
Abstract
Background:
Recurrence of regional cervical lymph nodes in patients with papillary thyroid carcinoma (PTC) is not uncommon, and is an important factor affecting the quality of life. The aims of this study are to investigate the risk factors that are associated with regional lymph node recurrence by comparing a group of patients with regional lymph node recurrence with a group without lymph node recurrence, and to analyze the clinical characteristics of recurrent regional lymph nodes in PTC.
Methods:
A retrospective analysis was performed on 189 patients who underwent surgery for PTC. By comparing a group with recurrent cervical lymph nodes (n = 33) with a group without recurrent cervical lymph nodes (n = 156), the risk factors for cervical lymph node recurrence were investigated and the clinical characteristics of recurrent cervical lymph nodes were analyzed.
Results:
Tumor size >2 cm, presence of extrathyroid tumor spread, high T stage, and presence of lymph node metastasis were associated with regional lymph node recurrence in univariate analysis (p < 0.05). Among them, only the N stage was significantly associated with regional recurrence in multivariate analysis (p < 0.05). The disease-free survival period was shorter in the lymph node metastasis–positive group, and the 10-year disease-free survival rate was 77.8% in the lymph node metastasis–negative group and 57.9% in the lymph node metastasis–positive group (p < 0.05). Among 130 patients without lymph node metastasis, regional recurrence occurred in 13 patients (10%), and the frequent levels of regional recurrence were levels II–IV of ipsilateral neck. In the patients with lymph node metastasis, the frequent levels were levels IV–VI of ipsilateral side and level II of the contralateral side.
Conclusion:
Considering the low incidence of regional lymph node recurrence and the levels with frequent regional recurrence in patients without lymph node metastasis, elective neck dissection in all cases of total thyroidectomy may be immoderate. However, if any risk factors for regional recurrence, including large tumor size, presence of extrathyroid spread, high T stage, and presence of lymph node metastasis, are detected by preoperative and intraoperative evaluation, a systematic compartment-oriented lymphadenectomy should be considered because of the high possibility of regional recurrence.
Introduction
Materials and Methods
A total of 215 patients who had PTC documented by histopathology and who had thyroid surgery between 1992 and 2003 were retrospectively analyzed. Among these patients, 26 patients were excluded due to insufficient medical records, short follow-up period (<2 years), and recurrence of primary tumor in the thyroid bed. Thus, a total of 189 patients were included in the study. Regional lymph node recurrence occurred in 33 (17.5%) of these patients. According to the presence of regional lymph node recurrence, the study population was divided into the regional lymph node recurrence group (n = 33) and no regional lymph node recurrence group (n = 156).
This study was presented to and approved by the local ethics committee, and the patients' approval and informed consent for review of their images and records were given by all the patients.
Surgical treatment and adjuvant therapy
Hemithyroidectomy was performed on 11 patients, and total thyroidectomy was performed on the remaining 178 patients. Hemithyroidectomy was chosen for those patients with single micropapillary carcinoma without nodal metastasis or extrathyroid spread. Total thyroidectomy followed by adjuvant therapies such as radioactive iodine (RAI) ablation therapy and thyroid hormone suppression therapy were performed on the remaining patients.
Among the patients who underwent total thyroidectomy, central neck dissection (CND) was performed on the patients who were intraoperatively suspected to have metastatic lymph nodes at level VI and were proven to have lymph node metastases in the lateral neck by preoperative ultrasound-guided fine-needle aspiration and intraoperative frozen biopsy. Lateral neck dissection (LND) was performed in the patients with lymph node metastases in the lateral neck.
Follow-up
The mean follow-up period was 81 ± 44 months (± standard deviation; range, 48–386 months). The patients who underwent hemithyroidectomy were followed with serial serum thyroglobulin (Tg) levels and ultrasonography after thyroid surgery. The remaining patients who underwent total thyroidectomy and RAI ablation therapy were followed up with serial serum Tg levels with or without thyroid hormone suppression of thyroid-stimulating hormone, whole-body RAI scans, and ultrasonography every 3–6 months. The criteria defined as regional recurrence comprise all of the following: clinical evidence of tumor, imaging evidence of tumor (uptake on whole-body scan or positive finding on ultrasonography), and increase of serial serum Tg levels with or without thyroid hormone suppression. In all cases that were suspicious for regional recurrence, computed tomography imaging and preoperative ultrasound-guided fine-needle aspiration were performed to define the location and pathology of recurrent lymph node.
Statistics
The following data were collected: sex, age, tumor size, multiplicity of primary tumor, extrathyroid spread, T stage, N stage, AJCC stage, AMES system, MACIS system, treatment modality, and location of regional recurrence.*
The association between regional recurrence and various clinical factors was examined using the Pearson χ 2-test, Fisher's exact test, or independent t-test as appropriate. Unconditioned logistic regression was used for the multivariate analysis of regional recurrence. Disease-free survival rates were estimated by the Kaplan–Meier method, and the different subgroups were compared using the log-rank test. The Cox proportional-hazards model was used for multivariate analysis. For all tests, a probability of <0.05 was accepted as statistically significant. All statistical analyses were done with SPSS software version 12.0 (SPSS, Chicago, IL).
Results
Patient risk factor
The age at diagnosis of the 151 female and 38 male patients ranged from 9 to 80 years (mean, 44.7 years). The mean age was 45.3 years for women and 42.6 years for men. Regional recurrence occurred in 27 (17.9%) of 151 female patients and 6 (15.8%) of 38 male patients, and there was no significant difference between the sexes (p > 0.05). Also, there was no significant difference between the “age less than 45 years” group and the “age 45 years and over” group (p > 0.05; Table 1).
Tumor risk factors and prognostic score system
Among the tumor risk factors, tumor size (smaller or larger than 2 cm), multiplicity of tumor, extrathyroid spread, T stage (T1-2 or T3-4), and N stage (with or without lymph node metastasis), larger size (>2 cm), presence of extrathyroid tumor spread, higher T stage, and presence of lymph node metastasis were associated with regional recurrence (p < 0.05; Table 2).
T stage, T1-2 versus T3-4; N stage, the presence of lymph node metastasis; N(–), no lymph node metastasis; N(+), lymph node metastasis.
There were no significant differences between the results of prognostic score systems (AJCC stage, AMES system, and MACIS system) and occurrence of regional lymph node recurrence (p > 0.05; Table 3).
Chi-square test.
Student's t-test.
AJCC, American Joint Committee on Cancer; AMES, patient age, presence of distant metastases, extent and size of primary tumor; MACIS, distant metastases, patient age, completeness of resection, local invasion, and tumor size.
Extent of surgical treatment
There were no regional recurrences in 11 patients who underwent hemithyroidectomy. Regional recurrence was found in 33 (18.5%) of 178 patients who had total thyroidectomy. However, the extent of thyroidectomy was not associated with regional recurrence.
CND and LND were performed in 84 patients and 49 patients, respectively. The incidence of regional recurrence was significantly higher in patients who underwent CND than LND (p < 0.05) (Table 4). Considering that multivariate analysis of the relationship between regional recurrence and type of neck dissection or N stage showed that only the N stage was statistically significant (p < 0.05), we believe that regional recurrence was more frequent in neck dissection groups, because neck dissection was mainly performed in patients with clinical evidence of lymph node metastasis (Table 5).
Fisher's exact test.
CND, central neck dissection, level VI; LND, lateral neck dissection, including levels II–V.
Multivariate analysis of clinical factors
Multivariate analysis of clinical factors, including sex, age, tumor size, T stage, N stage, and extrathyroid spread, showed that only the N stage was significant (p < 0.05), and lymph node metastasis increased the probability of regional recurrence by 3.474-fold (Table 6).
Age, <45 versus ≥45; tumor size, ≤2 cm versus >2 cm.
Disease-free survival
Univariate analysis showed that tumor size >2 cm, higher T stage, the presence of lymph node metastasis, and extrathyroid tumor spread were significantly associated with shorter disease-free survival period (p < 0.05) (Table 7). In multivariate analysis to confirm this relationship, patients with lymph node metastasis showed 3.138-fold shorter disease-free survival period (p < 0.05) (Table 7). The 10-year disease-free survival rate was 77.8% in the patients without lymph node metastasis and 57.9% in the patients with lymph node metastasis (p < 0.05) (Fig. 1).
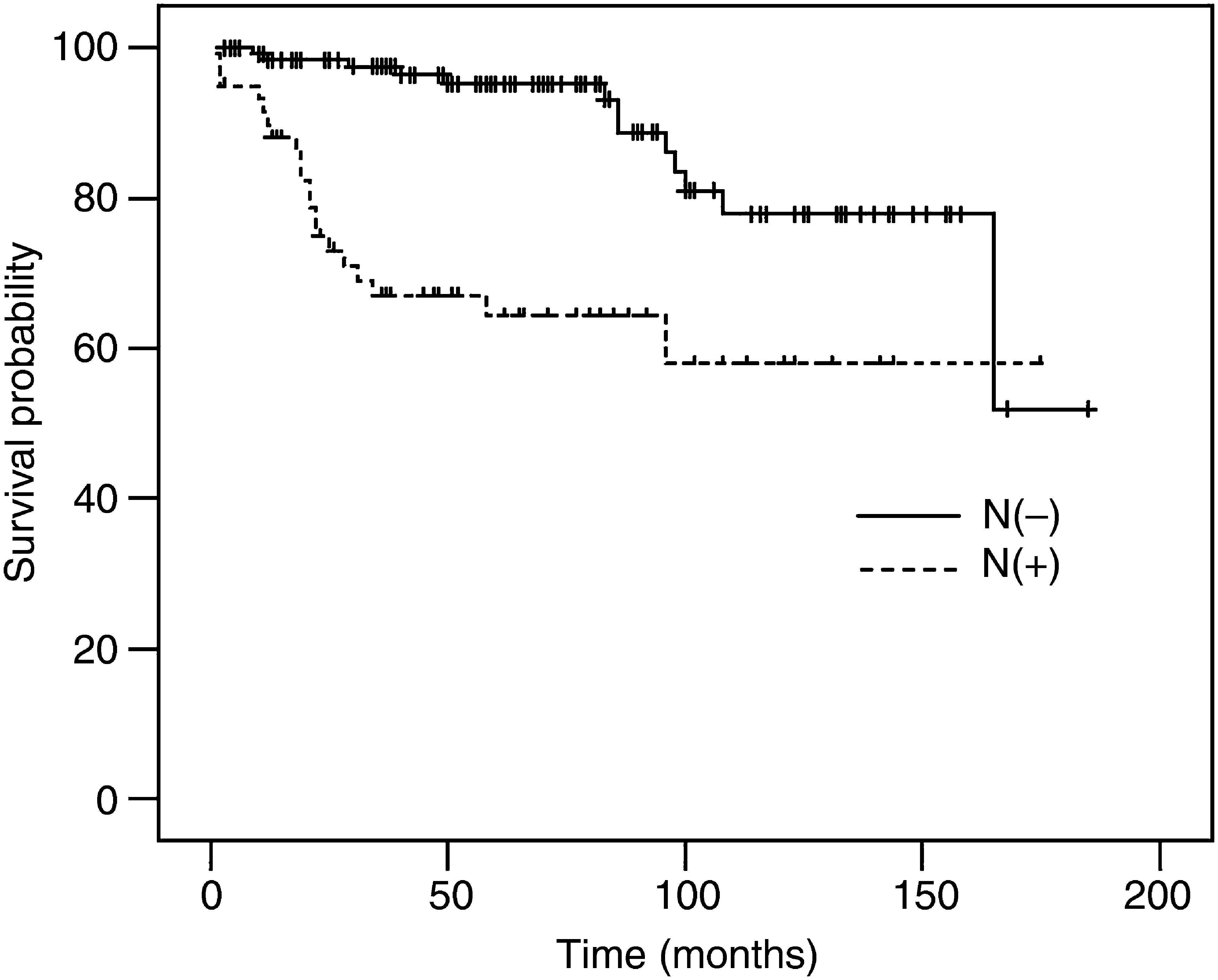
Disease-free survival curve according to the presence of lymph node metastasis. It shows a shorter disease-free survival period in patients with lymph node metastasis. N(−), no lymph node metastasis; N(+), lymph node metastasis.
HR, hazard ratio.
Clinical characteristics of lymph node recurrence
Among 130 patients without lymph node metastasis at the initial treatment, regional recurrence occurred in 13 patients (10%): 10 cases of ipsilateral neck recurrence, 1 case of contralateral neck recurrence, and 2 cases of bilateral neck recurrence. Regional recurrence was frequent in levels III, II, and IV of ipsilateral neck (Table 8). In 59 patients with lymph node metastasis at the initial treatment, 20 patients (33.9%) showed a regional recurrence. In these patients, there were 14 patients with ipsilateral regional recurrence and 10 patients with contralateral regional recurrence. In the ipsilateral regional recurrence group, metastatic lymph nodes were frequent in levels VI, III, and II at the initial treatment, and the frequent regions of recurrent lymph nodes were levels IV, VI, and V (Table 9). In contralateral regional recurrence group, the initial levels of metastatic lymph nodes were in levels VI and III, and recurrent lymph nodes occurred most frequently in level II (Table 10).
For treatment of regional recurrence, selective neck dissection (lymph nodes levels II–IV and VI) was performed in 18 cases, selective neck dissection (lymph nodes level I or II–V) in 12 cases, and lymph node excision in 3 cases. In all cases, RAI ablation therapy for adjuvant treatment was carried out and radiation therapy was performed in two cases. No patients with regional recurrence died of PTC, except for one patient who died of lung metastasis.
Discussion
The prognostic impact of prophylactic or therapeutic lymph node dissection in the patients with or without lymph node metastasis before surgery is controversial in PTC. Some authors suggest there is impaired survival in patients with PTC and lymph node metastasis at the time of initial surgery or lymph node recurrence after initial surgery (6,10), and others observed no decrease in survival rates (4,11,12). Even if there is controversy whether lymph node involvement at the time of initial surgery has any prognostic significance, recurrence in regional lymph nodes is not infrequent. Therefore, in terms of the quality of life, the recurrence of lymph node metastasis months to years after the initial thyroid surgery is an important clinical factor.
In the present study, univariate analysis showed that clinical risk factors such as tumor size, extrathyroid spread, T stage, and N stage at the time of presentation were associated with regional recurrence. This is in accordance with the results of previous studies (6,13 –15). Some authors suggest that large tumor size at presentation is associated with higher risk of regional recurrence (13 –15). In addition, it has been suggested that extrathyroid spread or higher T stage increases the rate of local recurrence and decreases survival rate, as well as increasing lymph node recurrence (6). However, in the present study, multivariate analysis demonstrated that only lymph node metastasis at presentation was associated with a significant difference in regional recurrence, and was the most predictable clinical factor for disease-free survival.
Although several groups reported up to 80% occult lymph node metastasis after prophylactic neck dissection (16 –18), the incidence of recurrent disease in patients without clinical evidence of lymph node metastasis is low (18). Therefore, some suggest that in the absence of evident clinical involvement of the regional lymph nodes, a compartment-oriented dissection should be performed limited to the region where metastases are frequently discovered, the central compartment (bilateral). In cases of clinically evident involvement of lymph nodes in the central and lateral compartment, systematic compartment-oriented lymphadenectomy should be performed (6,18). Similarly, among the patients who underwent total thyroidectomy, we performed CND in the patients who were intraoperatively suspected to have metastatic lymph node on level VI, and CND and LND in the patients who were proven to have lymph node metastases on lateral neck by preoperative ultrasound-guided fine-needle aspiration and intraoperative frozen biopsy. The incidence of regional recurrence in the patients without lymph node metastasis at initial treatment was 10%. Therefore, since the rate of lymph node recurrence in patients without lymph node metastasis is comparatively low, elective neck dissection would be immoderate. In addition, considering the level that regional recurrence occurred frequently, the relatively lower prevalence of central neck recurrence than in other levels suggest that elective CND in all patients with total thyroidectomy may be overtreatment. Therefore, we think that CND should be considered only in cases with intraoperatively suspicious lymph nodes in level VI.
However, since the patients undergoing therapeutic neck dissection for clinically evident lymph node metastasis tend to have more advanced disease, the possibility of lymph node recurrence can increase. Therefore, in our study, the reason for the high prevalence of lymph node recurrence in cases in which neck dissection was performed is likely related to their N stage before initial treatment, an explanation supported by other studies (19,20).
In the present study, the prevalences of temporary and permanent hypocalcemia were 16.9% and 3.9%, and the prevalences of temporary and permanent vocal cord paralysis were 4.5% and 1.7%, respectively. CND, including bilateral paratracheal lymph node resection, was the most important risk factor for the development of hypocalcemia and vocal cord paralysis after initial surgery. The other complications of LND were chyle fistula (1.6%), Horner's syndrome (1.1%), and shoulder impairment (4%). Shoulder impairment occurred especially in cases with extensive neck dissection including levels II–V. Considering that the prevalences of these complications were similar to previous studies (21,22), these may be inevitable consequences of neck dissection. Therefore, if these complications are unavoidable, it may be appropriate that neck dissection is performed only in PTC with a clinical evidence of lymph node metastasis.
Among the group with regional recurrence of lymph node metastases, in those without lymph node metastasis at the time of initial treatment, most recurrences occurred on the ipsilateral side of neck in relation to the primary tumor, especially in levels III, II, and IV. On the other hand, in patients with lymph node metastasis at the time of initial surgery, recurrent lymph node metastasis usually occurred in levels II, III, IV, and VI, and this recurrence was frequently found in levels IV, V, and VI on the ipsilateral side and level II on the contralateral side. In particular, patients with regional recurrence on the contralateral side had a tendency to have metastatic lymph nodes at level VI at the time of initial treatment.
The extent of neck treatment required for lymph node metastasis or recurrence in central and lateral neck is in dispute (23 –25). CND can be applied in all patients, or in patients with clinical evidence of lymph node metastasis as in the major guidelines, including the American Thyroid Association guideline and the National Comprehensive Cancer Network guideline (26,27). Also, there is an argument whether CND should be performed bilaterally or ipsilaterally (28). As for the indication for modified radical neck dissection (MRND), the major guidelines agree on performing therapeutic dissection only in patients with clinical evidence of lymph node metastasis, and other reports referred to the usefulness of prophylactic dissection (26,27,29). In case of regional recurrence, the extent of neck treatment may be decided according to neck dissection type at the time of initial surgery. Since extensive neck dissection at initial time may make it difficult to perform a compartmental neck dissection while sparing the morbidity, some authors reported the usefulness of sonographical localization for regional recurrence (25).
In the present study, MRND was performed in 49 patients at initial neck treatment, and in patients with regional recurrence, selective neck dissection in 18 cases, MRND in 12 cases, and simple excision in 3 cases according to severity of regional recurrence. Even if we could not come to any conclusions about the extent of neck treatment because of the small number of neck dissection cases, neck dissection including levels II–V and VI may be a favorable method for cases in which LND is necessary. In terms of neck treatment of regional recurrence, systematic compartment-oriented lymphadenectomy should be considered rather than simple excision of recurrent lymph nodes (node plucking).
Conclusion
Since the recurrence rate of cervical lymph node was only 10% in patients without lymph node metastasis at the time of initial surgery, elective neck dissection may be not always necessary. However, if any risk factors for regional recurrence, including large tumor size, the presence of extrathyroid spread, high T stage, and the presence of lymph node metastasis, are detected by preoperative and intraoperative evaluation, a systematic compartment-oriented lymphadenectomy and postoperative evaluation with serial serum Tg level and imaging methods (whole-body scan or ultrasonography) during follow-up should be considered because of the high possibility of regional recurrence.
Footnotes
Acknowledgments
The authors wish to thank Ms. Yoo-Kyung Choi for proofreading the study. This study was supported by Korea University Grant.
Disclosure Statement
The authors declare that no competing financial interests exist.