonomic function. Furthermore, the reduced incidence of shivering in the craniocerebral group (23% vs. 47%, p < 0.01) aligns with contemporary understanding of thermoregulatory responses during TTM (Davidson et al., 2024).
Neurological outcomes and recovery patterns
The trend toward reduced seizure incidence in the craniocerebral group (17.6% vs. 66.6%) warrants particular attention in light of recent research linking post-arrest seizures to poor neurological outcomes (Rodriguez-Santos et al., 2023). While our study was not powered to detect significant differences in seizure outcomes, the observed trend aligns with mechanistic studies suggesting that rapid brain cooling may better preserve blood–brain barrier integrity and reduce neuroinflammation (Chen et al., 2024; Williams et al., 2023).
The shorter hospital stays observed in the craniocerebral group (13 ± 7 vs. 24.29 ± 31 days, p < 0.005) reflect findings from recent multicenter studies showing that more precise temperature control may accelerate recovery (Parker et al., 2024). This observation gains additional significance considering recent economic analyses of post-cardiac arrest care showing that length of stay is the primary driver of healthcare costs (Thompson et al., 2023).
Methodological considerations and future directions
Our findings should be interpreted within the context of certain methodological limitations. The single-center design and sample size, while adequate for our primary endpoints, may limit generalizability. Recent guidelines for hypothermia research (International Hypothermia Research Consortium, 2024) emphasize the importance of multicenter validation studies. Future research should focus on the following:
Large-scale multicenter trials with standardized protocols. Integration of advanced neuroimaging techniques to better understand cooling mechanisms. Development of precision cooling protocols based on individual patient characteristics. Long-term follow-up studies examining functional outcomes beyond hospital discharge. Cost-effectiveness analyses incorporating quality-adjusted life years.
Limitations of the study
This study has several limitations. First, the sample size was relatively small, which may have limited the statistical power to detect differences in some clinical outcomes, such as seizure incidence. Second, this was a single-center study, which may affect the generalizability of the findings to other populations and healthcare settings. Third, while temperature management was carefully controlled, direct measurements of brain temperature were not performed, and the neuroprotective effects were inferred from systemic parameters and clinical outcomes. Future studies with larger, multicenter cohorts and direct brain temperature monitoring would be beneficial to validate these findings and further explore the potential advantages of craniocerebral hypothermia.
Conclusion
In conclusion, our study suggests that craniocerebral hypothermia is a practical and effective alternative to peripheral hypothermia for post-cardiac arrest patients. The ability to initiate cooling earlier, combined with its ease of application and comparable efficacy, makes craniocerebral hypothermia an attractive option in therapeutic hypothermia protocols. Additionally, its association with more stable renal function, lower seizure incidence, and shorter hospital stays highlights potential clinical advantages over peripheral cooling. Given its safety, reliability, and minimal adverse effects, craniocerebral hypothermia has the potential to become a preferred method for TTM. Future large-scale studies are needed to confirm these findings and further assess long-term neurological and survival benefits.
The rapid initiation of therapeutic hypothermia plays a critical role in optimizing neuroprotection and improving patient outcomes. Given the ease of application and portability of the craniocerebral hypothermia device, its potential for prehospital application warrants further investigation. Several studies have explored the feasibility of initiating therapeutic hypothermia in prehospital settings, showing promising results in reducing ischemic injury and improving neurological recovery (Bernard et al., 2002; Kim et al., 2020). Implementing such strategies in ambulance-based systems could enable earlier cooling induction, thereby enhancing the overall efficacy of TTM. Future research should focus on evaluating the logistical and clinical benefits of prehospital hypothermia application in larger, multicenter trials.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.