
Abstract
Background:
The vascular endothelial growth factor (VEGF) is a major promoter of endothelial growth and migration. Some studies have shown a correlation between expression of this growth factor and prognosis in several cancers, including well-differentiated thyroid cancer.
Aim:
We studied VEGF expression, local invasiveness, and other prognostic factors in papillary thyroid carcinoma (PTC) to test the hypothesis that the expression of VEGF is correlated with the degree of invasion of PTC.
Patients and Methods:
Clinical and pathological data of 76 patients with PTC were retrospectively reviewed. Group 1 consisted of patients with gross locally invasive tumors, group 2 consisted of patients with only invasion of the thyroid capsule, and group 3 consisted of patients with noninvasive PTC.
Results:
VEGF expression was noted within the tumor in all groups of PTC patients but was absent in the surrounding normal tissue. Older patients had higher expression of VEGF than younger patients. The age of patients with strong reaction to VEGF was 46 ± 14 (mean ± standard deviation), and that in patients with a weaker reaction was 39 ± 16 (p < 0.05). Only 20% of patients with a follicular variant of PTC had a strong reaction to VEGF compared with 68% of patients with classical PTC (p < 0.01).
Conclusions:
VEGF expression appears to be an early event in the development of PTC. Whether VEGF expression promotes the progression of PTC is not known, but the answer to this question may be important in view of its greater expression in older patients, a group whose prognosis in PTC is worse.
Introduction
Patients and Methods
This study was approved by the ethics review board of the Hospital das Clínicas of the University of São Paulo Medical School. We performed a retrospective review of all patients with locally invasive PTCs in whom complete clinical information was available and who were seen from 1986 to 2000. A similar number of patients with noninvasive PTCs were randomly selected for comparison if their clinical information was similarly available. This study did not include patients with poorly differentiated or undifferentiated tumors.
The data set included 30 patients with PTCs who had gross invasion of local structures (group 1), 18 patients with only invasion of the thyroid capsule (group 2), and 28 patients with PTC who did not have either gross invasion of local structures or invasion of the thyroid capsule (group 3). All patients were treated with total thyroidectomy and radioactive iodine postoperatively when residual disease in the neck was identified in the whole-body scan. Patients with regional neck metastasis were subjected to the appropriate neck dissection, ranging from central compartment to modified radical dissection. Locally invasive tumors were treated with shaving resection, achieving complete removal of macroscopic tumor. None of the patients required extensive surgery such as laryngectomy. Patients' age and sex, the size of the primary tumor, and its histological subtype were noted. In addition, information regarding tumor multicentricity, perineural and vascular invasion, regional metastasis, and recurrence of the disease was recorded.
Specimens were fixed in 10% neutral-buffered formalin and embedded in paraffin blocks. Four-micrometer sections were stained with hematoxylin and eosin for histological examination. All samples were fully examined by a single pathologist (I.V.C.). The World Health Organization classification of thyroid tumors was used (2004). PTCs were subclassified (14,15) into classical PTC, the follicular variant of PTC, and other variants of PTC.
Perineural invasion was detected only in cases with local invasion. We considered any site of vascular invasion within the tumor as a true vascular invasion, as it is not yet well defined where this invasion is important in papillary carcinomas, as it is in follicular carcinomas. PTC was considered to reoccur if new local, regional, or distant PTC was identified or there was a new rise in serum thyroglobulin.
A semiquantitative method (4,6,11,16) was used for VEGF determination. We considered not only the intensity of the reaction for each cell, but also the percentage of positive cells. The number of marked cells was 0 (no reaction), 1 (up to 10% reaction), 2 (11–50% reaction), and 3 (>50% reaction). The intensity of the reaction was graded as 1 (weak), 2 (medium), and 3 (strong). The final score was calculated by multiplying these two numbers, and the intensity score was expressed as null (0), weak (1 –3), moderate (4), or strong (6 –9). The antibody utilized was the polyclonal goat anti-VGF (Santa Cruz Biotechnology, Santa Cruz, CA) in a dilution 1:200. The positive control tissue was glioblastoma multiforme.
Fisher's exact test and the Pearson's chi-square test (17) were employed for statistical analysis. For the comparison of quantitative data variance analysis the Kruskal–Wallis test was employed (18). A p-value of 0.05 or less was considered indicative of a statistically significant difference.
Results
All PTCs had a positive reaction for VEGF (Table 1 and Fig. 1). Normal thyroid cells did not have a reaction for VEGF. Sometimes, the reaction for VEGF was observed in the cell membrane, but most commonly it was in the cytoplasm. The overall intensity of the reaction of VEGF was calculated as the product of the percentage of cells stained and the intensity of the reaction of positive cells. We observed that at least 28% of the tumors expressed a moderate reaction and up to 72% showed a strong staining, but the staining was similar in the three groups (p = 0.2143). There was a significant (p = 0.0452) positive correlation between VEGF expression and age (Table 2). In addition, there was significantly less VEGF staining (Table 2) in the follicular variant of PTC than in other histological types of PTC (p = 0.0041).
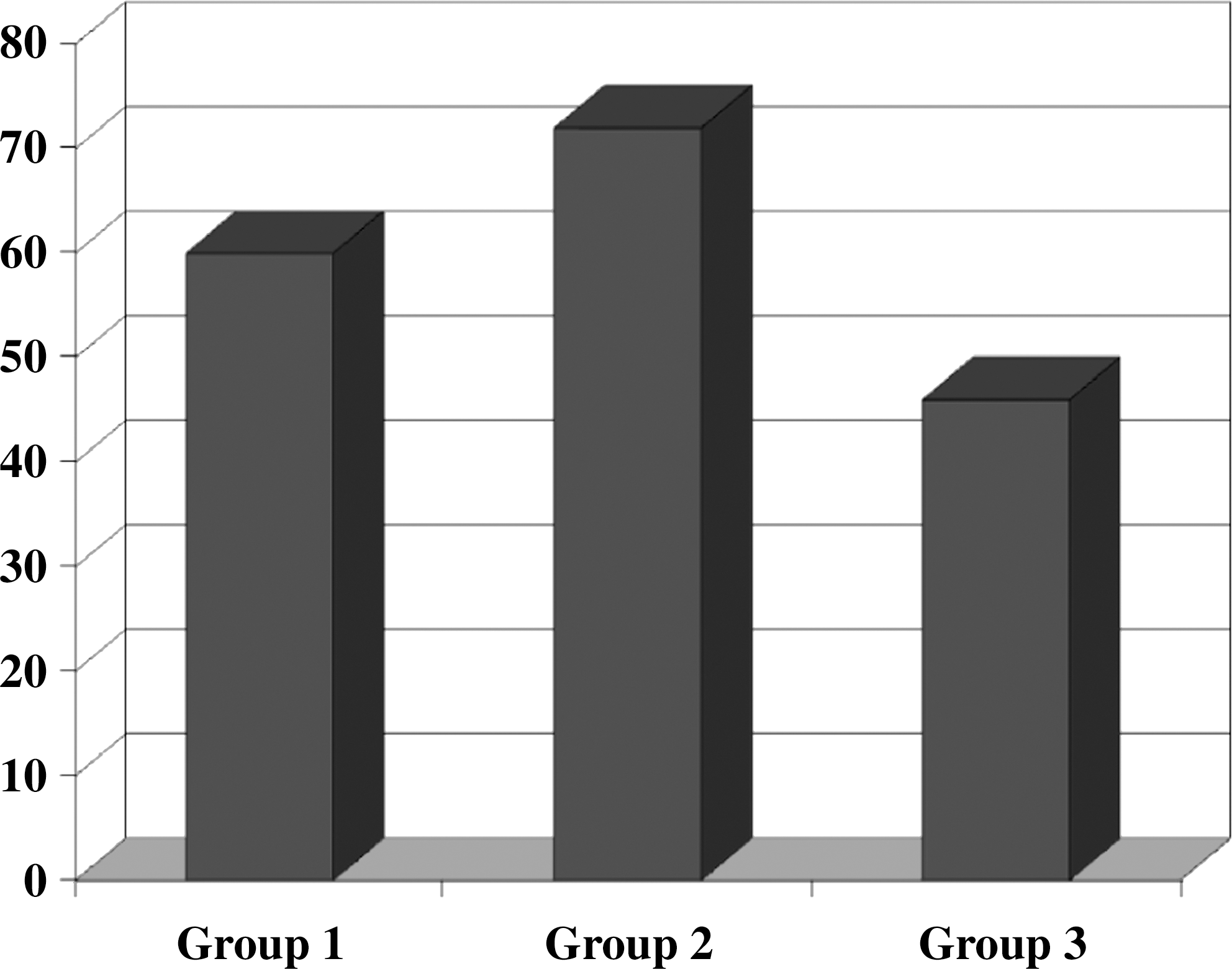
Percentage of patients with strong reaction to vascular endothelial growth factor in the three groups of patients with papillary thyroid carcinoma (PTC). Group 1, patients having gross invasion of local structures by PTC; group 2, patients having only invasion of the thyroid capsule by PTC; group 3, patients having no local invasion by PTC.
Definition of groups: group 1, patients having gross invasion of local structures by PTC; group 2, patients having only invasion of the thyroid capsule by PTC; group 3, patients having no local invasion by PTC.
PTC, papillary thyroid carcinoma.
Data were not available for all patients.
Mean follow-up time was 30 months.
Discussion
VEGF is one of the most important known factors that promote angiogenesis. It may be produced by many cells, but its receptor is almost exclusively confined to endothelial cells. It is highly active in the embryo but appears to have much less of a role or expression in the adult. VEGF is a glycoprotein that exists as at least five isoforms of varying size. In addition to cancer, its expression may be greater in hypoxia, in the presence of high concentrations of nitric oxide, and in activation of the oncogenes RAS and BRAF (1,13,19 –26).
VEGF expression has been studied in many different malignancies. A relative increase in its expression is associated with a worse prognosis in cancers of the esophagus, nasopharynx, and other head and neck sites (4,10 –12,27 –32), but this has not been noted in all studies (6).
In this study we noted that all PTCs exhibited a positive reaction to the VEGF. In contrast, there was no VEGF staining in the normal thyroid tissue around the tumors. The lack of VEGF expression in normal tissue is in agreement with other reports (5,27,36). In previous studies of thyroid tumors, higher expression of VEGF has been associated with a higher rate of mitotic activity and metastatic disease. Although we did not observe VEGF staining in normal tissue, VEGF expression has been noted in thyroiditis, nodular goiter, Graves' disease, and benign tumors (3,4,10,11,33 –36). Thus, though there appears to be a rationale for trials of VEGF inhibitors in PTC (19 –23), perhaps more so in older patients as they have greater VEGF expression, the exact importance of VEGF expression as a facilitator of tumor progression needs to be determined.
No difference in VEGF expression was noted among the three groups, in disagreement with another study (13). This might be consistent with a role for VEGF in the early phases of thyroid carcinogenesis. Jo et al. (13) found a significant correlation between VEGF expression and the size of the tumor or the presence of local invasion. Maybe the difference between our results and those of Jo et al. (13) relate to the larger number, namely, 162, of patients in their study. The patients studied by Jo et al. (13) were somewhat different from ours, perhaps explaining the differing results. Their number of follicular type of PTC cases was less then ours. Their method of measuring VEGF expression was also different from ours. They used four scores, from 0 (no staining) to 3 (moderate staining in most cells). We used more scores based on the intensity of the reaction in individual cells and the percentage of positive cells. They also used a different range of tumor sizes and did not provide information regarding the magnitude of the extrathyroidal invasion.
We did not find significantly greater expression of VEGF with many of the factors that have a poorer prognosis in PTC (Table 2). Unlike other studies (4,6,10,11, 27,39,40,41), we observed no correlation of VEGF expression with tumor size or the presence of metastatic disease. There was a clear relationship, however, between older patients and higher expression of VEGF. Seventy-two percent of the patients older than 45 years had a strong reaction to VEGF compared to 49% of the patients younger than 45 years. This was also noted in other studies (37,38). We also noted lower expression of VEGF in follicular variant of PTC compared to the classical PTC and less common frequent subtypes.
In conclusion, in the present series high expression of VEGF was very frequently noted in PTC. The fact that its expression was not positively correlated with more advanced disease does not rule out a role for the angiogenic factor VEGF in the initiation of thyroid carcinogenesis, but suggests, if such a role exists, that it is operative at a relatively early clinical, though not necessarily an early fundamental, stage. We hypothesize an important role for VEGF in thyroid carcinogenesis, as do others (6,42).
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.