
Abstract
There are many established strategies to target normothermia in the perioperative period; however, hypothermia remains a common occurrence and can have significant impacts on patient outcomes, unanticipated admissions, and postanesthesia care unit (PACU) throughput. This pilot study serves to shed light on the effectiveness of using high-flow nasal cannula (HFNC) as an alternative to a Bair Hugger (BH). This pilot study compares 10 patients warmed to normothermia with HFNC in the PACU with 15 patients warmed with traditional BH. Patients in the HFNC group reached the goal temperature of 36°C 9.1 minutes faster than the BH group. However, these findings were not statistically significant (mean time: 72.1 minutes vs 81.2; p = 0.247). In addition, phase 1 recovery times were about 8 minutes longer in the HFNC group compared with the BH group but were also not statistically significant (mean time: 180.8 minutes vs 172.4; p = 0.338). Based on the initial data, HFNC may play an important role in the future by making PACU rewarming more efficient and therefore having a huge impact on PACU discharge times, unanticipated hospital admissions, delayed emergence from anesthesia, and morbid cardiac events. Further large scale, randomized control studies need to be done to investigate HFNC as an alternative rewarming method for hypothermic patients in the PACU.
Keywords
Introduction
It is well established that anesthesia impairs the body’s natural thermoregulatory control, and this in addition to a cool operative room environment can cause significant hypothermia via core-to-peripheral redistribution (Sessler, 2001). In addition, there are certain surgical factors that can promote excessive heat loss such as large exposed body surface area, open body cavities, and use of cold irrigation. There have been many proposed solutions in order to maintain normothermia in the perioperative period. These interventions include prewarming, passive insulation, active cutaneous heating, forced air warmers, circulating water warmers, radiant warmers, fluid warming, airway heating and humidification, titrating the operating room temperature, and more invasive internal warming systems such as extracorporeal membrane oxygenation (Sessler, 2001). Forced-air and resistive heating are currently the most effective noninvasive options, but newer technologies are being developed (Sessler, 2001). Patients at highest risk for hypothermia include an age of >60 years, intraoperative infusion volumes >1500 mL, blood loss >300 mL, major surgery, and operative time >2 hours (Liu and Qi, 2021).
This is important because despite these interventions, hypothermia is a common occurrence and can have significant effects. These include increased intraoperative blood loss and transfusion requirements, prolonged duration of neuromuscular blockade, morbid cardiac events, prolonged postanesthesia care unit (PACU) discharge times, increased surgical wound infections, delayed emergence from anesthesia, increased costs, unanticipated admissions, postoperative shivering, and decreased patient comfort (Kim, 2019; Sessler, 2001). Unexpectedly, the latest study on the topic from Sessler et al., the PROTECT trial, found limited differences in major cardiovascular outcomes between patients at 37°C and 35.5°C intra operatively (Sessler et al., 2022). Sessler concluded that maintaining patients at 35.5°C intraoperatively is sufficient (Sessler et al., 2022).
The literature suggests that high-flow nasal cannula (HFNC) may be an alternative option for PACU rewarming and the goal of this study is to investigate the feasibility and efficacy of this method in comparison with the standard of care.
Methods
HFNC overview
HFNC can deliver flows up to 60 L/min through a heated humidifier, which increases gas temperature and humidity up to 37°C and 44 mgH2O/L (Gilardi et al., 2020). The lungs have a total area of about 100–140 m2 and therefore have a large surface area available for both gas and heat exchange (Gilardi et al., 2020). In addition, heat transfer and conduction in the lungs is enhanced by full humidification (Gilardi et al., 2020). Benefits of HFNC include accurate delivery of the set fraction of inspired oxygen (FiO2), carbon dioxide washout from nasopharyngeal dead space, provision of small degree of positive end-expiratory pressure, and improved tolerance due to the comfortable interface (Gilardi et al., 2020). In comparison with traditional low-flow nasal cannula, HFNC delivers heated and humidified air that is much less irritating to the nasal mucosa and ultimately improves patient comfort.
Thermoregulatory responses are 80% determined by core temperature as are most complications related to hypothermia (Sessler, 2001). Warmer efficacy is determined by net heat transfer (Sessler, 2001). However, heat applied peripherally is not instantly transferred to the core and therefore warming methods that target the core rather than the periphery may be more effective (Sessler, 2001). Sessler et al. discusses that respiratory heat transfer theoretically maintains core temperature slightly better than a comparable amount of heat applied to the skin surface as the heat is transferred directly into the core thermal compartment (Sessler, 2001).
Bair Hugger overview
Forced-air warming systems, known as Bair Huggers (BHs), consist of an electrically powered heater–blower unit and a patient cover and are typically designed for single-patient use (Sessler, 2001). Radiation is the leading source of intraoperative heat loss and results from “photon-mediated transfer between two nonadjacent surfaces” (Sessler, 2001). Forced air reduces radiative loss by “replacing the cool surfaces of the room with a warm cover” (Sessler, 2001). Convection is the second most important source of intraoperative heat loss and works by a mechanism similar to wind chill factor (Sessler, 2001). Essentially, when air moves rapidly over the skin, it can increase conduction by several orders of magnitude therefore increasing heat loss (Sessler, 2001). “Forced-air warmers take advantage of this phenomenon by producing a flow of warm air across the skin” (Sessler, 2001).
This pilot was a prospective cohort study performed in the PACU of a level 1 trauma center and tertiary care center. This pilot investigates HFNC rewarming effectiveness across a variety of patients and surgeries and the results are likely generalizable to many institutions across the United States. This research falls under a project improvement IRB approval which covers all pathways in advanced recovery including temperature. Appropriate IRB processes have been followed.
This pilot study includes 10 patients who had either orthopedic or urologic surgery and arrived to the PACU with a temperature <34.9°C. Orthopedic and urology patients were chosen as the administration of HFNC would be less likely to interfere with healing or postoperative hemodynamics. The first 10 patients to meet these criteria during the study time period were chosen for the HFNC intervention group. Patients included in the study were selected by the charge nurse in the PACU and assigned to PACU nurses based on availability. The nurses were responsible for taking the arrival temperature, calling respiratory therapy to initiate the rewarming method, and recording rewarming times and phase 1 recovery times. The two primary outcomes of this study were rewarming time and phase 1 recovery time. There were no secondary outcomes. These patients were treated with HFNC until normothermia was reached, defined as 36°C. Exclusion criteria were patients having any other type of surgery than discussed above, patients that arrived with >34.9°C, and patients that had a BH placed for postoperative warming before the HFNC machine arrived.
These 10 patients were compared with 15 patients during the same time period who had a variety of types of surgery and were rewarmed in the PACU with the BH only. There was no blinding as this was a feasibility study. To confirm the intervention was actually received, patient charts were reviewed and the warming method and total warming time was confirmed. Data were collected by PACU nurses by writing down rewarming time, rewarming method, and phase 1 recovery time. The site of temperature measurement was not standardized during this pilot study, and we suggest this as an improvement in future research. Unfortunately, 1 patient was incorrectly included in the HFNC intervention group with an initial temperature of 36.3°C, greater than the cut off for inclusion. In future research, greater attention to inclusion and exclusion criteria is imperative. The data were then assembled into an excel spreadsheet and checked multiple times to ensure no errors were made in the entering of data. The data were then analyzed as discussed below. All patients with spurious or missing measurements were excluded.
Statistical analysis was performed via IBM’s Statistical Package for the Social Sciences (SPSS) data software. Both one-tailed and two-tailed t-tests were used to compare the mean time to reach 36°C and the mean phase 1 recovery time between the HFNC and BH groups. One-tailed and two-tailed t-tests were both done to see if HFNC shortened rewarming time and if there was a significant difference between the two data groups respectfully. We believe the data to be both precise and reliable as both the study and control group interventions are easy to implement and involve tasks many PACU nurses already complete on a daily basis.
Results
For the HFNC group, starting temperatures ranged from 33.6°C to 34.5°C (Table 1, Figs 1–2). The time in minutes to reach normothermia ranged from 29 to 125 minutes, with an average of 72.1 minutes. Average phase 1 recovery time was 180.8 minutes.

Time to normothermia—One group of patients arriving to the postanesthesia care unit (PACU) with temperatures <34.9°C received high-flow nasal cannula (HFNC) (n = 10) and were compared with patients with similar temperatures who were rewarmed with a Bair Hugger (BH) (n = 15). The time it took for a study subject’s temperature to reach 36°C (normothermia) was calculated and averaged for both groups. The average time to normothermia was 9.1 minutes faster in the HFNC group, but these results were not statistically significant (one-tailed t-test: p = 0.247; two-tailed t-test: p = 0.495). The range displayed in this figure was 29–125 minutes for the HFNC group and 30–146 minutes for the BH group. Two of the BH group values were considered outliers (145 and 146 minutes), represented by open circles on the box plot.
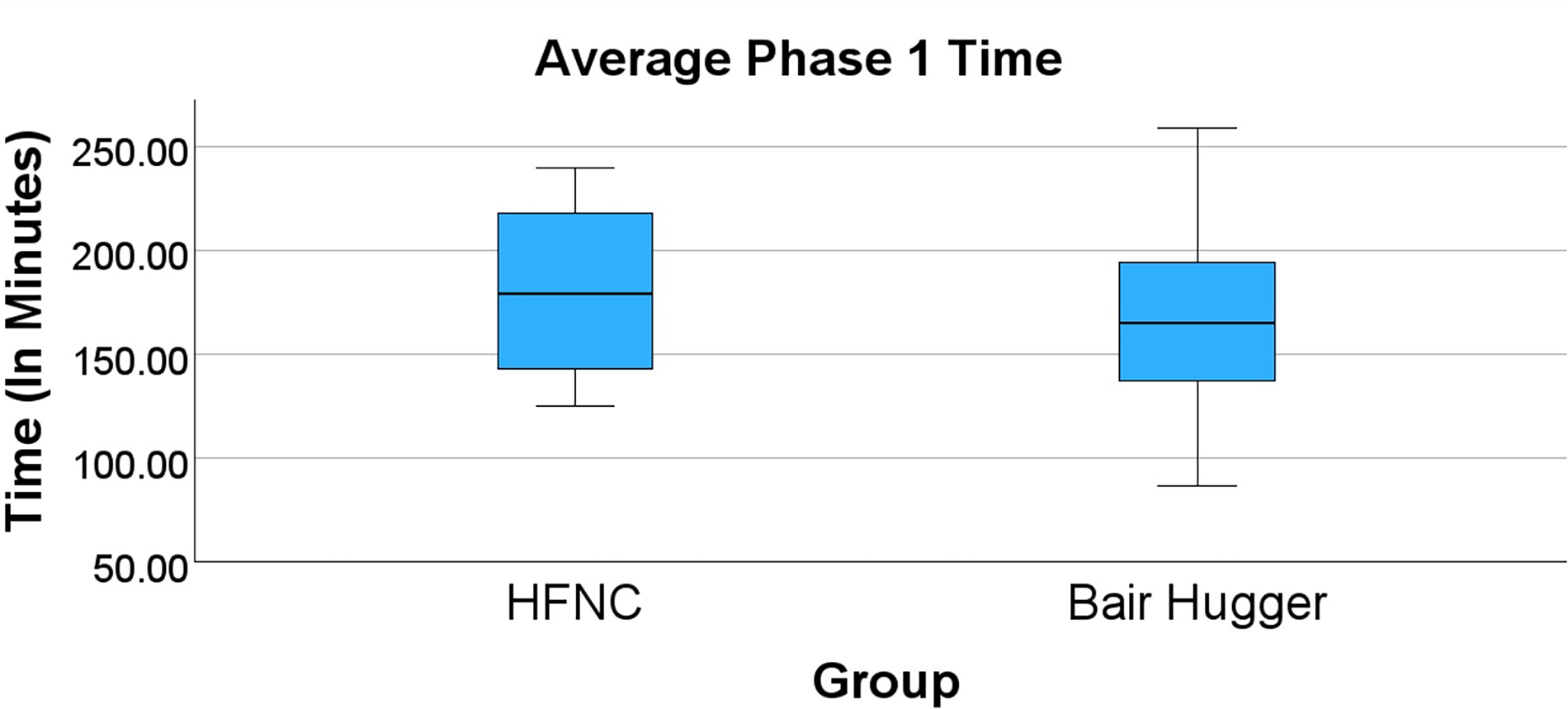
Average phase 1 time—Patients arriving to the postanesthesia care unit (PACU) with temperatures <34.9°C received either high-flow nasal cannula (HFNC) (n = 10) or were rewarmed with a Bair Hugger (BH) (n = 15). The time it took study participants in phase 1 of anesthesia recovery was calculated and averaged for both groups. The average phase 1 recovery time was 8.4 minutes faster in the BH group, but these results were not statistically significant (one-tailed t-test: p = 0.338; two-tailed t-test: p = 0.676). The range displayed in this figure was 125–240 minutes for the HFNC group and 87–290 minutes for the BH group.
High-Flow Nasal Cannula Group Data
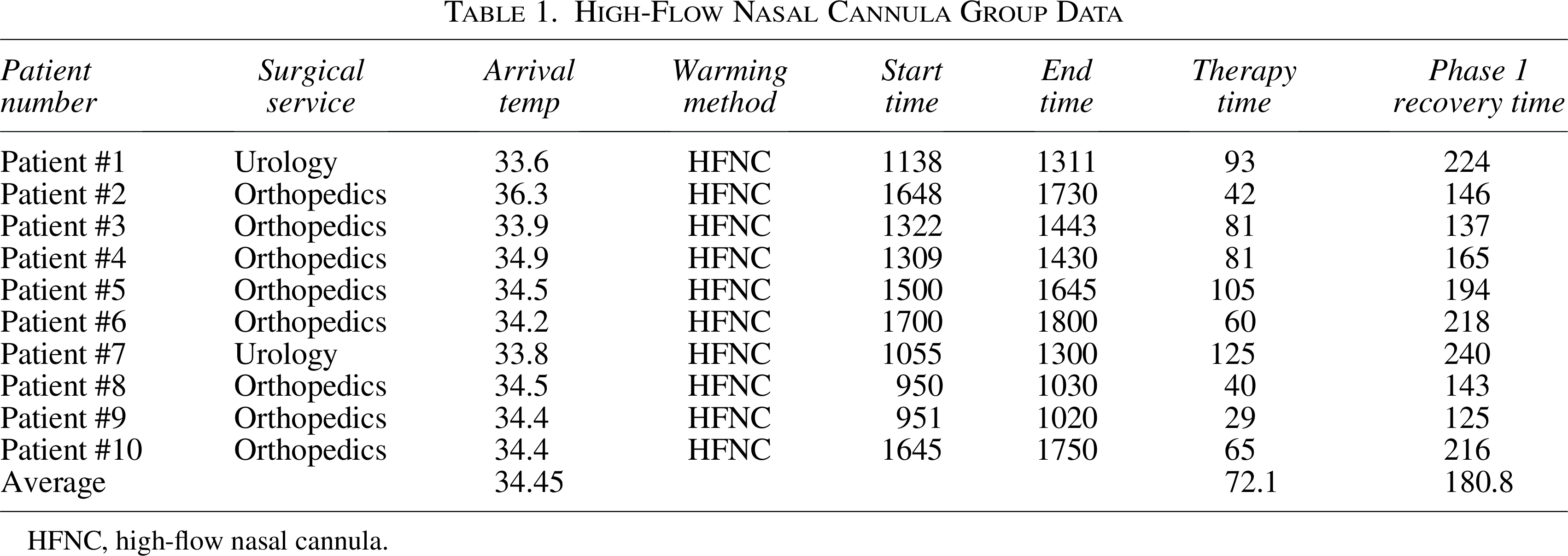
HFNC, high-flow nasal cannula.
For the BH group, starting temperatures ranged from 33.2°C to 35.4°C (Table 2, Figs 1–2). The time in minutes to reach normothermia ranged from 30 to 146 minutes, with an average 81.2 minutes. Average phase 1 recovery time was 172.4 minutes.
Bair Hugger Group Data

BH, Bair Hugger; HIPEC, Hyperthermic intraperitoneal chemotherapy.
Two tailed t-test p values were 0.495 for the time to reach normothermia and 0.676 for the phase 1 recovery time. One-tailed t-test p values were 0.247 for the time to reach normothermia and 0.338 for the phase 1 recovery time.
Discussion
Most of the current literature related to surgical hypothermia focuses on intraoperative prevention rather than postoperative management. Although all surgical and anesthesia teams strive to be proactive in treating and preventing hypothermia in the OR, hypothermia in the PACU is still a common occurrence. Most of the studies researching PACU rewarming focus on different types of body coverings such as blankets, radiant reheaters, and BHs (Ciufo et al., 1995; Liu et al., 2017; Yang et al., 2012). We found one study that explored humid heating rewarming, but it failed to show statistical significance in PACU rewarming (Brockbank et al., 2022).
Gilardi et al. looked at patients admitted to the emergency department over a 6-month period and compared rewarming with HFNC with no oxygen supplementation vs the institutional standard of care. They recorded body temperature every 15 minutes through a urinary catheter and compared the data with four matched control subjects (Gilardi et al., 2020). Subjects were matched on the basis of temperature at admission to the ER (Gilardi et al., 2020). The control subjects were treated with warm blankets and heated crystalloid infusion until their temperature reached 36°C (Gilardi et al., 2020). The HFNC subjects were treated with the institutional standard of care plus HFNC with gas flow set at 50–60 L/min, humidification chamber at 37°C, and FiO2 at 21% (Gilardi et al., 2020). All patients were fully awake, hemodynamically stable, and had no respiratory distress nor gas exchange impairment (Gilardi et al., 2020). They concluded the median time to rewarming was shorter in patients treated with HFNC, 120 minutes versus 345 minutes, with a Mann–Whitney p = 0.026 (Gilardi et al., 2020). Gilardi et al. cited no treatment-related side effects.
In our study, patients in the HFNC group reached the goal temperature of 36°C roughly 9 minutes faster than the BH group. Although a shorter time to reach normothermia, these results were not statistically significant (p value = 0.247). Interestingly, phase 1 recovery times were about 8 minutes longer in the HFNC group compared with the BH group. However, this longer recovery time was also not statistically significant (p value = 0.338).
To our knowledge, this study was the first to explore HFNC as an alternative treatment for postoperative hypothermia management in the PACU. Initial results appear promising as our study showed that HFNC was an effective rewarming method that may shorten time to normothermia as well as phase 1 recovery times.
It is important to also discuss the several limitations of HFNC. The machine is more costly compared with the BH both from a monetary perspective as well as time. This longer stay in phase 1 may be related to some of the disadvantages of HFNC, such as the need for more highly trained personnel, mobility issues, and longer set up time. The longer stay in phase 1 could also be in part due to nursing unfamiliarity with the technology as a method of rewarming and the institutional workflow to get it started. HFNC use is limited by the number of machines available in the hospital, and the machines themselves have limited mobility as well.
The goal of our study was to show initial data that HFNC was an effective modality for postoperative hypothermia in the hopes that it will spark further, larger sample size studies investigating its utility in hypothermia management postoperatively. Admittedly, our sample size of 25 patients (10 in the treatment group and 15 in the control group) limits our study, but it is a great starting point to explore the potential of HFNC for PACU rewarming and can be used to power future research. Another limitation of our study was the fluctuating anatomical sites the temperatures were taken from for various reasons; this should be standardized in future research.
Lastly, although the decrease in time to 36°C in the HFNC group was not statistically significant, there was still a decrease in a little over 9 minutes. With more studies and larger sample sizes, this decrease seen in our study could prove to be statistically significant and provide more efficient and effective rewarming.
Conclusion
In our study of just 10 patients, rewarming with HFNC compared with the current standard of care, the BH, shortened time to rewarming by 9.1 minutes. However, patients in the HFNC group had longer stays in phase 1 by 8.4 minutes. Further large scale, randomized control studies need to be done to investigate HFNC as an alternative rewarming method for hypothermic patients in the PACU. Based on the initial data, HFNC may play an important role in the future by making PACU rewarming more efficient and therefore having a huge impact on PACU discharge times, unanticipated hospital admissions, delayed emergence from anesthesia, and morbid cardiac events.
Authors’ Contributions
K.Pe.: Review and editing (equal). S.R.: Review and editing (equal). K.Po.: Conceptualization (supporting), data curation (primary), methodology (primary), and writing—review and editing (supporting). S.B., K.C., and M.M.: Conceptualization (supporting), methodology (supporting), and data curation (supporting). L.L.: Conceptualization (supporting), data curation (primary), methodology (primary), and writing—review and editing (supporting).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.