
Abstract
Background:
Acute suppurative thyroiditis (AST) resulting from a bacterial infection is an infrequent but potentially life-threatening endocrine emergency. Traditional management of this disease has been surgery in conjunction with targeted antibiotic therapy. Recent nonrandomized reports of small series have demonstrated good outcomes using less invasive approaches. No randomized clinical trials have been performed. Here, we provide a review of the literature and an approach to this problem based on expert opinion.
Methods:
The literature was reviewed utilizing PubMed, and a representative case of AST was presented to a panel of experts. Endocrinology, surgery, and infectious disease experts responded to a series of questions regarding diagnosis, management, prognosis, and harm.
Results:
Combining a broad spectrum of clinical expertise and the published literature, the authors suggest a clinical algorithm as a guide to management, addressing both diagnosis and acute and long-term management.
Conclusions:
Published studies indicate a trend toward less invasive management during active inflammation and infection and regarding definite therapy. Remaining questions are presented to foster an evidence-based approach to this disease. Ideally, future randomized, controlled trials will provide data to improve the therapy and outcome of AST.
Introduction
Traditional AST therapy has been surgery (partial or total thyroidectomy or surgical drainage) combined with targeted antibiotic therapy (15). Few published case reports suggest antibiotic therapy without surgical intervention (13). However, despite decades of reports describing surgical approaches as central to the clinical management of AST, more recent nonrandomized clinical practice appears to favor expectant management utilizing intravenous antibiotics without invasive surgery (16,17). Thus, diagnostic and treatment questions persist.
Here, we utilize a broad spectrum of clinical expertise and extensive review of the literature to explore the decision making process, generate a patient care algorithm, and encourage clinical trials and future reports on AST to provide answers to remaining diagnostic and management questions.
Methods
A representative case of AST was presented to a panel of experienced clinicians consisting of two thyroidologists, two endocrine surgeons, and one infectious disease specialist. The case details included data and therapeutic decisions obtained or made at the initial patient presentation. Discussants responded in writing to a series of questions on AST addressing diagnosis, management, prognosis, and harm. Once all responses were reviewed, an algorithm was constructed using their expert opinions and the published literature. The algorithm and supporting text were then refined by all authors.
Results
Acute evaluation and management
Initial evaluation
Most patients with bacterial AST present with anterior neck swelling, pain, and fever. Table 1 outlines the differential diagnosis of anterior neck swelling, fever, and pain and demonstrates a broad range of potential neck pathology. Table 2 illustrates predisposing mechanisms of infection, the identification of which may require specific therapy (18 –32). There is a wide spectrum of microbial pathogens reported in the immunocompetent and the immunocompromised host with AST. The suggested antibiotic therapy for each and their estimated incidence are shown in Table 3 (1,2,11,18,20,33 –59). A patient-focused approach based on clinical presentation with concurrent pathogen diagnosis and consideration of predisposing mechanisms is presented in Figures 1 –3.

Acute evaluation and management. Administration of IV iodinated radiocontrast will interfere with the ability to perform a thyroid radioactive uptake or scan for several weeks. CBC, comprehensive blood count; BUN, blood urea nitrogen; SCr, serum creatinine; TFT, thyroid function test; Tg, thyroglobulin and antithyroglobulin antibody; HIV, human immunodeficiency virus; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; CT, computed tomography; MRI, magnetic resonance imaging; GI, gastrointestinal.

Secondary evaluation and management.
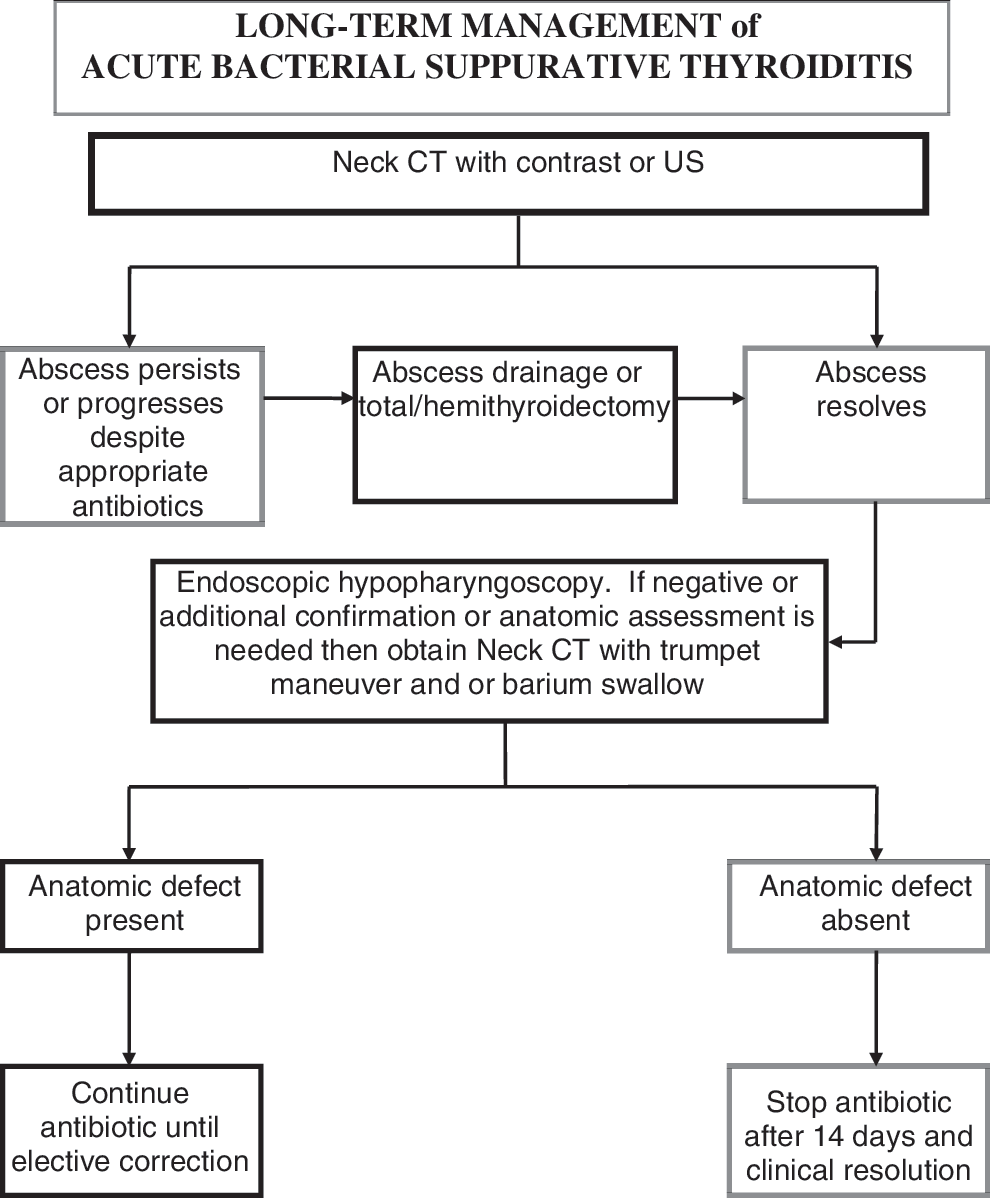
Long-term management.
In many cases, the route or source of infection is not obvious.
This table provides a suggested approach to antimicrobial therapy. It is not inclusive of all antibiotics effective for the listed pathogens. Local antimicrobial susceptibility patterns must be considered in antibiotic selection. Specific antibiotic therapy should be based on gram stain of aspirate/culture data; however, in view of the potential mortality associated with this disease, initial empiric antibiotic treatment pending culture data is recommended.
Initial therapy includes penicillinase-resistant penicillin and β-lactamase inhibitor.
Clindamycin is recommended if recent penicillin exposure or allergy.
See References (1,18,35). Frequencies may be inaccurate due to biased case reporting and testing methodologies.
In case of methicillin resistant S. aureus or penicillin intolerance.
For example, cefepime, ceftazadime.
For example, imipenem, meropenem.
If immunocompromised host, use in combination with penicillinase-resistant penicillin, β-lactamase inhibitor, and vancomycin for initial empiric therapy.
With suspicion of AST, timely stabilization of respiratory and cardiac function in a monitored setting is often necessary along with appropriate concurrent diagnostic assessment. The initial laboratory evaluation typically includes a complete blood count with differential and platelets; comprehensive metabolic panel to include serum electrolytes, blood urea nitrogen, creatinine, and liver function tests; serial thyroid function studies; serum thyroglobulin (Tg); erythrocyte sedimentation rate (ESR); C-reactive protein (CRP); urinalysis; urine and blood culture; and antibiotic sensitivity testing. Although there is a general consensus in the literature regarding baseline laboratory studies, there is disagreement regarding the utility of Tg measurement and inflammatory markers in the diagnosis of AST. Serum Tg is generally not a useful test in the evaluation of goiter. Moreover, the elevated value typically seen in AST does not contribute to the differential diagnosis other than identifying the thyroid as a site of inflammation or infection. Similarly, inflammatory markers such as ESR and CRP provide little specificity to the diagnosis of AST. Serial thyroid function studies are recommended, as there can be the release of thyroxine and triiodothyronine due to destruction of thyroid follicles with consequent thyrotoxicosis without hyperthyroidism (11,17,27,60 –65). Additional laboratory investigation may be appropriate based on clinical parameters and physical examination. Screening for human immunodeficiency virus (HIV) is prudent in all cases, as AST may occur in patients with preexisting thyroid disease or a compromised immune system, that is, HIV, transplant recipients, or those receiving chemotherapy (18,66 –68).
An important consideration in the initial evaluation is differentiating malignancy and subacute thyroiditis from AST (Table 1). Subacute thyroiditis is a relatively common entity associated with neck discomfort that can radiate outside the local cervical area. It may be associated with an increase in inflammatory markers such as white blood count (WBC), ESR, and CRP. During the painful stage, subacute thyroiditis is associated with clinical and biochemical thyrotoxicosis without hyperthyroidism. Thus, in the setting of thyrotoxicosis both subacute thyroiditis and AST demonstrate a very low radioactive iodine uptake of typically less than 1% as opposed to painful Graves' disease, which demonstrates an elevated radioactive iodine uptake (assuming the patient did not recently receive stable iodine such as intravenous computed tomography [CT] contrast). The most direct methods to differentiate between subacute thyroiditis and AST include thyroid ultrasound (US) and liberal fine-needle aspiration biopsy (FNA) targeting any mass and/or fluid collection. The thyroid sonogram should demonstrate an abscess in AST as opposed to diffuse heterogeneity and low intensity vascular flow in subacute thyroiditis. In subacute thyroiditis, the FNA usually shows evidence of multinucleated giant cell granulomas and mononuclear cell infiltration.
On rare occasions, thyroid cancers such as anaplastic or medullary thyroid cancer may grow rapidly and cause local infarction, necrosis, and thyroid tenderness mimicking AST or serve as a predisposing nidus for secondary infection (Tables 1 and 2). US and US-guided thyroid FNA (US-FNA) will usually be helpful in this differential diagnosis. In selected clinical circumstances (e.g., family history of medullary thyroid cancer), a serum calcitonin level and/or measurement of calcitonin in the thyroid aspirate needle washout may have utility.
Antibiotic selection
Concurrent with the timely diagnostic evaluation of AST, administration of broad spectrum empiric antibiotics and diagnostic reevaluation are important components of the management of this disease. Most patients present acutely with bacterial AST and chronologically require blood cultures, prompt empiric antibiotic treatment, and then timely culture of the suspected focus of infection (abscess or tissue sampling). A minority of patients present with a more indolent course that is more often associated with atypical organisms and are not the focus of this review. For hemodynamically stable patients, the identification of the responsible pathogen(s) prior to antibiotic initiation is a consideration; however, in view of the potential mortality of AST, prompt empiric antibiotic treatment of most patients before the culture results are known is preferred. The initial antibiotic regimen should be based on the patient's risk factors, medical history, severity of infection, antibiotic allergies, prevailing antimicrobial resistance patterns, and any recent antibiotic therapy. In an immunocompetent host that is able to tolerate penicillin, initial empiric therapy could include a penicillinase-resistant penicillin and β-lactamase inhibitor (e.g., piperacillin/tazobactem) and vancomycin if methicillin resistant Staphylococcus aureus is suspected. If a specific organism is identified, antibiotic selection can be more focused (Table 3). Therapy for patients with documented or suspected HIV infection requires consideration of opportunistic infections and initiation of a broader spectrum of antimicrobial therapy consistent with recommended treatment guidelines (50,55,69 –71). Subsequent antibiotic therapy should be adjusted to microbiology and antimicrobial susceptibility data.
Acute diagnostic imaging
Expedited CT imaging is informative in the evaluation of extrathyroidal (72) and intrathyroidal anatomy (73,74). CT with intravenous contrast of the neck and chest offers anatomic assessment of soft tissue enhancement, pyriform sinus fistula (16), and abscess including extension into the neck (including the retropharyngeal space) or mediastinum (59,75). While their embryological origin from ultimobranchial body or the third and/or fourth branchial arch congenital anomaly is debated (16,76), infections resulting from pyriform sinus fistulae are most often associated with left-sided neck abscesses (72) or intrathyroidal abscesses (17,77,78). However, it may be difficult to identify fistulae in the acute inflammatory period with either a CT and/or barium contrast study (16). While further investigation may be more diagnostic after resolution of the acute inflammatory phase, regardless of this, direct inspection by endoscopic hypopharyngoscopy may have the highest diagnostic yield (16). In most medical centers, CT is the preferred initial imaging modality in the acutely ill patient with suspected AST. US examination alone provides a less comprehensive view of the neck and upper mediastinum to identify potential extrathyroidal involvement. US and US-FNA biopsy are best utilized diagnostically and therapeutically if the CT reveals a thyroid mass or accessible fluid collection.
The relative diagnostic utility of magnetic resonance imaging (MRI) is unknown, as no studies have directly compared MRI, CT, or other imaging modalities in a comprehensive fashion. There are limited clinical data regarding whole body imaging with gallium (79), labeled white blood cells, or positron emission tomography/CT in AST. Likewise, radionuclide imaging with I123 or TC99m pertechnetate is unlikely to be helpful, as acute focal infection, inflammation, and thyroid malignancy are all associated with focally decreased uptake during euthyroidism, and all demonstrate diffusely decreased uptake during thyrotoxicosis in the absence of hyperthyroidism.
Secondary evaluation and management
US-FNA
Once the thyroid is established as the site of infection, US is the second imaging modality of choice in patients without airway compromise due to its ability to discriminate the internal anatomy of the gland and its associated opportunity for immediate diagnostic and therapeutic US-FNA. Urgent transcutaneous or open-surgical drainage is recommended for the patient with a compromised airway, whereas conservative diagnostic and therapeutic US-FNA drainage may be appropriate otherwise. Ilyin et al. recently reported two cases of AST treated nonsurgically utilizing US-FNA with a 21-gauge needle. US-FNA was performed on days 1 and 5 with oral and intrathyroidal administration of antibiotics without surgical intervention. There was no evidence of recurrence at the 6-month and 5-year follow-up (13). As this approach is limited in sample size and experience, studies that compare the outcome of this approach to a more traditional surgical drainage approach are needed.
US-FNA provides access to intra- and many extra-thyroidal abscesses for culture and antibiotic susceptibility testing and US monitoring of the response to antibiotic therapy. Bacteriologic and cytologic examination of US-FNA aspirates should be performed in all cases to identify the offending microbe(s) and exclude other thyroid pathology such as thyroid neoplasia that may play a causative role or masquerade as AST (80,81). The proposed clinical algorithm emphasizes that the patient's clinical status directs the urgency of intervention and the timeliness of definitive therapy.
Specific antibiotic therapy
As the patient's clinical status and microbiological susceptibility data become available, continuation of empiric antibiotic therapy or modification of the regimen may be necessary. The need to revisit the option for invasive treatment (in addition to antibiotic therapy) during active inflammation or infection should be guided by the presence or absence of an abscess, persistence of an abscess, or the recurrence of an abscess. Extrapolating from the larger experience with head and neck infections such as peritonsillar abscess (82), areas of suppuration (defined by imaging and US-FNA) do not necessarily mandate immediate surgery. Although large data series are absent, Lethert et al. successfully treated a case of AST with antibiotics without surgical intervention, but there was no abscess identified on CT imaging (57). Conversely, Ilyin et al. successfully treated AST with antibiotic therapy using frequent US-FNA and clinical surveillance of abscesses (13). Therefore, small areas of abscess may be successfully treated with antibiotic therapy supplemented with FNA without the need for open surgical drainage. Additional clinical outcome data are necessary to justify this approach in the majority of cases.
Long-term management
The long-term management of AST primarily focuses on antibiotic therapy and the need for invasive surgery or ablation of a predisposing anatomic defect.
Abscess persists or progresses
CT or US are valuable to delineate the persistence or resolution of the thyroid abscess (Fig. 2). Clinical deterioration, abscess persistence (>2 US-FNAs without improvement of the abscess), or abscess progression should direct therapy to drainage (large bore needle or open surgical drainage) or, if extensive disease is present, total, near total, or hemi-thyroidectomy (20,22,25,26,45,60,83). Open surgical drainage entails the placement of small passive drains that are advanced out over the course of several days and are intended to prevent seroma or continued abscess formation. Complications of abscess extension or rupture include tracheal or esophageal perforation, secondary involvement of the deep spaces of the neck, and descending necrotizing mediastinitis and septicemia (25,59,84).
Consideration of thyroidectomy should include assessment of the potential risks of surgery in a region of inflammation and the associated difficulty identifying normal tissue planes, which complicates the identification of the recurrent and superior laryngeal nerves and the parathyroid glands. Thyroid resection may be appropriate for diffuse, infiltrative processes characterized by multiple, poorly defined, and less discrete abscesses that persist or progress despite appropriate antibiotics (71,85). Patients with local or systemic symptoms and signs that do not respond to abscess drainage and antibiotic therapy should typically undergo thyroid resection (26,27,86). Resection is necessary when there are significant amounts of infarcted thyroid tissue or suspicion of thyroid malignancy (12,38,71). The completeness of the surgical resection may be significantly compromised by the inflammatory process. Thus, when possible, abscess drainage followed by elective resection after the acute inflammatory process has resolved may be a safer approach and, in the setting of cancer, a more oncologically sound choice.
Pyriform sinus fistula
If a pyriform sinus fistula is present, surgical resection or nonsurgical obliteration of the fistula reduces the chance of recurrent infection (16,17,29,87,88). Without intervention, further episodes of AST may be inevitable within months to several years (16,17,67,77,87,89). Transnasal flexible fiberoptic laryngoscopy (including hypopharyngoscopy of the left pyriform fossa apex) has become increasingly useful to identify the internal opening of a pyriform sinus tract and appears to be a more sensitive diagnostic test compared with CT and barium esophagography (16,77,90). Using this procedure, one may perform endoscopic cauterization of the pyriform sinus internal opening during the acute infection only if incision and drainage of the abscess are concomitantly performed (17,72). Otherwise, endoscopic cauterization can be performed after resolution of the acute infection. The substitution of US-FNA abscess drainage in place of incision and drainage in the setting of acute infection and endoscopic cauterization has not been reported. Airway compromise from laryngeal or pharyngeal involvement can be appreciated during transnasal flexible fiberoptic laryngoscopy and is suggested by dysphonia (66).
Kim et al. reported that the piriform sinus tract was identified in the acute setting with barium esophagography, CT, and direct endoscopy in 50%, 80%, and 100%, respectively (16). CT scanning with the use of an air contrast “trumpet maneuver,” where the patient holds a needle attached to a syringe between the lips and inflates a syringe simulating a trumpet, enhances visualization of a pyriform sinus fistula. However, it may be difficult to identify fistulae in the acute inflammatory period with either a CT and/or barium contrast study (16,76). Thus, if anatomic imaging is needed to identify or clarify an anatomic defect, it is best done after resolution of the acute infection. In a report of patients from ages 2–54 years, barium esophagography demonstrated 75% of fistula in the inflammatory period and 100% in the recovery period, yet it did not define the accurate anatomic pathway and the relationship of the fistulae to the thyroid. CT scanning using the trumpet maneuver identified and clarified the exact anatomic pathway of the fistulae in relationship to the thyroid in 30% of patients with fistulae during the acute inflammatory period and in 83% of patients in the recovery period (76). Most recently, Miyauchi et al. reported that during remission, barium swallow demonstrated the presence of a pyriform sinus in 100% of patients, whereas the CT scan with trumpet maneuver did so in only 68% of patients (17). Pyriform sinus fistulae have also been identified by US with or without the trumpet maneuver (75,91).
Elective resection or obliteration of the sinus tract is recommended after resolution of the thyroid abscess and clinical symptoms. Open surgery to excise a pyriform sinus tract may be effective but can be complicated by injury to the recurrent laryngeal nerve and other structures (16,17). Delaying open surgery until resolution of inflammation improves identification of vital structures in the neck, thereby reducing potential surgical complications (62). The recent use of endoscopic chemocauterization (ECC) with silver nitrate, 20–40% trichloroacetic acid (TCA), fibrin, or electrical cauterization has proved successful in small patient series and with lower risk of complications (16,17,72,77,90,92 –94). ECC allows closure of the internal opening of the sinus tract and probably eliminates the need for future surgical excision of the fistula (16,17,77). Most recently, Miyauchi et al. (17) achieved complete obliteration of the fistula without AST recurrence in 10 of 12 patients using ECC under general anesthesia with suspension laryngoscopy followed by intravenous antibiotics for 3 days. Oral intake is typically resumed 2–4 days postoperatively (16,17). This technique may not be feasible in all patients, and retention cysts may develop in some. Still, antibiotics combined with US-FNA draining of the abscess followed by ECC (if a fistula is present) after resolution of the acute inflammation may be an attractive alternative to more invasive approaches in many patients.
Long-term antibiotic therapy
Expert opinion regarding continued antibiotic therapy generally favors intravenous followed by oral therapy. In patients with a known pyriform sinus tract, continued antibiotic therapy until elective correction is reasonable. Conversely, antibiotic therapy is recommended for 14 days or until clinical resolution in patients without an anatomic defect. The schedule of antibiotics depends upon the clinical context, the organism(s), and the bioavailability of the antibiotic, as many have the same oral and parenteral bioavailability.
Conclusion
With effective antibiotic therapy and elimination of formed abscesses, patients with AST typically have an excellent prognosis if they survive the acute episode. However, it is difficult to determine the exact morbidity and mortality of AST due to its low incidence, underreporting of “typical” cases, and the presumed reticence to publish negative clinical outcomes. Thyroid function usually remains normal, although transient or permanent hypothyroidism or even thyrotoxicosis may occur as a result of the disease or treatment (7,27,61,67,95).
AST is an uncommon disease with few, if any, high-level evidence studies to clearly define the optimal diagnostic and therapeutic approaches. Currently, there is a trend toward identification of patients who may be best treated with less invasive strategies. A few medical centers (16,17,72) have demonstrated the ability to amass small cohorts of AST patients in relatively short time intervals. It seems possible that a motivated individual or professional organization could organize a well-designed multicenter study over a large geographic area to answer important questions such as (a) What approach or diagnostic sequence provides adequate accuracy and cost-effectiveness for the timely diagnosis of AST and the exclusion of illnesses requiring alternative therapy? Is this best accomplished with laryngoscopy, barium swallow, US, CT, or other imaging (such as MRI) alone; in combination; or in sequence? (b) What is the appropriate duration for antibiotic therapy in patients without an anatomic defect or in preparation for definitive correction of an identified defect? (c) Should therapy (antibiotics, drainage, chemocauterization, or surgery) and its timing be specified based on clinical parameters, the size of the abscess, microbiology, anatomic defect, or disease progression or persistence? (d) When US-FNA abscess drainage is used in place of open drainage, is there a benefit to direct instillation of antibiotics in addition to systemic antibiotics? Answers to these questions based on comparative clinical studies are needed to clarify the varying approaches described in the medical literature and to improve the cost-effective outcome of these challenging patients.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.