
Abstract
Background:
Dosimetry has been used to help identify when empiric dosages of 131-I treatment for suspected metastatic well-differentiated thyroid carcinoma (WDTC) may be increased or should be decreased, but dosimetry is complex, and easier approaches would be useful. The three objectives of this study were to assess the utility of the percent whole-body retention of 131-I at 48 hours (%WBR48hr) in identifying patients with WDTC in whom the therapeutic empiric prescribed activity of 131-I might be increased/decreased, to evaluate the thresholds proposed by Sisson et al. in 2003 for increasing or decreasing activity, and to determine the relationship between %WBR48hr and maximum tolerated activity (MTA).
Method:
A retrospective review was conducted of patients who had WDTC, total thyroidectomy, suspected metastatic disease, thyroid hormone withdrawal, and 131-I dosimetry. The %WBR48hr was determined based on the Benua-Leeper dosimetry protocol, and the four thresholds and recommendations of Sisson et al., 2003 for the use of %WBR48hr were evaluated relative to an empiric activity (EA) of 7.4 GBq of 131-I. A biexponential equation was determined from the %WBR48hr data.
Results:
Of 142 patients, 47 patients had a %WBR48hr of <9%, and all could have received more than the EA of 7.4 GBq with an average of 21.0 GBq (incremental range of 6.8–23.2 GBq). Ten patients had a %WBR48hr ≤ 5%, and all could have had their EA of 7.4 GBq safely increased by at least 250%. Conversely, if the %WBR48hr was >24.8%, then 7 of 14 of these patients would have exceeded the MTA by 0.37–3.18 GBq with an EA of 7.4 GBq. Finally, for patients with a %WBR48hr > 40%, five of six patients would have exceeded the MTA by 0.85–3.18 GBq. A biexponential regression equation is presented.
Conclusion:
We conclude that, with respect to the treatment of metastatic epithelial cell thyroid cancer, the %WBR48hr of 131-I helps identify those patients in whom the empiric therapeutic prescribed activity of 131-I may be increased or should be decreased so as not to exceed the MTA and that Sisson et al.'s thresholds published in 2003 are applicable. We favor a biexponential regression model using the %WBR48hr and a lower limit threshold as a potentially useful method for determining how much an empiric therapeutic prescribed activity of 131-I can be increased or decreased.
Introduction
Source: Sisson et al. (10).
The objectives of this study were [1] to assess the utility of the percent whole-body retention of 131-I at 48 hours (%WBR48hr) to identify patients in whom an empirically selected therapeutic activity of 131-I might be increased or should be decreased, [2] to evaluate the proposed threshold of Sisson et al. (10) for safely increasing or decreasing the prescribed activity of 131-I, and [3] to evaluate the relationship between %WBR48hr and maximum tolerated activity (MTA) to help provide a quantitative method to determine when and how much to either increase or decrease the empiric therapeutic prescribed activity of 131-I.
Materials and Methods
A retrospective review that was approved by our Institutional Review Board was conducted on patients who [1] had WDTC, [2] had a total or near-total thyroidectomy, [3] had 131-I whole-body dosimetry performed for the first time at the Washington Hospital Center between February 2000 and August 2005, [4] were suspected of having metastatic disease (e.g., by clinical exam, elevated serum thyroglobulin levels with negative antithyroglobulin antibodies, other imaging modalities, and/or histology), [5] underwent thyroid hormone withdrawal in preparation for radioiodine treatment, and [6] had adequately elevated thyroid-stimulating hormone (TSH) levels at the start of the dosimetry (e.g., >25 μIU/mL or if <25 μIU/mL, then <25 μIU/mL with 131-I uptake >5% in thyroid bed/lesion). Patients who had received recombinant human TSH injections in preparation for the 131-I dosimetry instead of thyroid hormone withdrawal were excluded. When available, the following patient characteristics were obtained: age, sex, height, weight, blood urea nitrogen (mg/dL), creatinine (mg/dL), free thyroxine (ng/dL), thyroglobulin (ng/mL), TSH (μIU/mL), uptake in thyroid bed/neck (%), and total lifetime prescribed activity of 131-I (mCi/MBq) administered for ablation/treatment.
Dosimetry
The dosimetry protocol employed at our facility is derived from the Benua-Leeper method (5) originally developed at the Memorial Sloan Kettering Cancer Center. Some minor modifications in the data collection have been incorporated: principally the elimination of the urine collection and the use of a dual gamma camera whole-body scanner in place of a scintillation probe to generate a geometric mean for the whole-body retention data. More details describing this procedure have been presented elsewhere (6), and the objective of the dosimetry is to calculate the MTA such that the radiation absorbed dose to the blood (bone marrow) would not exceed 200 rad (cGy). A prescribed activity of 2 mCi (74 MBq) of 131-I was administered orally for the dosimetry, usually in capsular form. Of note, this study reports the calculated MTA of 131-I, which does not necessarily represent the actual prescribed activity of 131-I that the patient received for treatment. The latter may have been less than the MTA for clinical reasons (e.g., low absolute neutrophil or platelet count, and/or results of bone marrow biopsy, time from previous treatment, and total accumulation dosage of 131-I), previous significant side effects (e.g., nausea vomiting and severe sialoadenitis), and/or patient desires. Also, to avoid confusion, the term “dose” will be used to refer to the radiation absorbed dose (rad or Gy), while the term “prescribed activity” will represent the amount of activity (mCi or MBq) administered.
Assessment of the thresholds of Sisson et al. (10)
Sisson et al. (10) reported two thresholds for the %WBR48hr for which the prescribed activity of 131-I might be increased (see Table 1). By applying these thresholds to our group of patients, we determined the number of patients in our group who could have received prescribed activities of 131-I larger than a standard empiric prescribed activity of 200 mCi (7.4 GBq) without exceeding the dose of 200 rad (cGy) to the blood. The absolute amounts of potential increases in the prescribed activities of 131-I over a 200 mCi (7.4 GBq) empiric prescribed activity of 131-I were recorded. For threshold three and four (Table 1), a similar determination was made, but in this case it involved a reduction in the empiric prescribed activity.
Percent whole-body retention at 48 hours of 131-I
The %WBR48hr was determined from the ratio of the geometric means of the whole-body dosimetry data at 48 hours postdosing to the measurement performed 1–2 hours postdosing before the patient voided. The anterior and posterior data were first corrected for background and possible changes in system sensitivity using an 131-I counting standard. The value at 48 hours was determined from a log-linear interpolation of the nearest time points. This “single-point-in-time” value was plotted relative to the dosimetrically determined MTA.
Statistical analyses
The various patients' characteristics, as well as the %WBR48hr, were statistically correlated with the MTA using the SAS/STAT software package. The correlations were investigated using both nonnormalized and normalized MTA for patient's body surface areas (BSA). The %WBR48hr data were modeled with a biexponential function using an iterative Levenberg-Marquardt algorithm.
This investigation was approved by the Institution Review Board of the MedStar Research Institute at Washington Hospital Center.
Results
During the evaluation period, dosimetry was performed for the first time in 142 patients who met the study inclusion criteria. The patient demographics are shown in Table 2.
TSH, thyroid-stimulating hormone; %WBR48hr, percent whole-body retention of 131-I at 48 hours; MTA, maximum tolerated activity.
Of the patients having a %WBR48hr < 9% (threshold 1), 100% (47/47) of the patients could have had their prescribed activity of 131-I increased without exceeding a radiation absorbed dose of 200 rad (cGy) to the blood. The potential increase in activity ranged from 183 to 626 mCi (6.8 to 23.2 GBq). Of the patients having a %WBR48hr < 5% (threshold 2), 100% (10/10) of patients could have had their prescribed activity of 131-I increased by at least 500 mCi (18.5 GBq).
Of the patients having a %WBR48hr > 24.8% (threshold 3), 50% (7/14) of patients would have exceeded 200 rad (cGy) to the blood, and not to have exceeded 200 rad (cGy) to the blood for the group of seven patients, the prescribed activity of 131-I would have had to been decreased by 10 to 86 mCi (0.37 to 3.18 GBq).
Of the patients having a %WBR48hr > 40% (threshold 4), 83% (5/6) of patients would have exceeded 200 rad (cGy) to the blood, and to not have exceeded 200 rad (cGy) to the blood for those five patients, the 131-I prescribed activity should have been decreased by 23 to 86 mCi (0.85 to 3.18 GBq). The one exception in this group was an obese male with a BMI of 53.2.
In regard to significant correlation of patient characteristics in Table 2 with MTA, no highly significant correlation was noted except for patient's weight and %WBR48hr with p-values of <0.005 and <0.0001, respectively. The patient's sex, height, and blood urea nitrogen level each just had a significant correlation of p < 0.05.
Once the MTA for each patient was normalized to the patient's BSA based on the Mosteller formula (11), there was no longer a statistical difference in MTA between the sexes (p < 0.945), the patient's height (p < 0.26), or weight (p < 0.10). As with the nonnormalized MTAs, none of the other parameters listed in Table 1 were significantly correlated with the normalized MTA with the exception of the %WBR48hr (p < 0.0001).
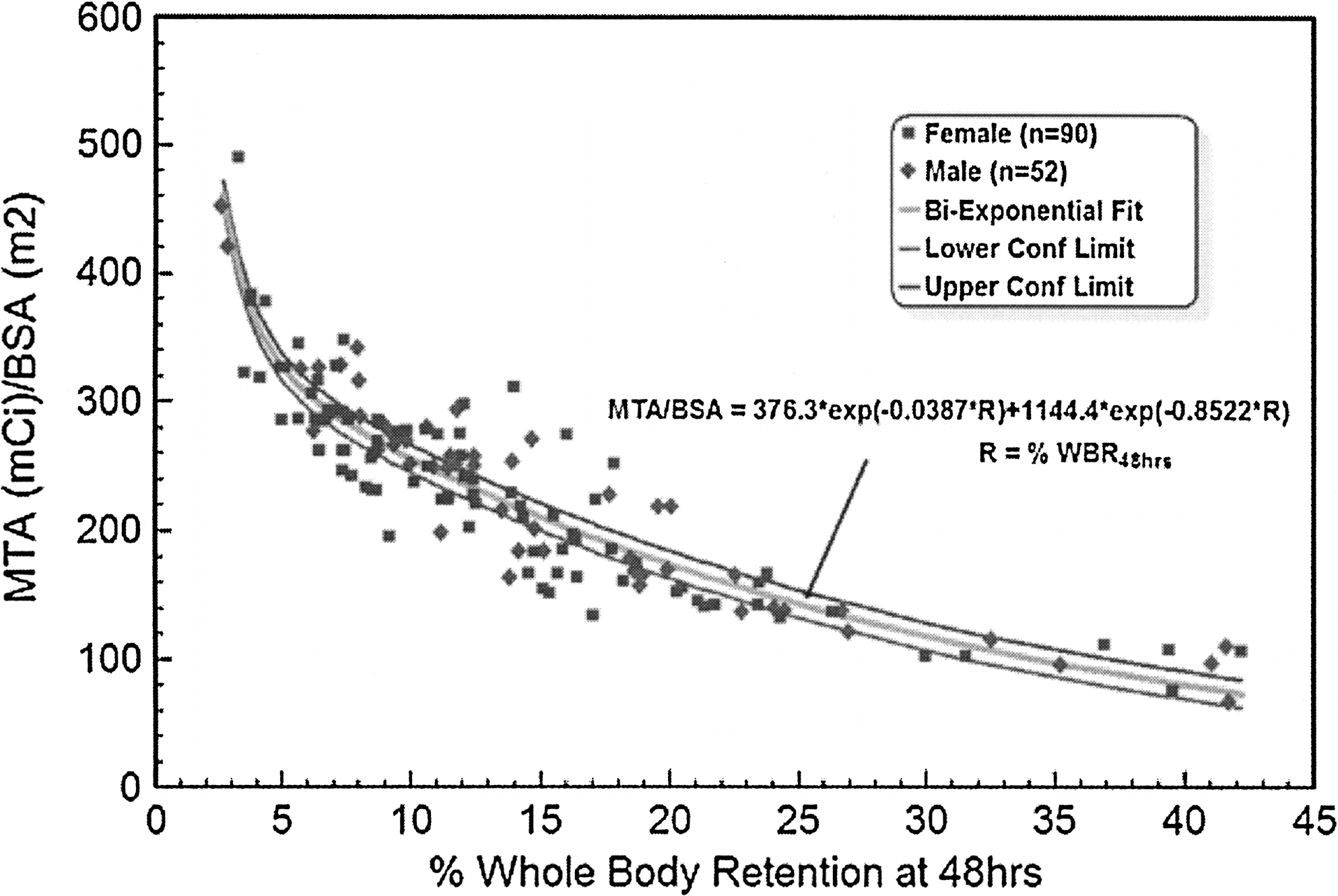
Because normalizing the MTA to the BSA resulted in a steeper upslope in the data when the clearance was more rapid, a biexponential function was used to model the MTABSA as a function of %WBR48hr. These data are shown in Figure 1 and are based on a nonlinear, least-squares iterative fit using the Levenberg-Marquardt algorithm. Figure 2 demonstrates the 95% upper and lower confidence limits about that biexponential fit. Although the biexponential function resulted in a good fit to the data (R = 0.92), the standard error in the amplitude of the second exponential was large. This is a result of the apparent, but expected, rapid rise in the MTA for very fast clearance (%WBR48hr < 4%) and the small number of patients (n = 6) in this range. The individual patient deviations are shown in Figure 3, which plots the deviation of the patient data from the biexponential regression model as a percentage of the predicted value. The average deviation was 0.55% over the entire range of clearance values. The standard deviation was ±14.3%.

Comparison of MTA versus %WBR48hr. Shown is the distribution of %WBR48hr for both male and female patients relative to the MTA normalized to the patient's BSA is demonstrated. The biexponential fit to the data is shown as a solid line. MTA, maximum tolerated activity; %WBR48hr, percent whole-body retention of 131-I at 48 hours; BSA, body surface area.
Upper and lower 95% confidence interval of the biexponential fit. Figure 2 is otherwise identical to Figure 1 with the exception of the inclusion of the 95% upper and lower confidence intervals for the biexponential model as indicated by the two dark lines. These represent the bounds within which we might reasonably expect the biexponential model to lie had the study been repeated with another group of patients.
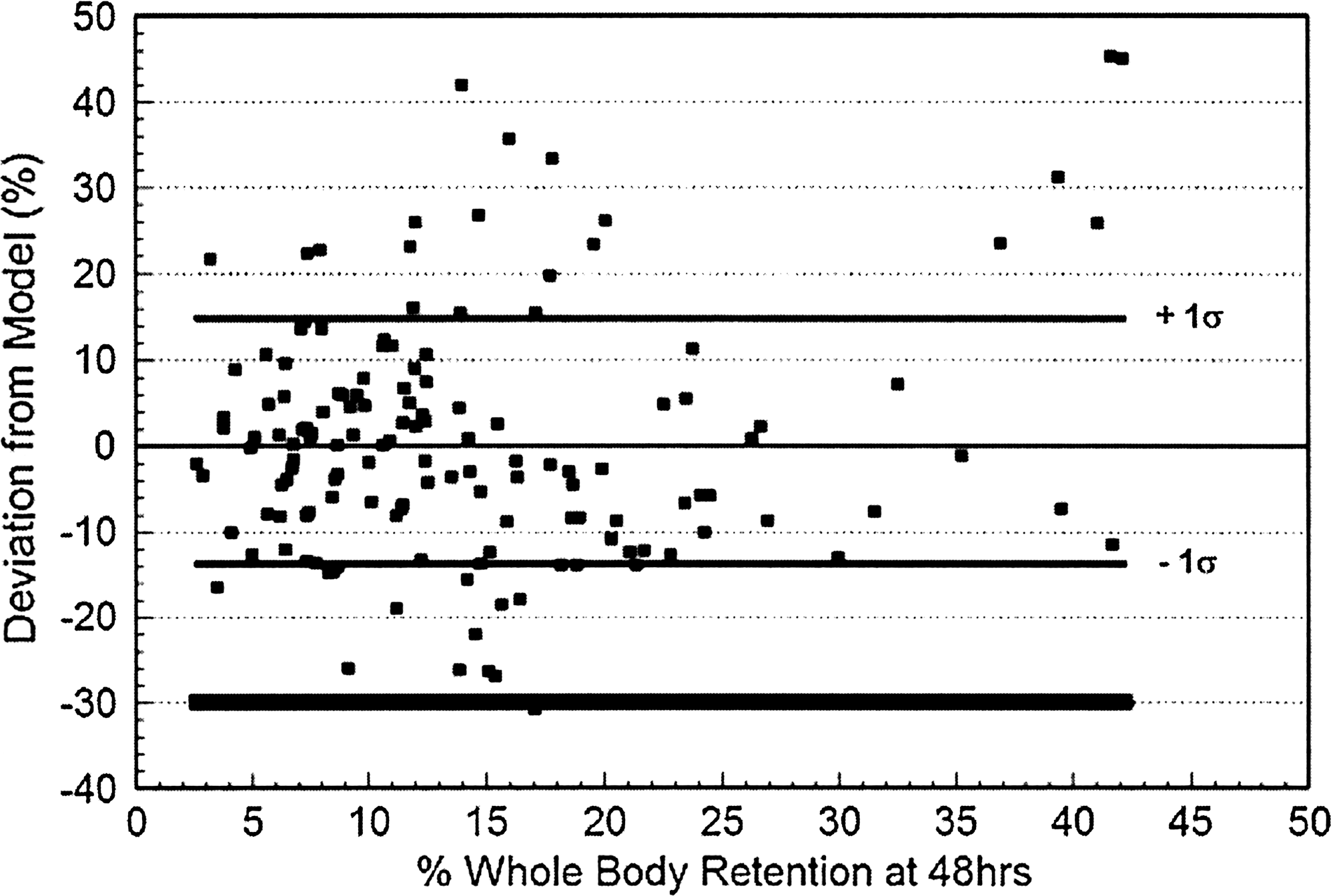
The individual patient deviations (percentage of predictive value). Figure 3 plots the deviation (i.e., difference) between the patient's MTA/BSA and the biexponential model–based prediction expressed as a percentage of the predicted value. Also shown are the ±1σ levels for this dataset. It can be seen that if the results of the model were used to determine the patient's treatment prescribed activity, then a number of patients (n = 6) would have exceeded their MTA by >20%. For reference purposes, a broad line located 30% below the model value demonstrates that all of the patients in this study lie at or above this level.
Discussion
As stated by Sisson (9), the objective of dosimetry is “… the potential of increasing the effectiveness of radioiodine treatments while preventing or limiting toxicity to normal tissues.” Given this objective, several whole-body dosimetric approaches have been proposed and implemented in clinical practice, which have been discussed in detail elsewhere (6). Unfortunately, the common dosimetry protocols are complex and require multiple return visits for the patient to evaluate the clearance of the radioiodine after a tracer administration. In the original article, Benua et al. (5) performed their whole-body dosimetry based on daily whole-body counts along with blood and urine samples for a data collection period as long as 8 days. Over time, most facilities simplified the procedure by eliminating urine collections and/or shortening the monitoring period to only 4–5 days (6,11,12). Nevertheless, even with these simplifications, dosimetry is still a lengthy and complex procedure. As a result, a limited number of facilities today perform whole-body dosimetry. In an attempt to further simplify the procedure, Thomas et al. (7) analyzed the whole-body retention and its relation to activity in the blood in 46 patients to determine whether the 131-I whole-body retention could be used as a predictor of the activity concentration in the blood, thereby eliminating the need for blood samples. At least in this group of patients they demonstrated good correlation between the blood dose estimates based on this external whole-body counting technique and those calculated by the Benua's original approach with agreement within ±10%. They concluded that a methodology based solely on the whole-body retention measurements provided a useful first-order approximation for hematopoietic dose estimates in adult patients. However, the results of another study did not agree with these findings. Robeson et al. (13) retrospectively analyzed 17 patients who had a dosimetry study performed. External whole-body counting correctly predicted the blood radiation absorbed dose in 35%, under-estimated it in 24%, and over estimated it in 41% dosimetries. Consequently, it was their conclusion that blood sampling remains an integral and necessary part of the dosimetry procedure. Sisson and Carey (8) also demonstrated two cases in which the relationship of whole-body clearance to blood clearance was not linear. On the basis of these patients they proposed that (1) a value of the relative whole-body retention at 48 hours >30% should be considered a warning of increased radiation to normal tissues, and (2) the maximum permissible activity based upon the percent 48-hour retention should be reduced to 50% if the patient is hyperthyroid, 60% if euthyroid, and 75% if mildly hypothyroid. In a later report, Sisson (9) further discussed the use of whole-body retention at 48-hour (%WBR48hr) such that a “… (%WBR48hr) below 10% would be an indication to increase their usual prescription if 131-I.” In a follow-up study, Sisson et al. (10) evaluated the %WBR48hr in a group of 87 patients. The mean fractional retention (±1SD) of 131-I at 2 days in the entire group was 0.165 + 0.087 with a range of 0.010–0.505. A range of 0.090–0.248 included 68% of the patients with 34% above and below the median of 0.152. The mean retention in females was almost identical to that in males. Based on these data, they proposed several recommendations by which this metric could be applied in clinical practice, and they are summarized in Table 1.
Our present study achieved several results. It validated the utility of the %WBR48hr in identifying patients whose therapeutic prescribed activity of radioiodine should be reduced or may be increased, it supported not good flow the thresholds of Sisson et al. (10) in Table 1, it demonstrated a significant negative correlation between the %WBR48hr and MTA. Finally, it defined a simple quantitative model by which the prescribed activity for a patient's therapeutic prescribed activity can be calculated based on the %WBR48hr and the patient's height and weight.
The biexponential equation adopted in this study, which incorporates normalization of the MTA to the BSA, offers a potential sex-independent method based simply on the patient's fractional retention of the administered 131-I at a single time point postadministration, namely, 48 hours. However, because of the deviation of the individual patient data from the model as reported in the results section, the patient's MTA may be overestimated by >15% in approximately 1 out of every 10 treatments. This would be unacceptable in clinical practice, and as a result, we propose that a conservative threshold needs to be applied to this model if it were to be used in place of a comprehensive dosimetry protocol. As shown in Figure 3, if a threshold is set at 70% of the predicted normalized MTA, then none of the patients in this study would have been treated with a prescribed activity that would have exceeded their MTA.
The present study has several limitations. First, this study does not assess long-term outcomes or side effects. This is almost always problematic with studies of patients with WDTC. Second, this study did not subdivide patients by various patient factors that have already been reported to increase the likelihood of exceeding 200 rad (cGy) to the blood (14 –16). These factors include advanced age as reported by Tuttle et al. (14) and Kulkarni et al. (15), as well as, functioning and nonfunctioning pulmonary metastases as reported by Esposito et al. (16). With more patients, the groups could be further refined, thereby offering potentially better reference groups that would be more specific for each patient's situation. Finally, this study did not include patients who were prepared with injections of rhTSH; thus, the data in this study may not be applicable to this patient population.
There are several potential benefits that can be derived from using the %WBR48hr. The %WBR48hr would save a significant amount of time not only for the patient but also for the physician and nuclear medicine staff. Equally as important, the %WBR48hr can be performed in almost any nuclear medicine facility since it does not require any specialized equipment or expertise. Perhaps, the most significant advantage is that this method offers the opportunity to use 123-I instead of 131-I to perform an estimate of the MTA when it would not be practical to perform a more comprehensive 4–5 day dosimetry protocol. Maxon et al. (17) and Mandel et al. (18) have demonstrated that imaging and, therefore, potentially quantitation can be performed with 123-I at 48 hours. Replacing 131-I with 123-I for the pretreatment diagnostic study and %WBR48hr would effectively eliminate the issue of potential stunning, at least to the extent that this phenomenon negatively impacts on a future 131-I therapy.
In adopting the use of the %WBR48hr, there are two final caveats. First, the original recommendations by Benua (5) that the actual WBR48hr should not exceed 120 mCi (4.44 GBq) when pulmonary metastases are not present and 80 mCi (2.96 GBq) when pulmonary metastases are present still apply. Second, although we believe that the determination of the %WBR48hr may represent an acceptable alternative method for those facilities that either will not or cannot perform a more comprehensive dosimetry protocol, it is paramount to remember that the %WBR48hr is just one measurement in time. Consequently, when one is trying to determine the prescribed activity for treatment of patients with metastatic WDTC, we still recommend as the preferred method and whenever possible a comprehensive whole-body and blood dosimetry protocol rather the %WBR48hr. A more comprehensive dosimetry protocol provides a potentially more accurate and clinically accepted estimate of the MTA based on a limit of 200 rad (cGy) to the blood and also the potential that a higher prescribed activity of 131-I might be administered, thereby potentially delivering a higher radiation absorbed dose to the metastases.
In summary, %WBR48hr is useful in identifying patients whose therapeutic prescribed activity of radioiodine should be reduced or may be increased, the thresholds based on Sisson et al. (10) in Table 1 are valid, and the application of the proposed %WBR48hr biexponential model with a 70% threshold should help determine how much the empiric therapeutic radioiodine prescribed activity may be increased or decreased. Finally, the %WBR48hr can be performed in almost any nuclear medicine facility.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.