
Abstract
The objective of this study was to assess the adherence to inclusion criteria for therapeutic hypothermia (TH) in neonates with hypoxic-ischemic encephalopathy (HIE) and to survey current attitudes on TH. This multicenter observational study therefore combined a retrospective analysis of the Swiss National Asphyxia and Cooling Register (2011–2023) and a prospective survey (2024) among neonatologists in the Canton of Zurich, Switzerland. A total of 456 neonates with HIE were registered in the Swiss National Asphyxia and Cooling Register in the Canton of Zurich, Switzerland, between 2011 and 2023. The rate of TH (52.6% [2011–2017] versus 52.0% [2018–2023]) as well as the incidence of off-protocol cooling remained stable over time (p = 0.614). The survey response rate was 69.5% (57/82). Difficulties with clinical grading of encephalopathy were identified. Subjectively, respondents considered themselves more generous to initiate TH. In conclusion, register data reflected good adherence to inclusion criteria for TH. The survey confirmed willingness to consider TH in milder HIE cases. However, there was no drift in clinical practice—yet?
Introduction
Hypoxic-ischemic encephalopathy (HIE) affects 1–8/1000 neonates in industrialized countries (Douglas-Escobar and Weiss, 2015). HIE is an important cause of mortality and morbidity and is responsible for various perinatally acquired brain injuries such as cerebral palsy, cognitive dysfunction, or epilepsy (Mathew et al., 2022). Therapeutic hypothermia (TH) is the most effective and the only evidence-based neuroprotective therapy for moderate and severe HIE (Azzopardi et al., 2009; Douglas-Escobar and Weiss, 2015; Jacobs et al., 2013; Mathew et al., 2022; Shankaran et al., 2005).
To be classified for TH, several criteria must be met, with some variations between countries (Azzopardi et al., 2009; Jacobs et al., 2013; Shankaran et al., 2005). In Switzerland, the Swiss National Asphyxia and Cooling Register was implemented in 2011, including a national cooling protocol (National Asphyxia and Cooling Register, n.d.). TH is generally initiated within the first 6 hours of life in neonates of ≥35 weeks gestational age with moderate to severe HIE. The Swiss National Asphyxia and Cooling Register facilitates the systematic recording of maternal, perinatal, and neonatal data; temperature management during TH and rewarming as well as short-term outcomes until discharge from the neonatal intensive care unit (NICU) (Brotschi et al., 2014, 2015; Grass et al., 2021). Adherence to established national cooling criteria can be monitored.
However, studies showed that neonates who did not meet the cooling criteria could also benefit from TH and had the same short- and long-term outcomes as neonates who met the criteria (Smit et al., 2015). Accordingly, the cooling criteria have presumably been implemented less strictly over the years so that neonates with milder HIE have also been included in TH (Parmentier et al., 2020). Despite the established evidence for the neuroprotective effect of TH in moderate and severe HIE, large, randomized controlled trials of TH in mild HIE are currently pending (NCT03409770, NCT04621279, and NCT04176471).
Accordingly, the question arises as to whether and how the patient characteristics of cooled neonates with HIE have changed in Switzerland over the past decade. Data from the Swiss National Asphyxia and Cooling Register were evaluated objectively regarding inclusion criteria for TH (2011–2017 versus 2018–2023), and the subjective attitude of neonatologists towards TH was determined by a survey (2024). As clinical practice continues to evolve, it is essential to evaluate if the inclusion criteria for TH have expanded to include milder HIE cases and to understand current attitudes among neonatologists. By assessing trends in TH application through registry data and clinician surveys, this study aims to understand how current practices align with or deviate from established protocols.
Materials and Methods
Study population and data collection
This observational study combined a retrospective analysis of prospectively collected data from the Swiss National Asphyxia and Cooling Register (2011–2023; TH and normothermia) and a prospective survey (2024) among neonatologists treating neonates with HIE, both in cooling centers and referral centers in the Canton of Zurich, Switzerland. Data collection, evaluation, and publication for this study were approved by the Zurich Cantonal Ethics Committee (KEK-ZH Number 2024–00714). STROBE guidelines were followed for reporting this study.
Swiss National Asphyxia and Cooling Register data of neonates receiving TH
Further analyses of this retrospective multicenter cohort included neonates ≥35 weeks gestational age (as of 2015, 2011–2014: ≥36 weeks gestational age) with HIE receiving TH between January 2011 and December 2023 in the participating neonatal cooling centers of the University Children’s Hospital Zurich, University Hospital Zurich, and Cantonal Hospital Winterthur. All parents of included neonates provided written informed consent for registration in the Swiss National Asphyxia and Cooling Register, including further scientific use of registered data.
All neonates were treated according to the Swiss National Asphyxia and Cooling Register Protocol (Brotschi et al., 2015). TH with whole-body cooling was initiated within 6 hours of birth, targeting 33.0°C to 34.0°C core temperature, and was continued for 72 hours. Inclusion and exclusion criteria for TH according to the national cooling protocol were applied (Brotschi et al., 2015; Grass et al., 2021; Supplementary Appendix A1). The flowchart in the (Supplementary Appendix A1) to initiate TH depicts the so-called “A-criteria” (APGAR ≤5 at 5 [10] minutes; need for ventilation at 10 minutes; worst pH, base deficit, and lactate within the first 60 minutes of life) and “B-criteria” (severity of encephalopathy, assessed by Sarnat score [Sarnat and Sarnat, 1976] and/or Thompson score [Thompson et al., 1997]; seizures). Neonates with moderate HIE (Sarnat score II [Sarnat and Sarnat, 1976] and/or Thompson score 7–12 [Thompson et al., 1997]) to severe HIE (Sarnat score III [Sarnat and Sarnat, 1976] and/or Thompson score 13–22 [Thompson et al., 1997]) within the first 6 hours of life qualify for TH according to national guidelines. The Sarnat score and Thompson score can be used interchangeably according to the national cooling protocol. However, Thompson scoring was only implemented gradually in Switzerland until 2015, after the introduction of the Swiss National Asphyxia and Cooling Register in 2011.
To evaluate differences between protocol-cooled and off-protocol-cooled neonates (did not fulfill A-criteria and/or B-criteria; ≤35 weeks gestational age; ≥6 hours of age at initiation of TH; evidence of major congenital malformation), those receiving off-protocol cooling based on clinical judgment of the attending neonatologist were included in the statistical analysis.
Maternal demographics, pregnancy data, delivery variables, perinatal and neonatal data (including outcomes until discharge from the NICU), were extracted from the Swiss National Asphyxia and Cooling Register for statistical analysis. For the longitudinal analysis of adherence to protocol, the data was halved into two time periods of 2011–2017 and 2018–2023 for comparison.
Within the dataset of cooled neonates analyzed, the Thompson score before cooling was missing in 18%, umbilical artery pH in 15%, and base deficit in 10%. All other analyzed data items were ≥99% complete. To compare between time periods, we used the chi-square test with Yates correction for categorical variables and the Mann–Whitney U test for metric variables. p-values were used as a quantitative measure of the strength of statistical evidence rather than rejecting null hypotheses.
Survey of Swiss neonatologists on “TH for neonates with HIE”
To compare objective data from the register to clinical practice and subjective perceptions, this study included a survey of neonatologists on their attitudes toward TH in HIE. Participating neonatologists worked either in a neonatal cooling center providing definitive indication for TH or in a neonatal unit indicating referral of neonates with HIE for assessment of eligibility for TH to a higher level of neonatal care.
Both questionnaires were created using LimeSurvey (LimeSurvey Website, n.d.) by the study team consisting of three practicing neonatologists (senior consultants) and one medical student. There was no validated survey available in the literature. The questionnaires were piloted by a neonatologist, and input was also obtained from various practicing pediatricians. The participant’s consent was implied through their voluntary completion of the survey.
The survey was distributed to all neonatologists in the three neonatal cooling centers of the Canton of Zurich, Switzerland (University Hospital Zurich, University Children’s Hospital Zurich, and Cantonal Hospital Winterthur; [Swiss Society of Neonatology, n.d.]). A questionnaire (Supplementary Appendix A2) consisting of 24 questions (including 19 multiple-choice questions, 4 nominal questions with a rating of 0–10, and one open-ended question) was sent to senior physicians (division heads, senior consultants, consultants, and fellows) in these hospitals via email.
A similar, slightly modified survey was sent to the referring neonatology units in the Canton of Zurich (Zollikerberg Hospital, City Hospital Zurich, and Buelach Hospital; [Swiss Society of Neonatology, unit accreditation, website]). Here too, senior physicians (division heads, senior consultants, consultants) were asked about their views on TH for HIE. This survey (Supplementary Appendix A3) consisted of 21 questions (including 17 multiple-choice questions, 3 nominal questions with a rating of 0–10, and one open-ended question) and was distributed by email.
All eligible employees (including the email addresses) in the surveyed NICUs were confirmed by the corresponding division heads. In the referral hospitals, the division heads indicated two employees with recent relevant work experience in neonatal cooling centers who thus received both questionnaires. For both surveys, a reminder email was sent after 1 month, followed by the closure of the survey after an additional 4 weeks. All survey responses were analyzed descriptively using Microsoft Excel.
Results
Swiss National Asphyxia and Cooling Register
Between January 2011 and December 2023, 456 neonates with HIE were registered in the Swiss National Asphyxia and Cooling Register by the three neonatal cooling centers and by two of the three referring neonatology units (one unit did not enter data) in the Canton of Zurich, Switzerland. Of these 456 neonates with HIE, 229 neonates received TH; the remainder of 227 neonates were treated with normothermia. Figure 1 (Fig. 1) depicted the ratio of neonates with TH to neonates with normothermia (no TH) over time. The rate of TH remained stable at 52.6% (2011–2017) versus 52.0% (2018–2023) of neonates with HIE who received TH. There was an increased number of neonates with HIE registered during the COVID-19 pandemic years 2020–2021.
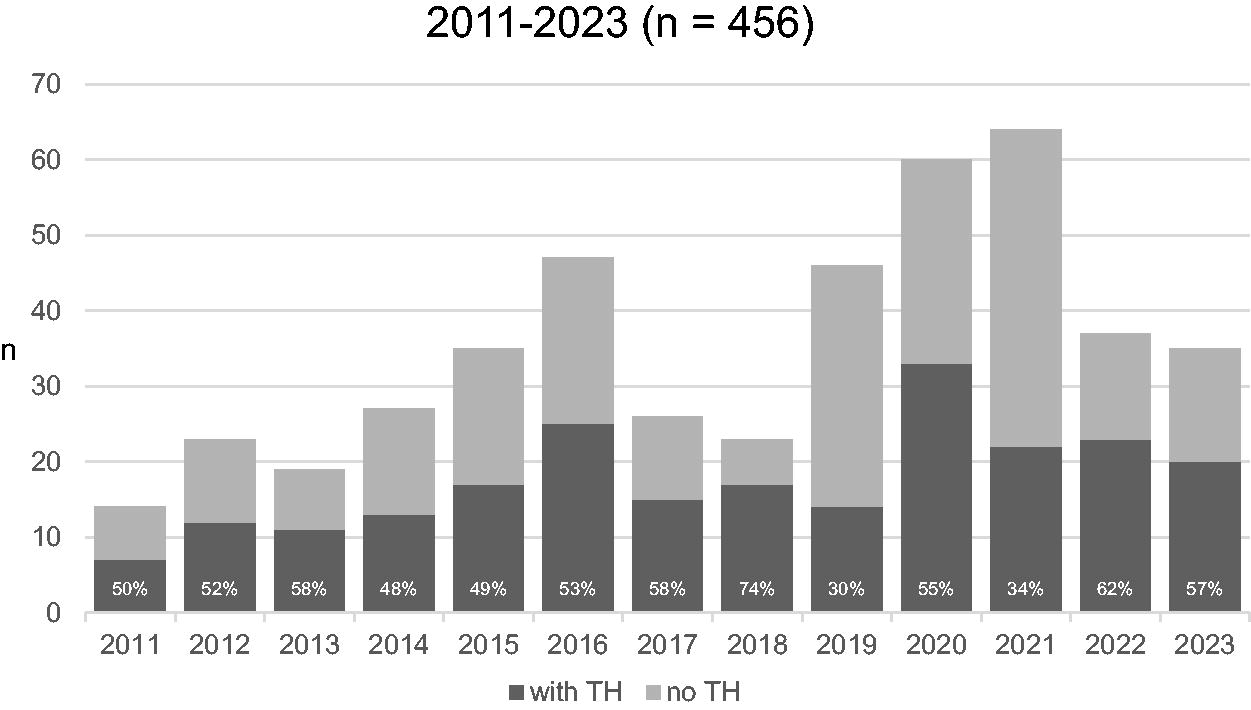
Annual data entries in the Swiss National Asphyxia and Cooling Register in the Canton of Zurich, Switzerland. Absolute numbers of neonates with TH (therapeutic hypothermia) and with normothermia (no TH) in the years 2011–2023 in the Canton of Zurich, Switzerland. Percentages (%) for neonates with TH. Note: The two largest neonatal cooling centers entered data as of 2011 and the third neonatal cooling center entered data since 2014. Two referring hospitals entered data since 2015 and 2019, respectively. One referring hospital did not enter data.
Of neonates with HIE receiving TH, perinatal (maternal, pregnancy, and delivery data) as well as neonatal characteristics and outcomes until NICU discharge were compared between 2011 and 2017 and 2018–2023 in Table 1.
Comparison of Neonates with HIE Receiving TH and of Cooling Characteristics between 2011–2017 and 2018–2023
Data extracted from the Swiss National Asphyxia and Cooling Register on neonates receiving TH (therapeutic hypothermia).
Neonatal outcomes as per definitions in (Grass et al., 2021).
CTG, cardiotocogram; PPHN, persistent pulmonary hypertension; GA, gestational age.
Data on the process of TH and off-protocol cooling details were compared also (Table 1). There were no passively cooled neonates in the later period. The incidence of off-protocol cooling remained stable over time (p = 0.614). The longitudinal analysis of the severity of encephalopathy evaluated by Thompson score [Thompson et al., 1997] as inclusion criteria for TH (B-criteria) according to the Swiss National Asphyxia and Cooling Protocol (Supplementary Appendix A1) was depicted in Figure 2 (Table 1 and Fig. 2).
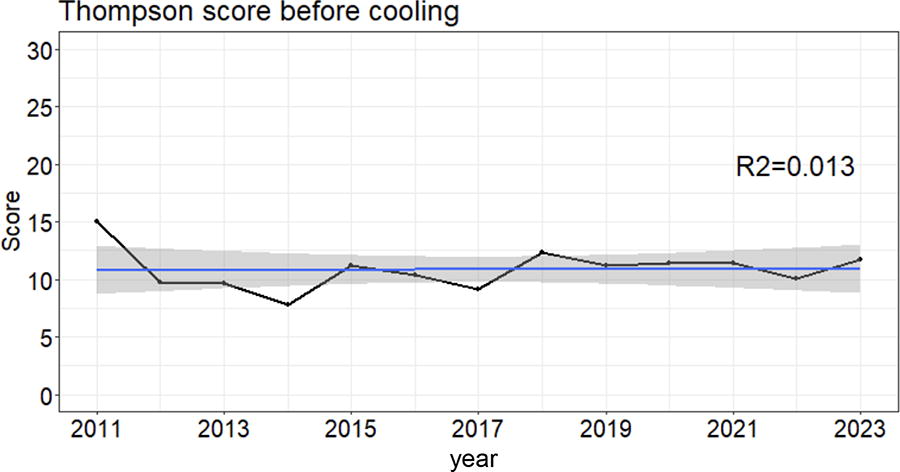
Longitudinal analysis of the Thompson score before initiation of TH. Severity of encephalopathy evaluated by Thompson score (Thompson et al, 1997) as inclusion criteria for TH (therapeutic hypothermia) according to the Swiss National Asphyxia and Cooling Protocol (shown in Supplementary Appendix A1). Median Thompson score per year (black line) with smoothed linear fit (blue line), 95% confidence interval for the fit (gray area) and goodness of fit (R2 = 0.013).
Survey of Swiss neonatologists on “TH for neonates with HIE”
The overall response rate was 69.5% (57/82): 54.5% (12/22) in the referring hospitals and 75.0% (45/60) in the cooling centers in the Canton of Zurich, Switzerland. All participants were board-certified pediatricians (mainly with training in Switzerland); almost all had additional sub-specifications in neonatology and/or pediatric intensive care, working mainly as (senior) consultants in the surveyed neonatology units. Fellows in subspecialty training were included. Among the participants from referring hospitals, 83.3% (10/12) had over 10 years of clinical experience. One respondent had between 8 and 10 years and one respondent between 5 and 7 years of experience (1/12, 8.3% each). In the cooling centers, 73.3% (33/45) of the respondents had more than 10 years of work experience, 17.8% (8/45) had 8–10 years, and 8.9% (4/45) had 5–7 years of work experience. This was also reflected in the numbers of treated neonates with HIE with TH: 77.8% (35/45) of the participants in the cooling centers treated more than 25 neonates with TH. Most respondents rated themselves as (very) familiar with the diagnosis of HIE (Supplementary Fig. S1), which was supported by reports on regular education and teaching on HIE (cooling centers: teaching available in 84.4% (38/45), information by register representative in 51.1% (23/45); referring hospitals: teaching available in 50.0% (6/12), information by register representative in 8.3% (1/12)).
The first survey topic was adherence to the Swiss National Asphyxia and Cooling Protocol, including inclusion criteria for TH. Most neonatologists in the referring hospitals stated strict adherence to protocol, whereas neonatologists in the cooling centers reported less adherence (Fig. 3). Adherence to protocol was associated with perception of good feasibility of the A-criteria and B-criteria in clinical practice (Fig. 3).
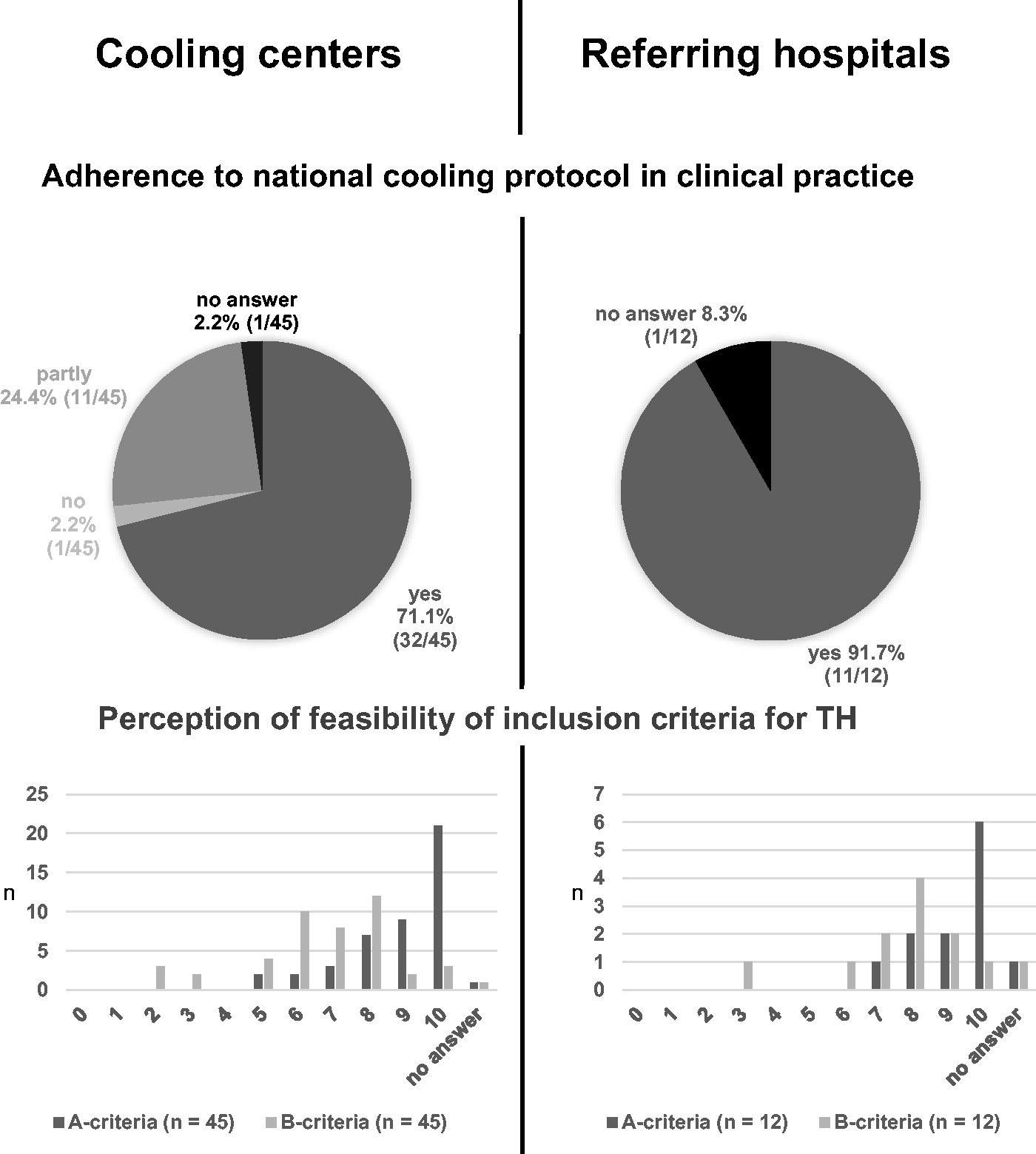
Adherence to protocol and feasibility of inclusion criteria for TH. Nominal scale on feasibility of A-criteria and B-criteria for inclusion for TH (therapeutic hypothermia); 0 = not at all feasible and 10 = very easily feasible (x-axis) and absolute number of respondents (y-axis).
Most respondents from cooling centers and referring hospitals reported that A-criteria were easier to apply than B-criteria (Fig. 3). Regarding the B-criteria, i.e. clinical assessment of severity of encephalopathy, the respondents were more familiar with the Thompson score than the Sarnat score (Supplementary Fig. S2). Most respondents used both scores (64.4% [29/45] in cooling centers and 50.0% [6/12] in the referring hospitals), but among those who only used one score, the Thompson score was preferred.
In view of the possibly difficult application of A-criteria and B-criteria, participants were invited to report additional criteria (multiple answers possible) for consideration of TH. Among the 45 respondents from the cooling centers, 26.7% (12/45) relied solely on A- and B-criteria. Additionally, 62.2% (28/45) incorporated findings on amplitude-integrated electroencephalogram (aEEG) into their assessments, and 26.7% (12/45) considered perinatal sentinel events separately. A similar pattern emerged among the referring neonatologists: 33.3% (4/12) relied solely on A- and B-criteria, 33.3% (4/12) considered aEEG, and 25.0% (3/12) took perinatal sentinel events into account.
The second main survey topic was the attitude toward TH to detect a possible change in clinical practice in recent years with increasing evidence, expertise, and clinical experience with TH. Both the referring neonatologists and neonatologists in the cooling centers considered themselves more generous to treat neonates with HIE with TH over time (Fig. 4A). The consensus of optional free-text responses was that while TH was not performed in cases of clear contraindications, in questionable cases, there have been situations where a more generous approach led to the decision to proceed with TH, following a risk-benefit approach (low perceived risks of side effects of TH, potential benefit of neuroprotection).
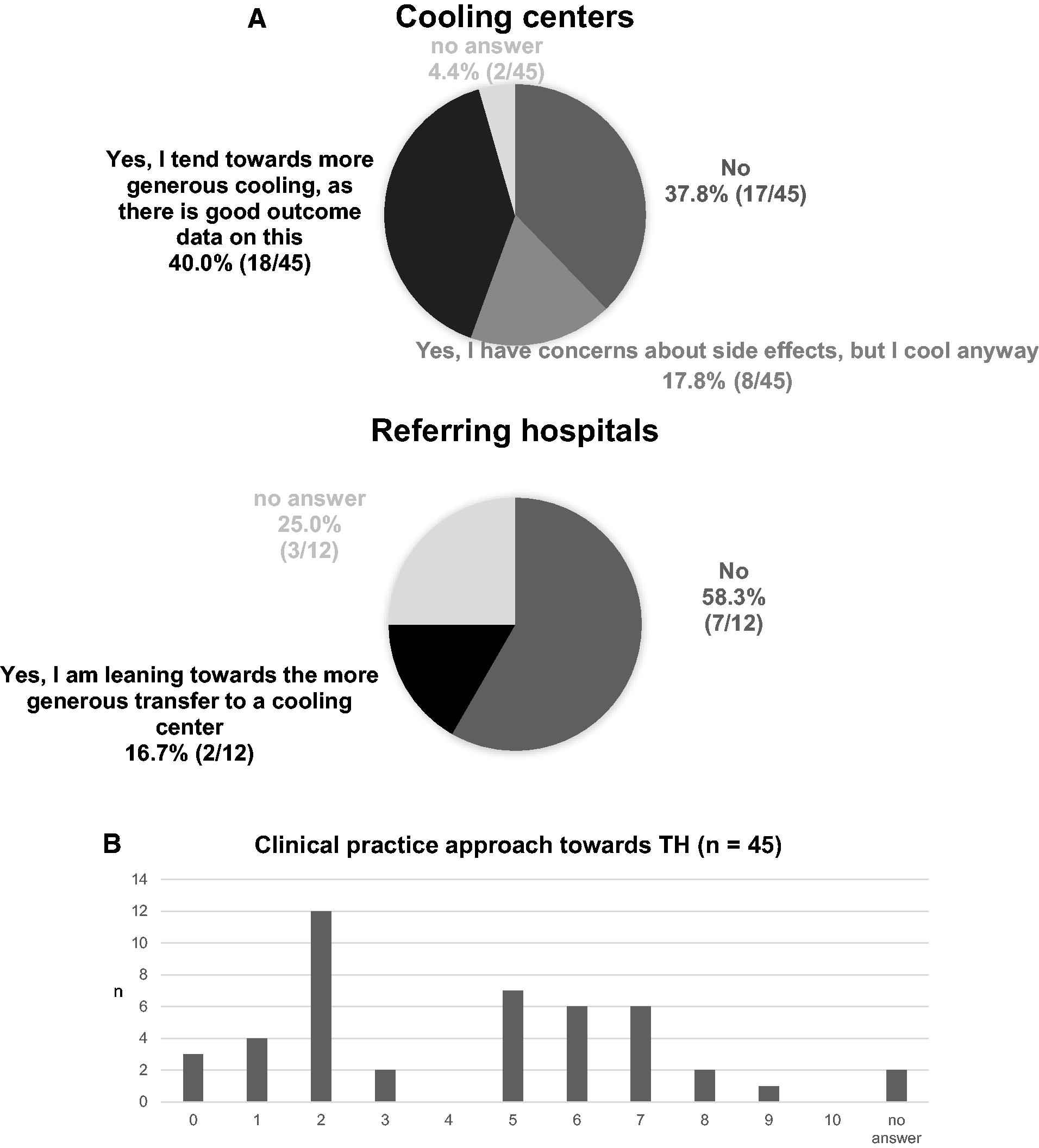
Attitudes towards TH and adherence to guidelines to initiate TH.
In the cooling centers, 46.7% (21/45) of the participants reported being up to date with the latest literature on HIE, similar to the referring neonatologists (5/9; 55.6%). They reported that their attitude toward TH was influenced by the literature: In the cooling centers, 71.1% (32/45) responded that they were more open to TH based on evidence in the literature, whereas 22.2% (10/45) did not change their attitude based on literature, and 1 person (1/45; 2.2%) was more critical regarding TH due to literature reports. There were two non-replies (2/45; 4.4%). At the referring hospitals, 58.3% (7/12) were more open-minded towards TH, 16.7% (2/12) did not change their opinion, and 3 (3/12; 25.0%) did not answer this question. Neonatologists in the cooling centers self-rated their clinical approach concerning inclusion for TH on a wide range from conservative with adherence to guidelines to progressive with nonadherence to guidelines (Fig. 4B).
Discussion
In this study, we compared patient characteristics in neonates with HIE receiving TH between 2011–2017 and 2018–2023 in the Canton of Zurich, Switzerland, to evaluate if there was any drift in clinical practice to include milder HIE cases for TH over time. Objective data from the Swiss National Asphyxia and Cooling Register were thus augmented by a survey among treating neonatologists to include subjective attitudes and perceptions regarding TH.
The ratio of neonates with HIE receiving normothermia and TH remained stable, and there was no difference in perinatal and neonatal demographics of cooled neonates over time. Inclusion criteria for TH of the Swiss National Asphyxia and Cooling protocol remained unchanged, and adherence to protocol was similar in both time periods.
Moderate to severe grading of encephalopathy with standardized, but partly investigator-dependent, clinical neurological examinations (Sarnat score [Sarnat and Sarnat, 1976] and/or Thompson score [Thompson et al., 1997] was one inclusion criteria for TH (B-criteria, Supplementary Appendix A1). Difficulties with objective clinical assessment of encephalopathy were reported in the survey, reflecting clinical practice. This uncertainty was potentially of clinical relevance since survey respondents perceived themselves as more generous in their decision-making for TH, particularly in neonatal cooling centers.
Recent studies showed that the majority of practicing neonatologists would treat a neonate with mild(er) HIE with TH after considering the individual case (Singla et al., 2022). In a global survey, a quarter of respondents stated that they would be happy to treat every neonate with mild HIE with TH (Singla et al., 2022). In the Netherlands, more neonates with mild HIE were treated with TH in recent years, with a shift from moderate to mild HIE, while the ratio of severe HIE remained stable (Parmentier et al., 2020). Possible reasons were more confidence gained through experience with TH and the absence of significant side effects of TH (Parmentier et al., 2020), which were also stated as reasons to consider off-protocol cooling by respondents of our survey.
As TH is currently the only evidence-based, effective neuroprotective therapy for neonates with moderate to severe HIE (Jacobs et al., 2013; Mathew et al., 2022), this might also be a reason why neonatologists were more likely to offer TH to neonates with milder HIE, framed as a “do something” approach (Parmentier et al., 2020). Being aware that there was no evidence to support TH in mild HIE (Kariholu et al., 2020), respondents assessed that their decisions to provide TH outside of national guidelines were generous, however driven by “good intentions” of possible neuroprotection. This inclination to provide TH more generously might be associated with the fact that active servo-controlled cooling has become standard of care and can be performed with less effort compared to passive cooling.
This urge for neuroprotection might be due to the growing awareness that mild HIE can result in neurodevelopmental impairment. Studies showed that neonates with mild HIE and no TH had significantly lower full-scale IQ, verbal, and performance IQ scores compared with a healthy control group, as well as motor and cognitive disabilities and impairments in memory (Conway et al., 2018; Murray et al., 2016). Gagne-Loranger et al. depicted that not-cooled neonates with initially mild HIE progressed to more severe encephalopathy and developed subsequent brain injury (Gagne-Loranger et al., 2016). However, according to preclinical data, providing TH to a non-hypoxic brain might also lead to brain injury (O’Brien et al., 2019; Wang et al., 2016).
This drift in clinical practice, according to survey results, in line with the internationally described loss of equipoise for TH in mild HIE, was not confirmed by the current cantonal analysis of Swiss National Asphyxia and Cooling Register data. The TH provided in adherence to the cooling protocol was overall 85% (Table 1). The remaining 15% of off-protocol cooling occurred in the absence of A-criteria in 38% (13/34) and of B-criteria in 35% (12/34) (Table 1). Especially the increasing trend in not fulfilling two A-criteria over the years (p = 0.067; Table 1) might indicate the willingness of neonatologists to provide TH more generously, acknowledging that comparatively objective criteria (pH, base excess, lactate, and APGAR scores) were not fulfilled. Inclusion of some cases of mild HIE, i.e., not fulfilling the B-criteria, for TH was expected. Unexpectedly, there were slightly less cases with mild HIE who received TH in the later period (p = 0.177; Table 1). However, there was a trend of more neonates graded with a Thompson score of 7 before cooling in the later time period, maybe reflecting the trend to offer TH to neonates with milder HIE in congruence with the survey results and the literature (van Oldenmark et al., 2025). Neonatologists may tend to assign the threshold Thompson score of 7 (or higher) more generously. This could imply that neonates who might objectively fall just below the threshold were given the necessary score to justify or indicate eligibility for TH, which would explain the discrepancy of survey results (in line with international trends) and stable rates of off-protocol cooling in the Canton of Zurich.
The question arose of how encephalopathy was graded and whether it was reliably reported. Clinical assessment of encephalopathy remains a key challenge. This was supported by the survey results since the feasibility of A-criteria was rated higher compared to B-criteria, i.e., severity of encephalopathy (Fig. 3). Grading the severity of encephalopathy is based on a structured clinical neurological examination (i.e., Sarnat [Sarnat and Sarnat, 1976] and/or Thompson [Thompson et al., 1997] score) and thus depends on the experience and knowledge of the examiner. A two-person independent assessment of Sarnat and/or Thompson score (Sarnat and Sarnat, 1976; Thompson et al., 1997) to meet consensus may enhance the accuracy of early identification and targeted interventions.
Of note, the referring neonatologists were quite sure that the guidelines were fully complied with, while the neonatologists in the cooling centers (who ultimately initiated TH) were not clearly of the same opinion. Compared to a previous national analysis, reported rates of off-protocol cooling were notably lower in the Canton of Zurich (2011–2017: 13%) compared to Switzerland overall (2011–2018: 21%) (Birkenmaier et al., 2023).
Many of the referring neonatologists and those working at cooling centers already considered aEEG findings in their assessments, possibly due to international training and knowledge of HIE guidelines including aEEG. Given its use in recent studies, the role of aEEG in guiding the decision to initiate TH for mild HIE, as well as its potential as a prognostic tool (Rao et al., 2022), could be discussed by the Swiss National Asphyxia and Cooling Register Committee. Adding an aEEG to the B-criteria and performing a two-person independent (ideally blinded) clinical assessment of encephalopathy may improve the decision-making process for TH.
The international drift in clinical practice to provide TH to cases of mild(er) HIE, outside of established guidelines and to varying degree, is concerning. Pending reports of randomized controlled trials on the efficacy and safety of TH in mild HIE will provide guidance and help to overcome uncertainties. Moreover, the objective identification of mild HIE remains challenging and will be of even higher importance if TH will continue to be indicated for moderate to severe HIE only.
Strengths and limitations
Important strengths of this multicenter study were the large sample size and prospective data collection for more than a decade, following the same Swiss National Asphyxia and Cooling protocol. Inclusion criteria for TH remained unchanged, except for including neonates ≥35 weeks gestational age as of 2015, compared to ≥36 weeks gestational age in 2011–2014. As for the limitations, one key issue was the potential selection bias since probably not all neonates with HIE receiving normothermia were entered into the Swiss National Asphyxia and Cooling Register. Furthermore, the Thompson score was not assessed in all neonates on admission, which limited the evaluation of the Thompson score over time. The survey benefitted from the high response rate of neonatologists directly involved in daily clinical practice at the bedside. The survey question on adherence to cooling protocol aimed at self-reporting own adherence. However, we cannot exclude that some respondents reported perceived general adherence.
Conclusions
Given that the topic of reassessing the threshold for application of TH in neonates with HIE is currently being investigated in many studies, these findings contributed to raising awareness in clinical practice and may contribute to potential adjustments in the Swiss National Asphyxia and Cooling protocol. The aim is to continue to provide evidence-based neuroprotection for neonates with HIE and counteract the drift in clinical practice toward TH until proven effective and safe in mild HIE.
Footnotes
Acknowledgments
Thank you to all neonatologists who participated in the survey. The authors would also like to thank the following data managers for entering data into the Swiss National Asphyxia and Cooling Register at the following hospitals: University Childrens’ Hospital Zurich, University Hospital Zurich, Cantonal Hospital Winterthur, Hospital Zollikerberg Zurich, City Hospital Zurich. Thank you very much to Verena Rathke for her work as register coordinator.
Authors’ Contributions
C.L., M.K., B.B., and B.G. made the conception of the study. C.L. was responsible for acquisition of data, data analysis and interpretation, search and review of literature, and drafting of article. C.L. and M.A. performed all statistical analyses of the study and interpreted results. B.G. and B.B. supervised the design of the study, data analysis and interpretation, search and review of literature, and critical review of the article. All authors critically revised the article and have read and approved the final article.
Ethics Approval and Consent to Participate
Data collection, evaluation, and publication for this study was approved by the Swiss ethical committee of the Canton of Zurich (KEK-ZH Number 2024-00714). Informed consent was obtained from all subjects. Informed consent was a prerequisite for obtaining ethics approval for this study.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Appendix A1
Supplementary Appendix A2
Supplementary Appendix A3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.