
Abstract
This investigation seeks to assess the impact of various temperature management approaches on the rates of death and organ failure among adult patients suffering from sepsis. A comprehensive search of PubMed, Embase, and CENTRAL was performed to identify randomized controlled trials (RCTs) published up to September 2024. These trials examined the impact of temperature management strategies on sepsis patients. Two independent investigators conducted literature screening, quality assessment, and data extraction. A meta-analysis was conducted using a fixed-effect model to evaluate outcome measures, including mortality and organ dysfunction. This study is registered with PROSPERO, CRD42024627677. The analysis incorporated eight RCTs, involving 1843 patients. The findings demonstrated that the management of hyperthermia markedly diminished the mortality risk among individuals suffering from sepsis (risk ratio = 0.47, 95% confidence interval [CI]: 0.37–0.59, p < 0.001), exhibiting low heterogeneity (I2 = 39%). However, the effects of hyperthermia on organ dysfunction remained unclear (Mean Difference [MD] = −0.92, 95% CI: −1.91 to 0.07, p = 0.07), exhibiting low heterogeneity (I2 = 0%). However, these effects on organ dysfunction were based on only two studies and 215 patients, which made them prone to a type II error. Hyperthermia management strategies are effective in reducing mortality among adults with sepsis. However, their impact on organ dysfunction requires further investigation through high-quality RCTs. Despite the limitations of this study, hyperthermia strategies offer a promising approach to multidimensional intervention in sepsis. Further studies should strengthen structured subgroup analyses and mechanistic studies based on RCTs to optimize treatment strategies under various clinical scenarios.
Introduction
The latest international sepsis guidelines and expert consensus have provided many opinions on the management strategies for sepsis but have not yet mentioned the management strategies for body temperature in adult sepsis patients. Fever and hypothermia have been observed in septic patients, and the impact of different body temperature management strategies on the prognosis of adult sepsis patients remains controversial (Thomas-Rüddel et al., 2021). Despite significant progress achieved in medical treatment, sepsis continues to be a predominant factor contributing to morbidity as well as mortality on a global scale, with nearly 50 million cases reported annually and causing over 11 million deaths. It represents a major global health threat (Liu et al., 2022).
Fever and hypothermia are the defining symptoms of sepsis, with the latter experienced by roughly 9–35% of individuals affected. Research indicates that infections in Intensive Care Unit (ICU) patients increase the likelihood of hypothermia, which is independently linked to higher morbidity and mortality. A rise in thermal regulation among ICU patients suffering from infections has been correlated with a decreased rate of in-hospital mortality, with the lowest danger of death observed when body temperature reached its zenith between 39.0°C and 39.4°C (Barichello et al., 2022). Conversely, a moderate fever can inhibit pathogen growth and enhance prognosis. However, an excessively high body temperature increases metabolic strain, causes organ damage, and worsens the outcomes.
In addition, hypothermia is independently associated with a high mortality rate in patients with sepsis, but its effect on long-term prognosis is still unclear (Rumbus et al., 2017). There is ongoing debate about the best temperature management strategies for septic patients, particularly regarding the optimal interventions for fever and hypothermia. This investigation seeks to use a meta-analytical framework to reveal the influence of diverse temperature management approaches on mortality rates and organ failure in the adult patients suffering from sepsis, with evidence-based recommendations made to optimize temperature management and improve patient outcomes for clinical practice.
Information and Methodology
This research adheres to the established protocols outlined by PRISMA 2020.
Literature search
An exhaustive inquiry was made using different terms such as “sepsis,” “body temperature management,” “fever,” “hypothermia,” “mortality,” “organ dysfunction,” and “randomized controlled trial (RCT).” The inquiry was conducted across various records, encompassing PubMed, Embase, and CENTRAL. The time frame for the search spanned from the establishment of each database to September 2024. The method of search as adopted in PubMed is detailed in Supplementary Table S1. In addition, the relevant conference literature was manually searched, and the references to included studies were reviewed to identify further pertinent studies.
Criteria for inclusion and exclusion
Type of study
Only RCTs were included.
Study population
The studies involving adult patients diagnosed with sepsis were delineated by the 2001 SCCM/ESICM/ACCP/ATS/SIS International Consensus Conference on sepsis definitions (Annane et al., 2005).
Interventions
The experimental group applied a strategy of hyperthermia management (T ≥ 38.3°C), while the control group adopted hypothermia management (T ≤ 35.6°C). The duration of the intervention was not restricted.
Outcome indicators
The primary outcome measures included mortality (e.g., in-hospital mortality, 28-day mortality). Focusing on organ dysfunction, secondary outcomes were assessed using the sequential organ failure assessment (SOFA) and multiple organ dysfunction syndrome (MODS) incidence.
Exclusion criteria
Research was omitted if they: (i) encompassed individuals with significant comorbid conditions (e.g., end-stage cancer, irreversible organ failure); (ii) were not published in Chinese or English; (iii) lacked full text or had incomplete data; (iv) did not report clear outcome measures; or (v) were duplicate publications or secondary analyses.
Evaluation of studies and extraction of data
Two investigators conducted a thorough literature screening and engaged in independent cross-checking. When differences of opinion arose, they were addressed through discourse or resolved by an impartial adjudicator. Additional information was obtained as much as possible for missing data by contacting the original authors. Literature information was recorded uniformly using a predesigned extraction form that included the following items:
(1) Basic information: type of study, first author, year of publication, study area, etc.; (2) study population: the sample size of patients, baseline characteristics (e.g., age, gender, condition score, etc.); (3) interventions: the specific methods of temperature management and control group interventions; (4) outcome indicators and outcome data: mortality, organ dysfunction, and related data of patients; and (5) risks of bias: randomization method, allocation concealment, blinding application, and so on. The outcome data were prioritized to extract key indicators from the immediate postintervention period to 28 days.
Literature quality assessment
The quality of the literature covered was evaluated using the Cochrane Risk of Bias Tool (version 5.4), which allows for (i) random sequence generation, (ii) allocation concealment, (iii) the blinding of implementation and outcome assessment, (iv) data completeness (whether to report missed visits and their treatment); (v) the selectivity of reporting of outcome metrics; and (vi) other factors that may lead to bias. The results of the evaluation are shown in Figure 1.
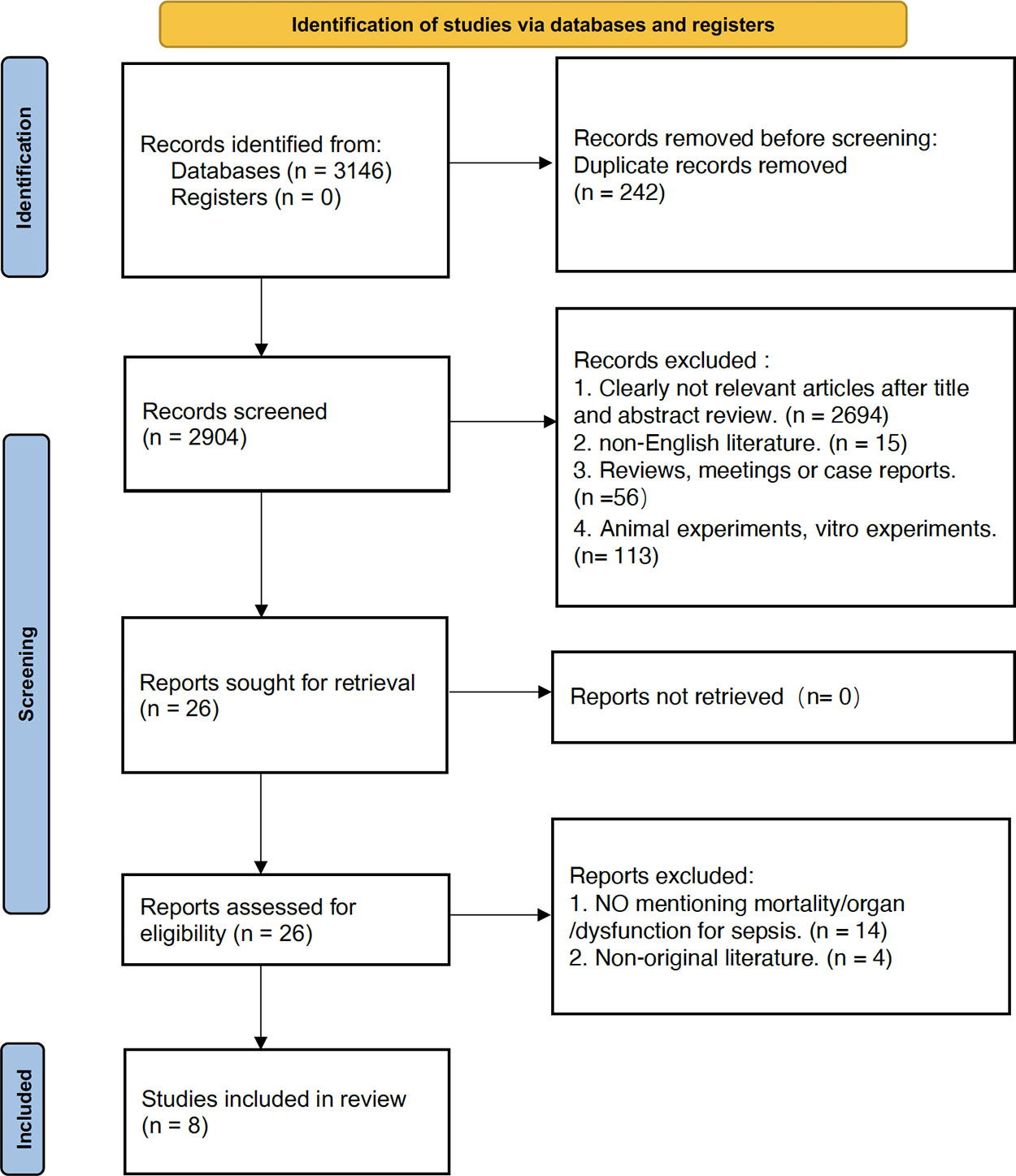
Flowchart of literature screening.
Statistical methods
The statistical analysis was conducted using Rev Man 5.4 software. The raw data were extracted from the literature as much as possible. If the literature failed to provide the mean and standard deviation of the pre- and postintervention differences, the postintervention mean minus the pre-intervention mean was taken as the mean of the pre- and postintervention differences, and the standard deviation was estimated according to the method of the Cochrane Handbook. For the measures using the same measurement tool, weighted MD was treated as the effect size, with its 95% CI computed. For the measures using various instruments for measurement, Standardized Mean Difference and its 95% CI were used. Based on Cohen's d, the intervention effect was classified into three levels according to the effect size: <0.2 as a low effect, 0.2–0.5 as a moderate effect, and >0.5 as a high effect. The diversity among the studies included was assessed using the p value and I2 of the χ2 test. The parameters p ≥ 0.10 and I2 < 50% suggest an absence of significant heterogeneity within the reviewed literature, thereby warranting the application of a fixed-effect model for the meta-analysis; otherwise, the full text was required to be read to exclude the factors of clinical heterogeneity, and to determine if the heterogeneity still could not be excluded. Subsequently, the random-effect model was employed for the meta-analysis. The differences in effect size between subgroups were compared according to the methods of the Cochrane Handbook. Statistical significance was established at p < 0.05.
Results
Outcomes of the literature review
The preliminary literature review produced 3146 documents that might fit the topic of this study, with 26 papers identified after initial screening through software de-weighting and the reading of topics and abstracts. After the eligibility and exclusion requirements of the literature were thoroughly examined, eight distinct works were selected upon an exhaustive review. The literature screening process and its corresponding results are illustrated in Figure 1 and Supplementary Table S1.
Attributes of the incorporated studies
Eight papers were published from 2000 to 2022, involving 1843 adult patients with sepsis. The essential data of the test and control groups were comparable, all with different temperature management strategies, as illustrated in Table 1.
Fundamental Attributes of the Literature Included
Results of the methodological quality assessment of the literature presented
The Cochrane Risk of Bias Assessment Tool was adopted in eight studies, as illustrated in Figure 2.
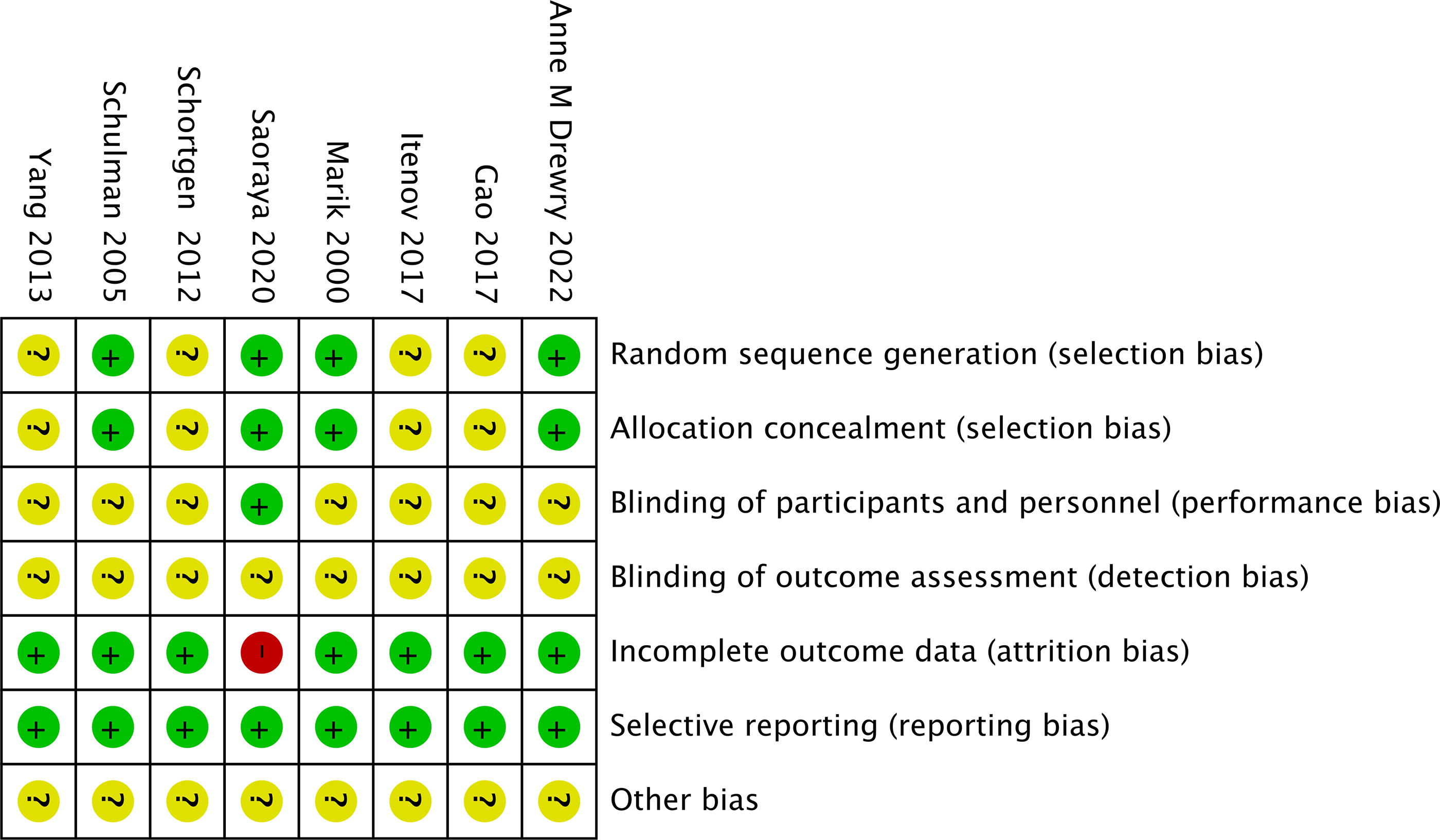
Includes study bias risk.
Meta-analysis of findings
Main outcome indicators: mortality (in-hospital mortality, 28-day mortality)
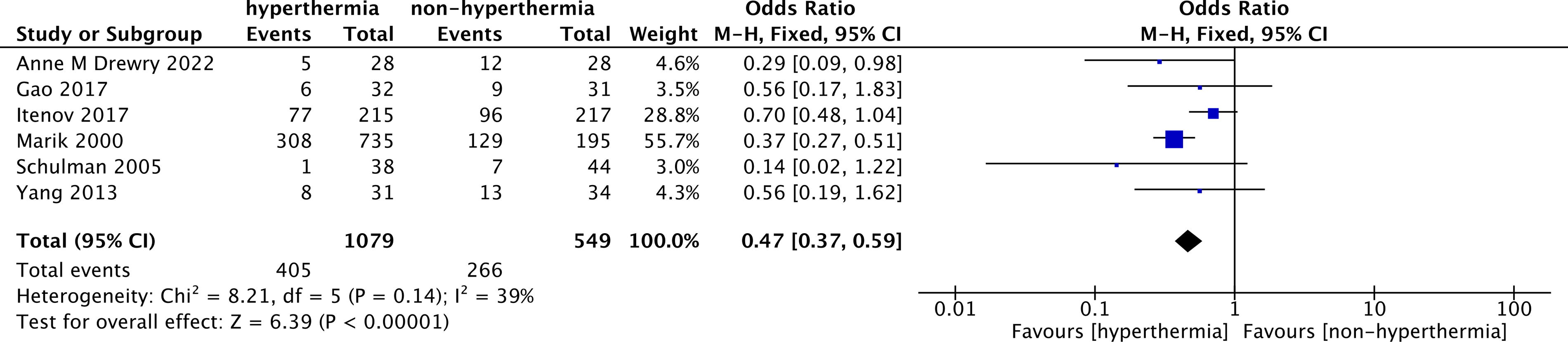
Six RCTs were incorporated, involving 1628 patients. Heterogeneity analysis showed that χ2 = 8.21, p = 0.14, and I2 = 39%, suggesting that inter-study heterogeneity was low and the fixed-effect model was applicable. The meta-analysis conducted using the fixed-effect model revealed a statistically significant reduction in the 28-day all-cause mortality rate within the hyperthermia management cohort compared with the hypothermia management cohort (risk ratio [RR] = 0.47, 95% CI [0.37, 0.59], p < 0.00001), with a Z-test statistic of 6.81 (p < 0.001). The difference was statistically significant. Individual studies (e.g., Yang et al., 2013) contributed less to the total effect size due to their considerable 95% CI spans but failed to significantly change the overall direction. Most studies had effect sizes consistent with the combined effect, and the combined effect size (diamond) was to the left of RR = 1, further confirming the clinical validity of hypothermia management (Fig. 3).
Funnel plot analysis of included studies.
As indicated by the funnel plot (Fig. 4), the distribution of the included studies exhibited a degree of symmetry, implying a minimal probability of publication bias. The standard errors (SEs) and RRs of the studies showed a reasonable distribution pattern, with most of the studies concentrated in the top region of the funnel, indicating a large sample size and high precision of the results. Furthermore, the study points were uniformly allocated on either side of the central vertical axis (RR = 1), substantiating the stability and reliability of the analytical results. This meta-analysis did not show significant publication bias, and the statistical results were credible, providing reliable evidence for the protective effect of hypothermia management on clinical outcomes among sepsis patients.
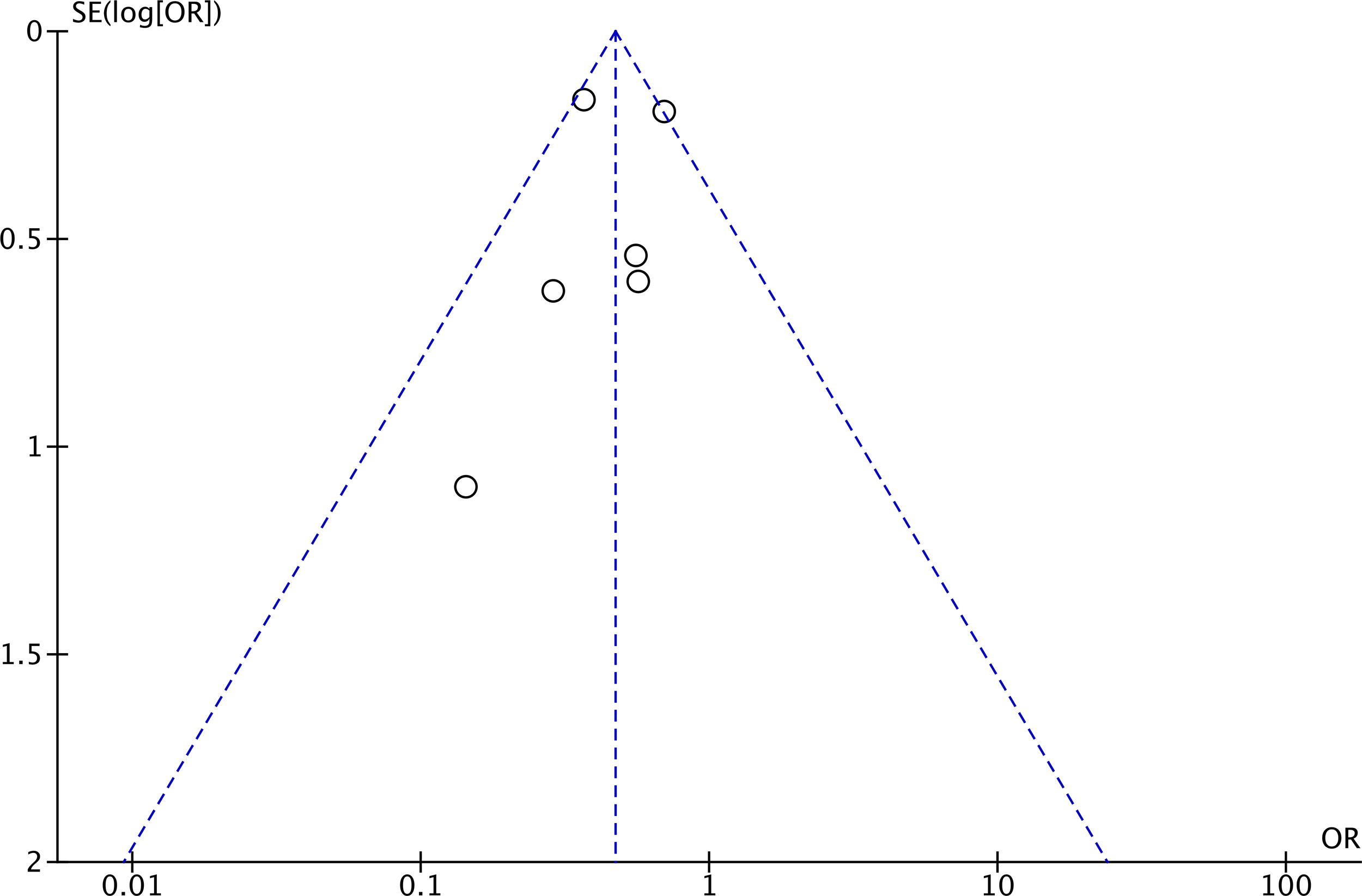
Funnel plot analysis of included studies.
Secondary outcome indicators: organ dysfunction (SOFA score)
A total of two RCTs containing 215 patients were included, and heterogeneity analysis showed that χ2 = 0.04, p = 0.84, and I2 = 0%, suggesting that the inter-study heterogeneity was low and the fixed-effects model was applicable. As indicated by the meta-analysis conducted using the fixed-effect model, the 14-day Sequential Organ Failure Assessment (SOFA) score did not demonstrate a statistically significant improvement in the hyperthermia management group compared to the hypothermia management group (MD = −0.92, 95% CI [−1.91, 0.07] p = 0.07), with a Z-test statistic of 1.83. The difference was not statistically significant (Fig. 5).

Forest plot analysis of included studies.
Discussion
Representing the body's adaptive reaction to an infection, fever is a vital clinical indicator in the individuals suffering from sepsis. More than 90% of ICU sepsis patients experience fever (Srzić, 2022). Therefore, fever is regarded as a significant independent risk factor for mortality among patients in the ICU. As a strategy aimed at organ protection, temperature management has been extensively employed in managing fever, effectively diminishing tissue oxygen consumption through various mechanisms. Several prior investigations have been conducted to explore the influence of temperature regulation on the survival rates of patients suffering from sepsis. For example, it has been found that in sepsis patients, hypothermia is associated with an increased mortality rate, while fever is not (Tan et al., 2024). The patients do not benefit from temperature control even though it is widely used (Young et al., 2019). However, there is no clear clinical evidence on what temperature management strategies should be used for septic febrile patients and which temperature goals maximize patient prognosis.
This study encompasses eight RCTs involving 1843 adult patients suffering from sepsis, with publications spanning from 2000 to 2022. The intervention group employed hyperthermia management (HT), while the control group adopted hypothermia management (LT). The target temperature range for the study was clearly defined, with hyperthermia management maintaining a temperature of ≥38.3°C and hypothermia management maintained at ≤35.6°C (Marik and Zaloga, 2000). Patient characteristics showed a mean age of approximately 65 years with a balanced gender ratio (male/female close to 1:1). Most studies set strict entry criteria, including the confirmed cases of acute sepsis or septic shock, to ensure the relevance and consistency of results. Regarding interventions, some studies applied intensive temperature control strategies (e.g., therapeutic normothermia management), whereas the control group received conventional temperature management or no temperature control intervention. In addition, the trials included several interventions to regulate body temperature, such as acetaminophen, a water-flow cooling blanket, ice packs, an automatic cooling blanket, and ice-cold bed sheets. Each of these interventions may have a different effect on mortality, which was not explored in depth due to the limitations of the included article. Future research will also aim to identify which strategy is superior in reducing mortality rates. Regarding primary outcome indicators analysis, meta-analysis showed that hyperthermia management significantly reduced 28-day all-cause mortality among the patients, providing reliable evidence to support standardized temperature management (Gao et al., 2017). Regarding secondary outcome metrics analysis, hyperthermia management versus hypothermia management strategies did not demonstrate an advantage in organ dysfunction in septic patients. This may be related to the insufficient number of cases studied and the lack of high-quality RCT studies. In addition, this conclusion was based on only two studies and 215 patients, as a result of which it could easily be subject to a type II error. More research should be conducted in the future to explore this issue. Other studies have shown that the feasibility of maintaining fever control within 24 hours is positively correlated with the effectiveness of the intervention, which is clinically significant, especially for early intervention in ICU patients (Liu et al., 2021). In addition, hyperthermia management has shown potential clinical benefits in reducing ICU length of stay, lowering the cost of anti-infective therapy, and optimizing patient prognosis. This may be because hyperthermia management exerts a protective effect through multiple mechanisms, including immunomodulation and hemodynamic stabilization. A moderate hyperthermia strategy enhances monocyte function and increases human leukocyte antigen expression level while inhibiting the release of excessive pro-inflammatory factors and preventing inflammatory storms (Zhang et al., 2023). In addition, temperature-controlled management can improve microcirculatory perfusion, optimize tissue oxygen supply and organ metabolism, and significantly reduce the incidence of MODS (Beadle et al., 2023). High body temperatures may also accelerate pathogen clearance by enhancing host resistance to infection. Studies have demonstrated that the synergistic effect of temperature management and inflammation modulation can effectively protect vital organ function, reduce sepsis-related mortality, and mitigate complications (Shimazui et al., 2020).
In nonclinical practice, medical personnel ought to adopt a tailored temperature regulation approach that considers the specific circumstances, including a designated temperature range informed by the patient's age, pre-existing conditions, and the severity of sepsis. Early intervention for temperature control is critical and needs to be rapidly assessed and implemented at the time of patient admission, combined with dynamic monitoring indicators (e.g., acute physiology and APACHE II, cytokine levels, hemodynamic parameters) to optimize the effectiveness of the intervention. In addition, the implementation of temperature management relies on multidisciplinary collaboration, including the joint involvement of infectious diseases, critical care medicine, and the nursing team to ensure comprehensive and safe treatment. Future clinical practice should further standardize the implementation pathway of temperature control interventions, enhance the training and education of healthcare professionals, and conduct more refined studies on subgroups of high-risk patients (e.g., elderly patients or those with multiple comorbidities) to optimize temperature management strategies and improve clinical outcomes.
The findings from the risk of bias assessment indicated that certain studies posed an unclear risk to random sequence generation and allocation concealment, potentially leading to selection bias. However, most of the studies in the blinded implementation and the assessment of completeness of the outcome data demonstrated a minimal risk and overall high data quality. Specifically, these studies often involved independent investigators for data collection and follow-up, reducing the potential of experimental blinding and measurement bias. However, individual studies (e.g., Yang et al., 2013) were assessed as having a significant risk of bias, which can be attributed to the limited sample sizes and shortcomings in both study design and reporting methodologies. In addition, a few studies inadequately described the balanced baseline characteristics of the experimental and control groups, which may affect the robustness of the outcomes of meta-analyses.
Although the results of this meta-analysis show the significant clinical benefits of hyperthermia management in terms of mortality in septic patients, certain limitations remain. First, the restricted quantity of incorporated studies and the comparatively modest sample sizes restricted statistical effectiveness and reduced the generalizability of the findings. Furthermore, some of the included research failed to address traumatic brain injury or other neurological diseases, such as subarachnoid hemorrhage and stroke, where hyperthermia can be harmful and affect mortality, thereby influencing the conclusions. Second, the randomization methods and allocation concealment strategies adopted in some studies were poorly described, thus increasing the risk of selection bias. Third, the wide variation in intervention methods and temperature-controlled targets across studies may have increased heterogeneity of the results. In addition, the description of patients’ baseline characteristics in some studies was not comprehensive enough to completely exclude the interference of potential confounders. Finally, this management showed significant variation, encompassing both pharmacologic and external mechanical cooling devices. This suggests that other factors, such as drug effects and changes caused by the cooling method, might explain some of the outcomes. However, the present study has not yet explored them respectively that are involved due to the limited studies included.
Conclusion
In summary, the results of this meta-analysis support hyperthermia management as an essential intervention strategy for sepsis treatment in terms of reducing mortality rates among the individuals afflicted with sepsis. However, there is a lack of adequate evidence to support hyperthermia management strategies for reducing the potential for organ dysfunction in sufferers, for which the hyperthermia management strategies for the patients with sepsis should still be viewed cautiously and dialectically. To achieve this objective, the clinical implementation must consider the patient's distinctive features, the severity of the illness, any underlying conditions, and the individual's tolerance to temperature control interventions. In addition, hyperthermia management needs to ensure the safety and efficacy of the intervention by incorporating real-time monitoring and multidisciplinary collaboration.
Ethics Approval and Consent to Participate
As this is a systematic review and meta-analysis, ethics approval and consent to participate are not applicable.
Author Disclosure Statement
No competing financial interests exist.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.