
Abstract
Primary dysmenorrhea is a prevalent condition causing severe menstrual pain in nulliparous women, negatively impacting daily functioning and well-being. This randomized controlled trial investigated the efficacy of cryotherapy in alleviating pain and enhancing secondary outcomes such as sleep quality, quality of life, and physical activity. Fifty-eight nulliparous women were randomly assigned to a cryotherapy group or a control group. Pain intensity was measured using the Numeric Rating Scale, whereas secondary outcomes were evaluated with the Pittsburgh Sleep Quality Index, World Health Organization Quality of Life-Brief Version, and the International Physical Activity Questionnaire. Socioeconomic factors, including household income, education, and occupation, were also assessed. Cryotherapy significantly reduced pain intensity from a baseline of 7.1 ± 1.4 to 1.8 ± 1.7 (p < 0.001) compared with a modest reduction in the control group (5.9 ± 1.9–5.4 ± 2.1). Sleep quality improved more in the cryotherapy group (6.90 ± 3.0 to 5.03 ± 2.5) than in the control group (6.88 ± 3.6 to 5.68 ± 2.8). However, no statistically significant changes were observed in the quality of life or physical activity levels, likely because menstrual pain alone may not sufficiently influence these domains, which are affected by broader psychosocial and behavioral factors. These findings demonstrate that cryotherapy is a simple, cost-effective intervention for managing primary dysmenorrhea, providing substantial pain relief and modest improvements in sleep quality. Further research is recommended to evaluate its long-term benefits and potential for broader applications in menstrual health management.
Introduction
Primary dysmenorrhea, a prevalent gynecological condition, manifests as menstrual pain in the absence of identifiable pelvic abnormalities. It accounts for the majority of menstrual pain cases in ovulating women, with a prevalence estimated between 45% and 95% among reproductive-aged females (Correyero-León et al., 2024; Piontek et al., 2024). The pain is typically characterized by acute, spasmodic cramps that emerge 1–2 years postmenarche, coinciding with the establishment of ovulatory cycles. It generally begins 1–2 days prior to menstruation, peaks in intensity within the first 24–36 hours of bleeding, and may persist for up to 3 days (Amza et al., 2024; Fuentes-Aparicio et al., 2023). This pain, localized in the suprapubic region and often radiating to the thighs or back (Correyero-León et al., 2024), is frequently accompanied by physical and psychological symptoms that exacerbate the overall burden (Ferries-Rowe et al., 2020; Fuentes-Aparicio et al., 2023; Iacovides et al., 2015; Karout et al., 2021).
While the pathophysiology of primary dysmenorrhea is not fully understood, it is believed to involve a complex interplay of hormonal, vascular, and inflammatory factors. These mechanisms contribute to vasoconstriction, uterine hypercontractility, hypoxia, and increased pain perception (Amza et al., 2024; Karout et al., 2021). Additionally, dysregulated inflammatory responses may further exacerbate symptoms, with heightened levels of proinflammatory mediators observed in affected women (Szmidt et al., 2020). In addition to pain, these physiological alterations have been associated with sleep disturbances in women with dysmenorrhea, including reduced sleep quality and increased risk of insomnia (Iacovides et al., 2015).
Management strategies for primary dysmenorrhea encompass hormonal, nonhormonal, and nonpharmacological interventions. Hormonal treatments, particularly oral contraceptives, regulate menstrual cycles and alleviate pain. Nonsteroidal anti-inflammatory drugs are the first-line nonhormonal therapy due to their established analgesic effects (Amza et al., 2024; Kirsch et al., 2024). Nonpharmacological approaches include transcutaneous electrical nerve stimulation, physical exercise, dietary supplements, manual therapy, and thermotherapy, which offer varying degrees of symptom relief (Deodato et al., 2023; González-Mena et al., 2024; Kirsch et al., 2024). Heat thermotherapy, through its vasodilatory effect, is widely used to mitigate menstrual pain by improving uterine blood flow and alleviating hypoxia (Amza et al., 2024; Li et al., 2024).
Cryotherapy, which involves the application of cold to reduce tissue temperature, has emerged as a potential alternative for pain management. It acts by lowering nerve conduction velocity, reducing blood flow, and promoting muscle relaxation, thereby alleviating pain, inflammation, and edema (Garcia et al., 2021; Guillot et al., 2017). The analgesic effects of cryotherapy are attributed to its influence on neuromuscular electrophysiology, particularly the inhibition of sodium channel closure, which diminishes nociceptor discharge frequency and raises the pain threshold (Garcia et al., 2021; Zhang et al., 2018). Moreover, cryotherapy modulates the inflammatory response by decreasing proinflammatory and increasing anti-inflammatory mediators, as supported by evidence from clinical studies (Kunkle et al., 2021). The temperature range typically used in cryotherapy for pain management falls between −5°C and −20°C, depending on the duration of exposure and the specific intervention. Temperatures in this range effectively reduce nerve conduction velocity and promote local vasoconstriction, which helps to control inflammation and reduce pain. Unlike heat therapy, which primarily improves circulation and muscle relaxation, cryotherapy provides pain relief by altering nerve conduction and inflammatory processes, potentially offering an alternative mechanism of action that may be more effective for certain individuals. Additionally, while physical exercise has shown benefits for dysmenorrhea, adherence to regular activity can be challenging, particularly during episodes of severe pain. Cryotherapy, as a passive intervention, may be a more accessible and immediate pain relief option.
Given the pathophysiology of primary dysmenorrhea—characterized by inflammation and pain mediated by uterine hypercontractility—cryotherapy presents a promising noninvasive treatment. Its physiological effects suggest potential benefits for reducing pain intensity and improving overall well-being. This study hypothesizes that cryotherapy alleviates menstrual pain primarily by reducing nerve conduction velocity and modulating inflammatory pathways, leading to decreased pain perception and improved comfort. However, limited research has focused specifically on cryotherapy’s efficacy in nulliparous women, a demographic often disproportionately affected by dysmenorrhea.
Therefore, the objectives of this randomized controlled trial are to evaluate the effectiveness of cryotherapy in nulliparous women with primary dysmenorrhea and to examine the influence of socioeconomic status on treatment outcomes. This study seeks to advance the understanding of cryotherapy as a noninvasive intervention for menstrual pain and its broader implications.
Materials and Methods
Design
This study is a randomized clinical trial conducted to assess the effects of cryotherapy in nulliparous women with primary dysmenorrhea. The protocol for this clinical trial was approved by the Ethics Committee of the University of Malaga, Spain (reference number 87/2024-H), and was prospectively registered in an international public registry ClinicalTrials (registration reference NCT06667440). The study has been carried out in accordance with The Code of Ethics of the World Medical Association, and every participant was given a brief explanation of the study procedure prior to providing written consent.
Participants
Recruitment took place between the months of June and August 2024 through social media and official communication channels of the Universities of Malaga and Valencia. Potential participants completed an online form, including their demographic information. Forms were screened by two members of the research team, checking for eligibility criteria.
Participants were included if they (1) were menstrually active, (2) had normal menstrual cycles that varied between 24 and 38 days (Campbell et al., 2021), (3) had menstrual periods between 3 and 7 days, and (4) suffered pain lasting from 1 to 3 days. Participants were excluded if they (1) were diagnosed with a disease that could generate secondary dysmenorrhea, (2) had systemic or psychiatric diseases, and (3) had a history of use of hormonal medication, birth control pills, or intrauterine devices.
Interventions
Participants were randomized in a 1:1 ratio to either the intervention group, which received home-based cryotherapy, or the control group, which received no intervention, using a sealed opaque envelope system. An independent researcher, not involved in participant recruitment or assessment, conducted the randomization to ensure allocation concealment. Researchers responsible for outcome assessments and statistical analyses were blinded to group allocation. Although participants were not blinded due to the inherent nature of the intervention, efforts were made to minimize bias during the assessment process.
Participants were instructed to apply a cold pack for 15 minutes, twice daily, during the first 3 days of their menstrual period. Follow-up was conducted over three consecutive menstrual cycles. Specific criteria were established for the cold pack used, as well as a detailed application protocol. The cold pack used in this study met specific criteria: it measured between 11 and 15 cm in width and between 25 and 30 cm in length. It consisted of a nontoxic gel to ensure safe use. Participants were instructed to position themselves comfortably, preferably lying on their backs with knees bent. They were directed to place the cold pack horizontally over the hypogastric region—between the navel and pubic area—and to maintain this position for 15 minutes. To ensure safety, participants were also instructed to use a protective barrier, such as a cloth, between the cold pack and the skin to prevent direct contact and avoid the risk of frostbite or cold burns. This procedure was repeated twice daily, ideally at consistent times, over the first 3 days of the menstrual cycle. Adherence to the intervention was monitored through continuous contact with the participants via email and instant messaging, where researchers provided support and reminders to ensure consistent application.
Outcomes
Participants were assessed prior to the intervention by two blinded members of the research team. Outcome measures were collected every month during the first 3 days of the participants’ menstrual cycle, over a total of three menstrual cycles. Participants were instructed to complete an online form to record their outcomes during these 3 days. To ensure completeness, the research team maintained regular follow-up with participants, reaching out in cases where data were missing or if participants encountered difficulties with the outcome reporting process.
Main outcome
Pain intensity was assessed using the Numerical Rating Scale (NRS), which asks participants to rate their pain on an 11-point scale, with 0 indicating “no pain” and 10 representing the “worst pain imaginable.” Higher scores correspond to greater pain intensity (Euasobhon et al., 2022).
Secondary outcomes
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a standardized self-administered instrument designed to evaluate various aspects of sleep over a 1-month period. The PSQI comprises 19 items, which are grouped into 7 subscales: (1) Subjective Sleep Quality, (2) Sleep Latency, (3) Sleep Duration, (4) Habitual Sleep Efficiency, (5) Sleep Disturbances, (6) Use of Sleep Medication, and (7) Daytime Dysfunction. Each subscale is scored from 0 to 3, with higher scores indicating greater severity of the respective issue. The total PSQI score, ranging from 0 to 21, is calculated by adding the subscale scores, with higher total scores reflecting poorer overall sleep quality (Otero et al., 2022).
Quality of life was assessed using the World Health Organization Quality of Life-Brief Version (WHOQOL-Bref), a widely used tool to evaluate overall well-being across four domains: physical health, psychological health, social relationships, and environment. The WHOQOL-Bref consists of 26 items, with each item rated on a 5-point Likert scale. The domain scores are calculated from the responses, with higher scores reflecting better quality of life in each domain. Additionally, the WHOQOL-Bref includes a global quality of life item, which provides a summary measure of participant perceived overall well-being (Rondung et al., 2023).
Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ), a widely used self-reported measure designed to evaluate physical activity levels over the past 7 days. The IPAQ includes three subscales: (1) Vigorous Physical Activity, (2) Moderate Physical Activity, and (3) Walking. Responses are used to calculate the total physical activity score, expressed in metabolic equivalent of task (MET)-minutes per week. Higher total scores indicate greater physical activity levels, with results typically categorized into three levels: low, moderate, and high physical activity (Sanda et al., 2017).
Statistical analysis
Statistical analyses were performed using SPSS software (version 28.0 for macOS; SPSS Inc., Chicago, IL). Descriptive statistics were reported as means with standard deviations (SDs) for continuous variables and as frequencies for categorical variables. The normality of the data distribution was assessed using the Kolmogorov–Smirnov test, and the homogeneity of variances was tested using Levene’s test, and no significant differences were found. Given the absence of prior studies in this specific context, the sample size calculation was based on an anticipated effect size of 0.8. To detect between-group differences with 80% statistical power and a two-sided significance level of 0.05, we estimated that a minimum of 50 participants (25 per group) would be required. To account for potential dropouts and losses to follow-up, we aimed to recruit a larger sample.
Pain intensity, sleep quality, and quality of life will be analyzed using a mixed-model two-way analysis of variance (ANOVA) to evaluate between-group factors (cryotherapy vs. control) and within-group factors (changes over time) if data meet normal distribution. If normality is not met, nonparametric methods will be employed. Between-group differences will be assessed using the Mann–Whitney U test, and within-group changes over time will be analyzed with the Wilcoxon signed-rank test.
Socioeconomic status was evaluated using the Kuppuswamy Socioeconomic Status Scale (Sharma, 2017), which classifies individuals into socioeconomic categories based on three dimensions: education, occupation, and household monthly income. Educational levels were categorized into four tiers: (1) professional training, (2) undergraduate level, (3) graduate level, and (4) postgraduate level. Occupations were classified according to the level of training required: (1) unemployed, (2) student, (3) jobs requiring technical training, (4) jobs requiring professional training, and (5) jobs requiring graduate or postgraduate education. Household monthly income was stratified into five categories: (1) <500 euros, (2) 500–1000 euros, (3) 1000–1500 euros, (4) 1500–2000 euros, and (5) >2000 euros. Associations with continuous variables were examined using Pearson’s correlation coefficient, whereas Spearman’s rank correlation coefficient was employed for associations involving categorical variables.
Results
Participants
Initially, 183 responses were collected from women with dysmenorrhea through a preliminary survey. After applying the study’s inclusion and exclusion criteria, 107 respondents were excluded, leaving 76 eligible participants. Of these, 59 consented to participate and were randomized into 2 groups: 29 in the intervention group and 30 in the control group. During the intervention period, five participants in the control group were lost to follow-up. This resulted in a final sample of 54 participants, comprising 29 in the intervention group and 25 in the control group. Participant flow throughout the study is shown in Figure 1.
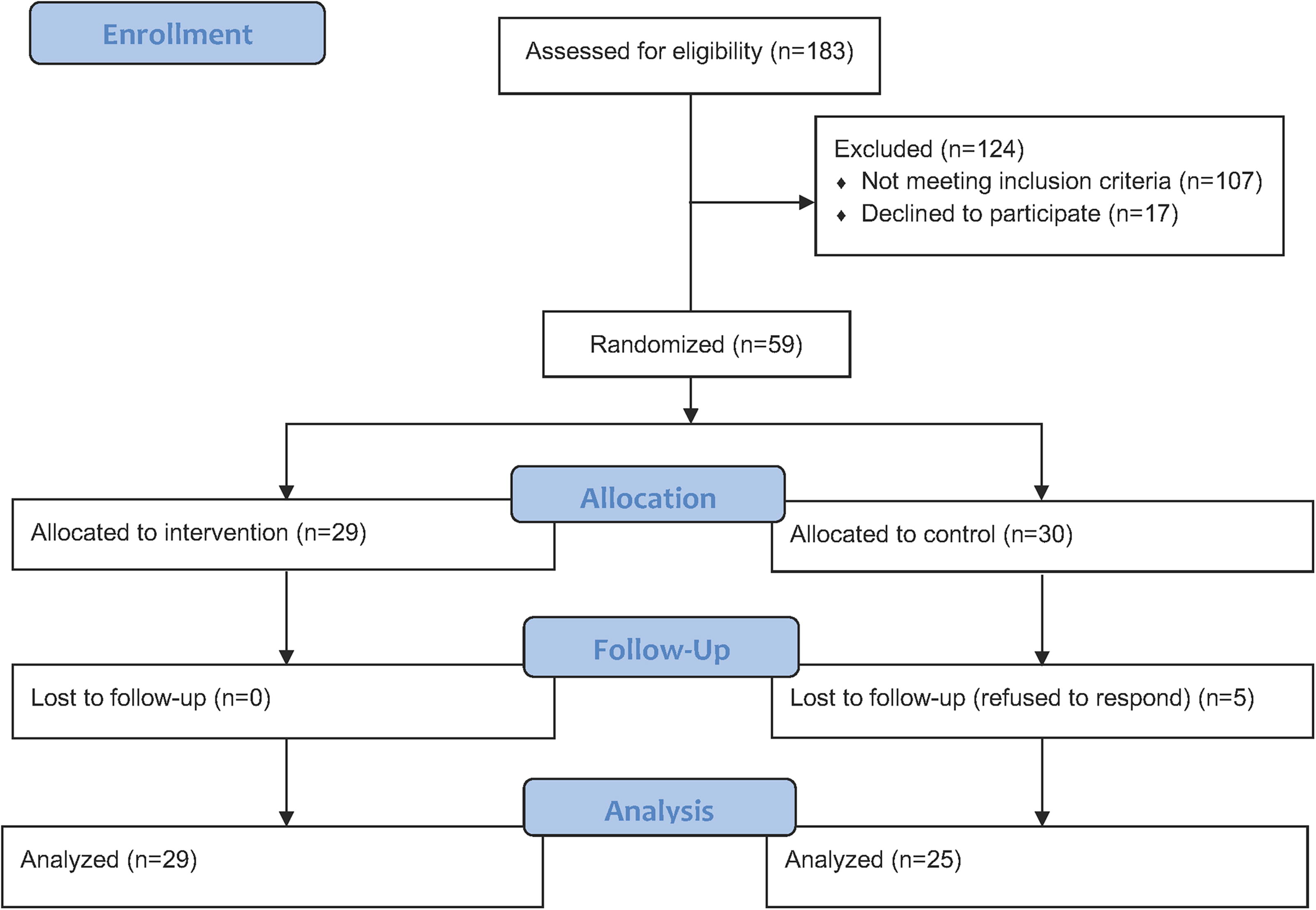
Participant flow diagram.
Baseline demographic characteristics of the participants are presented in Table 1. The mean age of the sample was 24.5 years (SD = 3.2), with no significant differences between the cryotherapy group (24.5 ± 3.6 years) and the control group (24.4 ± 2.8 years). No participants in the cryotherapy group reported other health conditions, whereas two participants (6.7%) in the control group reported health conditions; however, these were unrelated to primary dysmenorrhea. Regarding medication use, six participants (20.7%) in the cryotherapy group and seven participants (23.3%) in the control group reported prior use, resulting in an overall prevalence of 22%. All participants discontinued these medications at least 1 year before the study. In the cryotherapy group, five participants had previously used oral contraceptives, and one had an intrauterine device. In the control group, six participants had used oral contraceptives, and one did not specify the type of medication.
Baseline Demographic Characteristics of the Participants
SD, standard deviation.
Socioeconomic and educational characteristics of the participants are detailed in Table 2. The study population was predominantly highly educated, with 39% having completed postgraduate studies and 50.8% holding undergraduate degrees. In terms of occupation, the majority of participants held jobs requiring graduate or postgraduate qualifications (57.6%), with 51.7% in the cryotherapy group and 63.3% in the control group. Students made up 22% of the sample, evenly distributed between groups, whereas a small proportion of participants were unemployed (3.4%, all in the control group). Household monthly income levels ranged widely, with 30.5% reporting <500 euros per month, primarily students. The most common income range was 1500–2000 euros (32.2%), followed by 1000–1499 euros (27.1%). A small fraction (1.7%) reported incomes exceeding 2000 euros, exclusively in the cryotherapy group.
Participant Socioeconomic Status
EUR, euros.
Main analysis
Results of the ANOVA analysis are presented in Table 3. Cryotherapy significantly improved pain intensity with a marked reduction from pre- to postintervention, whereas the control group showed minimal change. Sleep quality improved modestly in both groups, with a greater reduction in scores observed in the cryotherapy group, although the group-by-time interaction was not significant. Quality of life showed minimal changes, with stable scores in the cryotherapy group and a slight decrease in the control group, neither of which was significant. Physical activity levels exhibited slight variability, with an increase in the cryotherapy group and a decrease in the control group, but these changes were not statistically significant.
Results of the Mixed-Design Two-Way Repeated Measures ANOVA
IPAQ, International Physical Activity Questionnaire; MET, metabolic equivalent of task; NRS, Numerical Rating Scale; PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation; WHOQOL-Bref, World Health Organization Quality of Life-Brief Version.
Pain intensity
Pain intensity showed significant improvements in the cryotherapy group compared with the control group. Preintervention NRS scores were similar between groups (cryotherapy: 7.1 ± 1.4; control: 5.9 ± 1.9). Postintervention scores revealed a marked reduction in pain for the cryotherapy group (1.8 ± 1.7) compared with minimal change in the control group (5.4 ± 2.1). These results are illustrated in Figure 2.
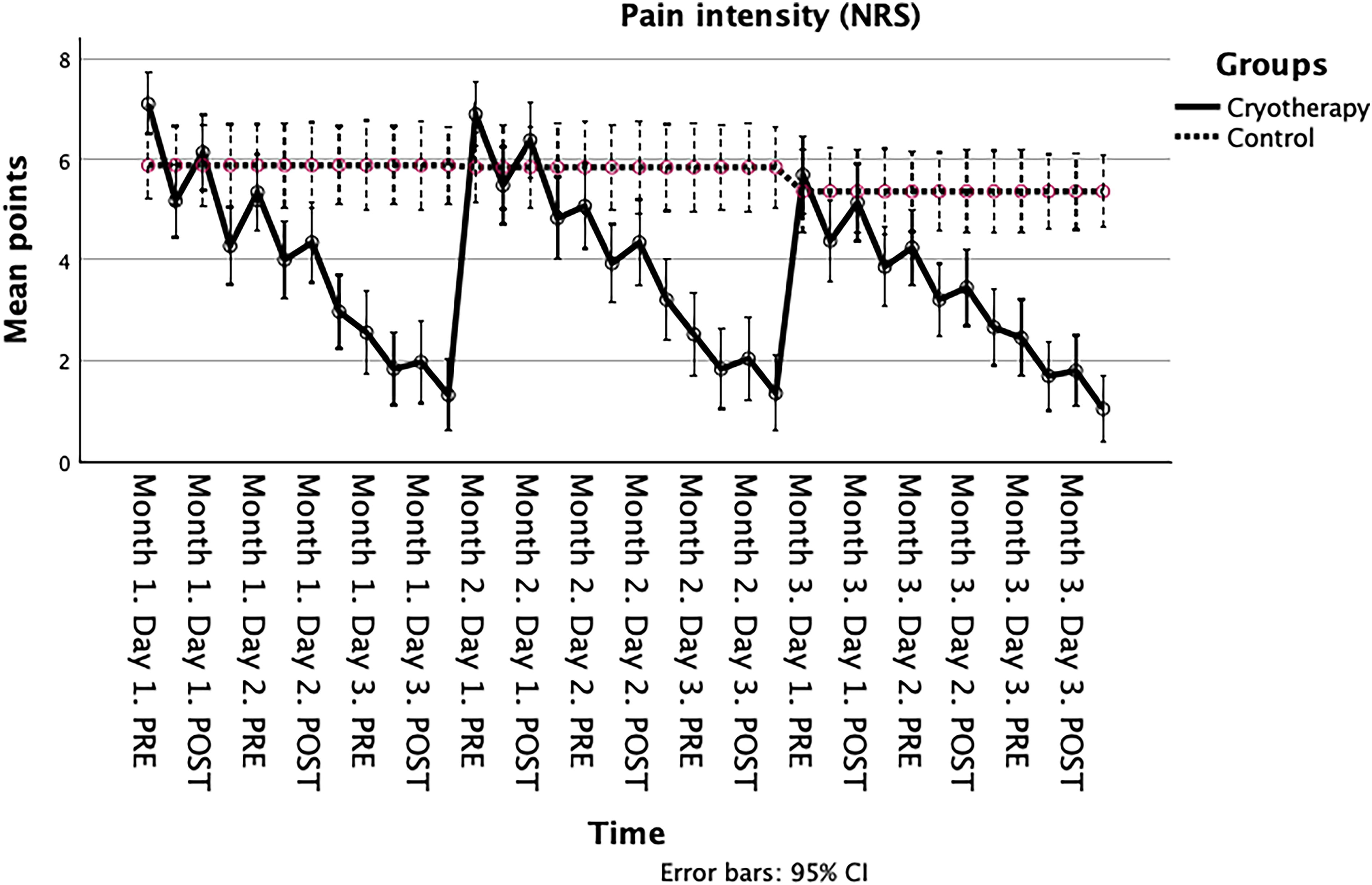
Changes over time for pain intensity.
Sleep quality
Sleep quality showed a modest improvement in the cryotherapy group compared with the control group. Baseline PSQI scores were similar between groups (cryotherapy: 6.90 ± 3.0; control: 6.88 ± 3.6). Postintervention scores indicated a greater reduction in PSQI scores for the cryotherapy group (5.03 ± 2.5) compared with the control group (5.68 ± 2.8). These findings are illustrated in Figure 3.
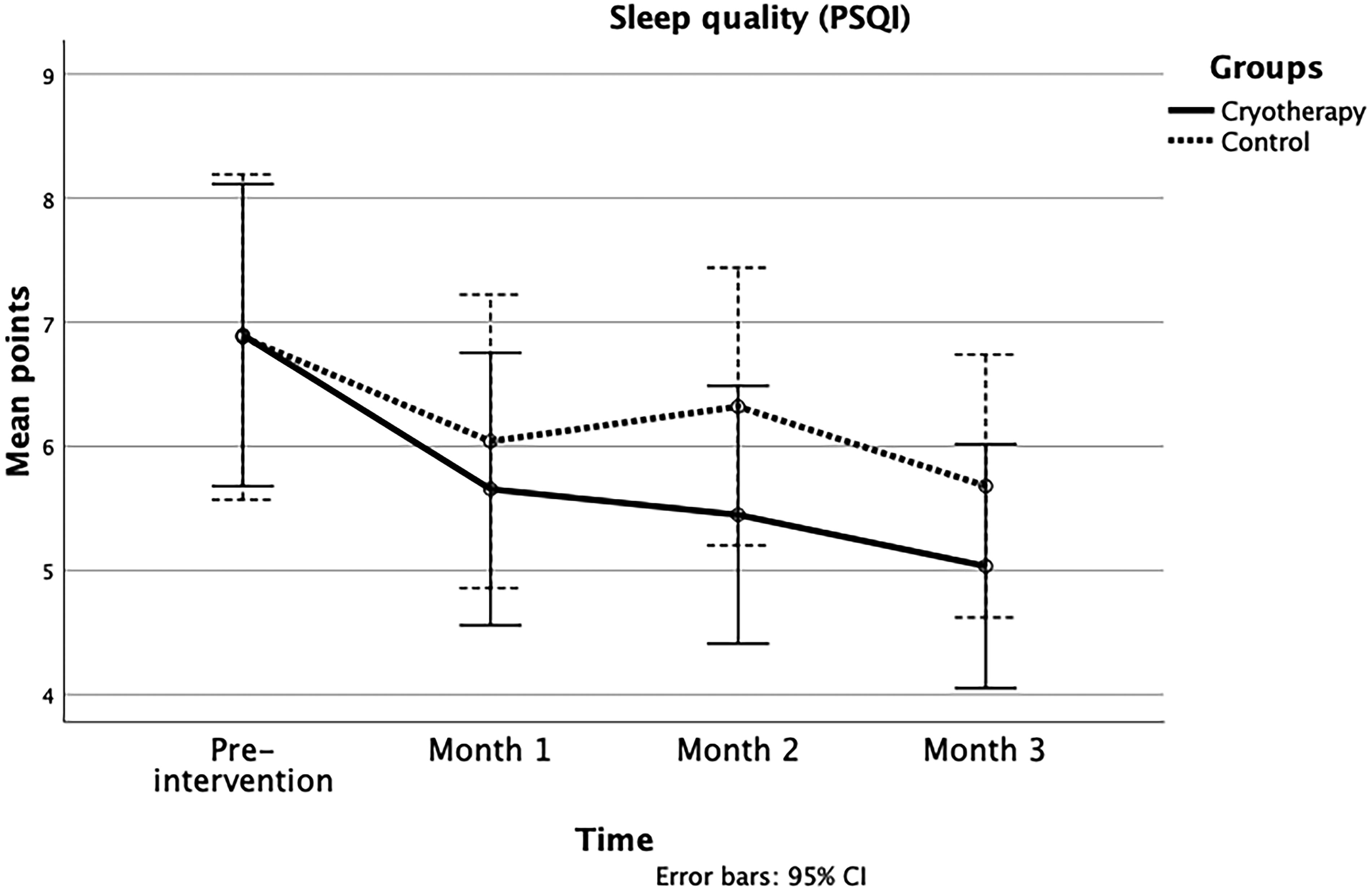
Changes over time for sleep quality.
Quality of life
Quality of life showed minimal changes in both the cryotherapy and control groups over time. Baseline scores were slightly higher in the cryotherapy group (75.8 ± 10.8) compared with the control group (71.6 ± 16.4). Postintervention scores remained stable for the cryotherapy group (75.6 ± 11.1) but decreased slightly for the control group (69.7 ± 16.6). These findings are illustrated in Figure 4.
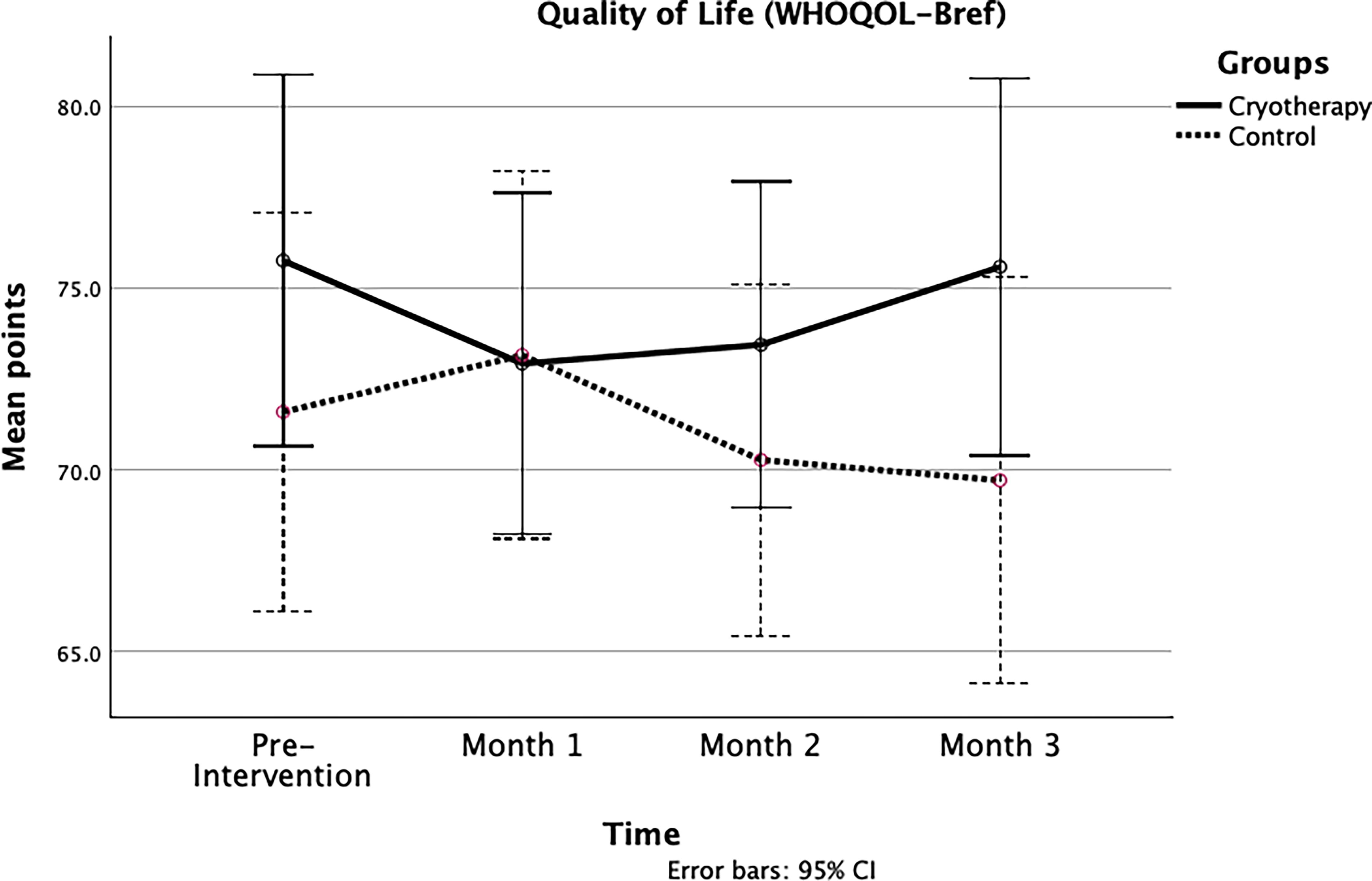
Changes over time for quality of life.
Physical activity levels
Physical activity levels showed variable changes in both the cryotherapy and control groups over time. Baseline IPAQ scores were lower in the cryotherapy group (3360.6 ± 2486 METs) compared with the control group (5301.4 ± 7792.3 METs). Postintervention scores increased slightly in the cryotherapy group (3652.7 ± 4818.5 METs) but decreased in the control group (3605.2 ± 3850.9 METs). These results are illustrated in Figure 5.
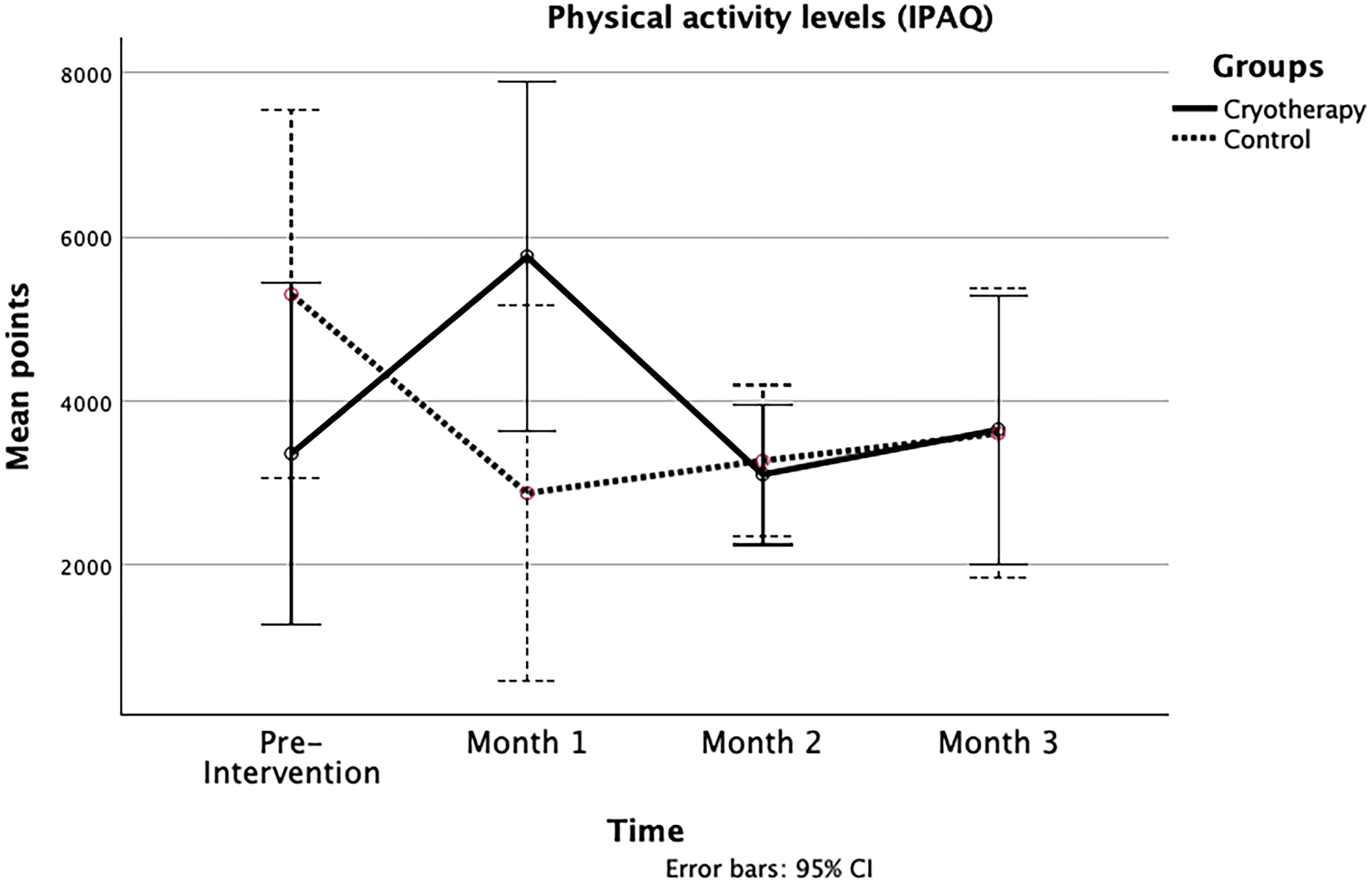
Changes over time for physical activity levels.
Correlation analysis
The results of the correlation analyses are summarized in Table 4. In general, age, educational level, and occupation did not show significant correlations with the intervention outcomes in either the cryotherapy or control groups. However, a significant positive correlation was observed between household monthly income and NRS scores in the cryotherapy group (p < 0.001), suggesting that higher income was associated with greater pain reduction. No significant correlations were found between household income and the other outcomes in either group.
Results of the Correlation Analysis Between Results and Participant’s Age and Socioeconomic Status
IPAQ, International Physical Activity Questionnaire; NRS, Numerical Rating Scale; PSQI, Pittsburgh Sleep Quality Index; WHOQOL-Bref, World Health Organization Quality of Life-Brief Version.
Discussion
This study aimed to evaluate the effectiveness of cryotherapy in reducing pain intensity and its impact on sleep quality, quality of life, and physical activity levels in nulliparous women with primary dysmenorrhea. A secondary objective was to explore the relationship between treatment outcomes and participants’ socioeconomic status, including household income, education, and occupation. To our knowledge, this is the first study to examine cryotherapy specifically in this population. Our results showed that cryotherapy led to significant reductions in pain intensity, whereas its effects on sleep quality, quality of life, and physical activity were more modest and did not reach statistical significance.
Menstrual pain in primary dysmenorrhea follows a cyclical pattern, with peaks at the onset of menstruation that subside as the cycle progresses. Our findings suggest that repeated cryotherapy modulates this pattern, progressively reducing pain intensity at these peaks. This trend was absent in the control group, highlighting cryotherapy’s potential efficacy. Silva et al. (2022) similarly reported reduced pain intensity and quality-of-life improvements after daily 20-minute cryotherapy sessions over one cycle, despite a smaller sample size. Although research on cryotherapy for dysmenorrhea is limited, its effectiveness has been demonstrated in other pain-related conditions. For instance, cryotherapy has been used for postpartum perineal pain management, where its application significantly reduced pain intensity following vaginal delivery (Morais et al., 2016). Additionally, its anti-inflammatory effects have been observed in chronic pain conditions, where cryotherapy downregulated proinflammatory pathways such as interleukin (IL)-6/IL-17, potentially contributing to pain relief (Guillot et al., 2017). These mechanisms may help explain the analgesic effects observed in our study, suggesting that cryotherapy’s impact on dysmenorrhea could be mediated by similar physiological responses. Adherence to the protocol, particularly limiting sessions to 20 minutes, is critical to balancing efficacy and avoiding adverse effects such as increased ischemia and hypoxia (Morais et al., 2016).
Sleep quality showed improvements in both groups over the follow-up period, indicating that it is not exclusively tied to pain intensity but is influenced by multifactorial elements. Previous studies have identified a range of factors affecting sleep quality, including anxiety, depression, and excessive technology use (Nikolic et al., 2023). Other contributors, such as dietary habits, alcohol, tobacco, or caffeine consumption, and environmental conditions, such as low indoor temperatures, have also been highlighted (Zhou et al., 2022). Additionally, occupational stressors, such as workload and job demand, play a critical role in sleep disturbances (Güngördü et al., 2023). These findings emphasize the complexity of sleep quality as a variable, requiring a holistic approach for its evaluation and management.
The correlational analysis also revealed a positive association between age and physical activity levels. However, this did not translate into a significant change in overall physical activity, likely due to the young age of the participants. Additionally, a positive correlation was found between improvements in sleep quality and reductions in pain intensity. This suggests that pain reduction may facilitate more restorative sleep, potentially by alleviating nighttime discomfort or reducing anxiety related to pain anticipation. The analysis also revealed a positive association between monthly income and improvements in pain intensity. Consistent with findings by Thurston et al. (2023), participants with higher incomes reported greater reductions in pain, potentially linked to lower stress levels and reduced financial concerns. Additional factors, such as better access to complementary health resources, greater job stability, and the psychosocial impact of perceived social status, may also contribute to this relationship. These psychosocial factors can mediate the connection between socioeconomic status and health outcomes, potentially triggering physiological responses that influence mental and physical health risks over time (Zimmer et al., 2022). This underscores the importance of considering socioeconomic disparities in the evaluation and implementation of therapeutic interventions, as they may affect treatment efficacy and overall health outcomes.
No significant changes were observed in the quality of life or physical activity levels in either group, suggesting that menstrual pain intensity alone may not sufficiently influence these domains in women with primary dysmenorrhea. Emotional regulation competency has been shown to enhance perceived quality of life, reflecting the intricate interplay between emotional and physical factors (Nazari and Griffiths, 2022). Furthermore, a broader range of life domains, such as social inclusion, autonomy, intimacy, and personal achievement, should be considered when assessing the quality of life (Skevington et al., 2021). Regarding physical activity, it is unlikely that variations in exercise levels during the initial days of menstruation translate to meaningful monthly changes in activity patterns. The effects of cryotherapy on physical activity may be more pronounced in cases of chronic pain rather than episodic menstrual pain.
This study is not exempt from several limitations that warrant consideration. The small sample size may limit generalizability, particularly for secondary outcomes such as sleep quality, quality of life, and physical activity. Additionally, the 3-month follow-up was relatively short, restricting evaluation of long-term effects such as sustained pain relief. Also, participants’ mean age of 24.5 years reflects a predominantly young cohort, limiting applicability to other age groups. Remote follow-ups via telephone posed challenges for accurately monitoring adherence, and the absence of objective measures raises potential variability in compliance. While socioeconomic factors were assessed, other confounding variables such as psychological factors and concurrent treatments were not fully explored. Additionally, the possibility of a placebo effect in the cryotherapy group cannot be ruled out, as the expectation of pain relief and the sensory experience of cold application may have contributed to perceived improvements. Future studies should explore strategies to differentiate true physiological effects from potential placebo responses. The short intervention period and its timing may have limited cryotherapy’s impact on gradual outcomes such as quality of life and physical activity. Future research should include larger, more diverse samples, extended follow-up periods, and robust adherence monitoring to better evaluate cryotherapy’s efficacy and applicability.
Despite its limitations, this study highlights cryotherapy as an effective, low-cost, and accessible therapeutic option for primary dysmenorrhea. With equipment readily available and no need for medical prescriptions or specialized supervision, cryotherapy offers a convenient and noninvasive alternative for pain management. Its practicality and safety reinforce its potential as a widely applicable intervention, providing a promising avenue for improving women’s health and well-being.
Conclusion
Cryotherapy appears to be an effective, accessible, and low-cost intervention for reducing pain intensity in nulliparous women with primary dysmenorrhea. While further research is needed to assess its long-term effects and broader benefits, these findings suggest that cryotherapy could be a valuable addition to the management of menstrual pain. Future studies should explore larger and more diverse samples, investigate different application durations and frequencies, and compare cryotherapy with other nonpharmacological treatments to better understand its efficacy and optimize its clinical application.
Footnotes
Authors’ Contributions
B.P.-D.: conceptualization (equal), data curation (lead), formal analysis (equal), methodology (equal), supervision (equal), visualization (lead), and writing—review and editing (equal); L.G.-R.: conceptualization (equal), investigation (equal), and writing—original draft (equal); S.M.-I.: conceptualization (equal), investigation (equal), and writing—original draft (equal); M.B.-D.: formal analysis (equal), resources (equal), methodology (equal), supervision (equal), and writing—review and editing (equal); and E.D.-M.: methodology (equal), project administration (lead), resources (equal), supervision (equal), and writing—review and editing (equal).
Data Availability Statement
Data obtained in this study will be made available by contacting with the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.