
Abstract
Background:
To decrease the severity and frequency of radiation sialoadenitis, postponement of the use of sialagogues has been proposed for the first 24 hours after 131I treatment for well-differentiated thyroid cancer. One proposed mechanism is that sialagogues increased salivation and salivary blood flow resulting in greater radioiodine uptake in the salivary glands—a rebound effect. This case study demonstrates no rebound effect.
Methods:
A 33-year-old woman with well-differentiated thyroid cancer desired to know whether she would have a rebound effect if she used sialagogues during the 24-hour period after her 131I treatment. Salivary images of the parotid glands were initiated 2 hours after the administration of 131I for her whole body scan. Lemon juice was administered. Background corrected time–activity curves were obtained for both parotid glands. The potential reduction in radiation absorbed dose to the parotid glands secondary to the administration of lemon juice was calculated.
Results:
The time–activity curves demonstrated that the 131I in the right and left parotid glands decreased rapidly after lemon juice by 87% and 83%, respectively, with return to pre–lemon juice levels by 30 and 13 minutes in the right and left parotid glands, respectively. However, at no time during the 1 hour of imaging did the uptake in either parotid gland significantly exceed the pre–lemon juice levels of activity. The potential reduction of radiation absorbed dose to the parotid glands secondary to the use of lemon juice ranged from as much as 30% to 67%.
Conclusion:
This case study demonstrates 1) an approach to assess whether an individual patient will have increased or decreased radioiodine uptake in the salivary glands after administration of sialagogues without the administration of any additional radioiodine, 2) a decrease of radioiodine uptake in the salivary glands after lemon juice without a rebound effect, and 3) a potential reduction of radiation absorbed dose with administration of sialagogues.
Introduction
This report presents a case that demonstrates 1) an approach using the prescribed activity for the radioiodine whole body scan (WBS) to assess whether or not an individual patient will have increased or decreased radioiodine uptake in the salivary glands after administration of sialagogues, 2) a decrease of radioiodine uptake in the salivary glands after lemon juice without evidence of a rebound effect, and 3) a reduction of radiation absorbed dose after the use of sialagogues.
Case History
A 33-year-old woman was diagnosed with well-differentiated thyroid cancer. Total thyroidectomy disclosed a primary tumor measuring 2.5 cm with 14 of 14 lymph nodes positive for metastatic papillary thyroid carcinoma. Additional ultrasound and magnetic resonance imaging of the neck showed multiple enlarged lymph nodes in the right supraclavicular region as well as a right posterior paratracheal lymph node. Positron emission tomography performed with [18F]fluorodeoxygluocse (FDG) in combination with computed tomography demonstrated FDG activity in several lymph nodes in the right level 5 lymph node area. Fine-needle aspiration of a right supraclavicular node demonstrated papillary thyroid cancer. Additional surgery with a modified right neck dissection and resection of the paratracheal node was performed. Eight of 43 lymph nodes were positive for papillary thyroid cancer. Her only medications had been thyroxine and Cytomel® (King Pharmaceuticals, Inc., Bristol, TN). The patient's review of symptoms for possible salivary gland disease was negative. She had no prior history of salivary gland disease, smoking, alcohol use, previous radioiodine therapy, or external beam radiation therapy to the head or neck. There was no family history of salivary gland disease. Except for the healing scar from the recent thyroidectomy and modified neck resection, the patient's physical examination was unremarkable. Specifically, the salivary glands were normal with no swelling, masses, and/or tenderness. Her laboratory tests while taking liothyronine (LT3) including complete blood count (BC), comprehensive metabolic profile (MP), free thyroxine (FT4), total triiodothyronine (TT3), and thyrotropin (TSH) were all within the normal reference range. Because of the extensive loco-regional disease, the patient was referred by her endocrinologist for a 131I WBS and dosimetry in anticipation of radioiodine treatment.
As an intelligent and informed individual, the patient was aware of the report by Nakada et al. (3) as well as of the letter to the editor by Lam and van Isselt (4), and the patient desired to know whether or not she should take sialagogues within the first 24 hours or even within the first several hours after the administration of her treatment dosage of 131I. In order to attempt to 1) characterize the radiopharmacokinetics of radioiodine in her salivary glands after the administration of a sialagogue to assess whether or not to use sialagogues and 2) if sialagogues were to be used, determine the frequency for the use of sialagogues, a salivary gland scan using the diagnostic prescribed activity of the radioiodine for the diagnostic WBS and dosimetry was clinically ordered and performed with her full consent. This case was approved by the Washington Hospital Center Institutional Review Board for publication as a case study.
Salivary Gland Scintigraphy
Preparation
The patient discontinued her Levothyronine 5 weeks prior to administration of her diagnostic activity of 131I for her WBS, at which time she initiated treatment with LT3 25 μg twice daily by mouth. The latter was discontinued 2 weeks prior to administration of her diagnostic activity of 131I, and at the same time she initiated a low iodine diet. Two days prior to her administration of her diagnostic activity of 131I, her TSH was 109 mIU/mL and her thyroglobulin was 29 ng/mL with no detectable antithyroglobulin antibodies. The patient was NPO for 4 hours prior to the administration of her diagnostic activity of 131I. Iodine 131 was used because the patient was undergoing whole body dosimetry, the latter to help determine the maximum tolerated activity of 131I for treatment.
Imaging procedure
For the WBS and dosimetry, the patient was administered 67 MBq (1.8 mCi) of 131I orally in capsule form. Imaging of the salivary glands was initiated 2 hours after administration of the 131I with images acquired for 1-minute duration every minute for ∼60 minutes. Five minutes into the imaging, 5 mL of Real Lemon Juice® (Mott's, Inc., Stanford, CT) was administered orally through a tube into the patient's mouth over a period of less than 1 minute. After ∼60 minutes, an additional 5 mL of lemon juice was administered, and the lemon juice was repeated three times at approximately 15- to 20-minute intervals. Imaging was continued at 1-minute intervals for an additional ∼60 minutes. The head was carefully positioned to assure symmetry, and the patient was instructed not to move her head. Anterior views of the head, face, and neck were obtained to allow assessment of both parotid and submandibular glands. Images were obtained using a peak of 364 keV, 20% window, 64 × 64 computer matrix, and a high energy collimator on an Siemens single head E-cam model 04022 (Hoffman Estates, IL).
Image and computer analysis
Regions of interest (ROI) were placed over each parotid gland and background areas as noted in Fig. 1. The right and left background ROIs were normalized to and subtracted from the right and left parotid ROIs, respectively, and time–activity curves were obtained for the ∼2 hours.
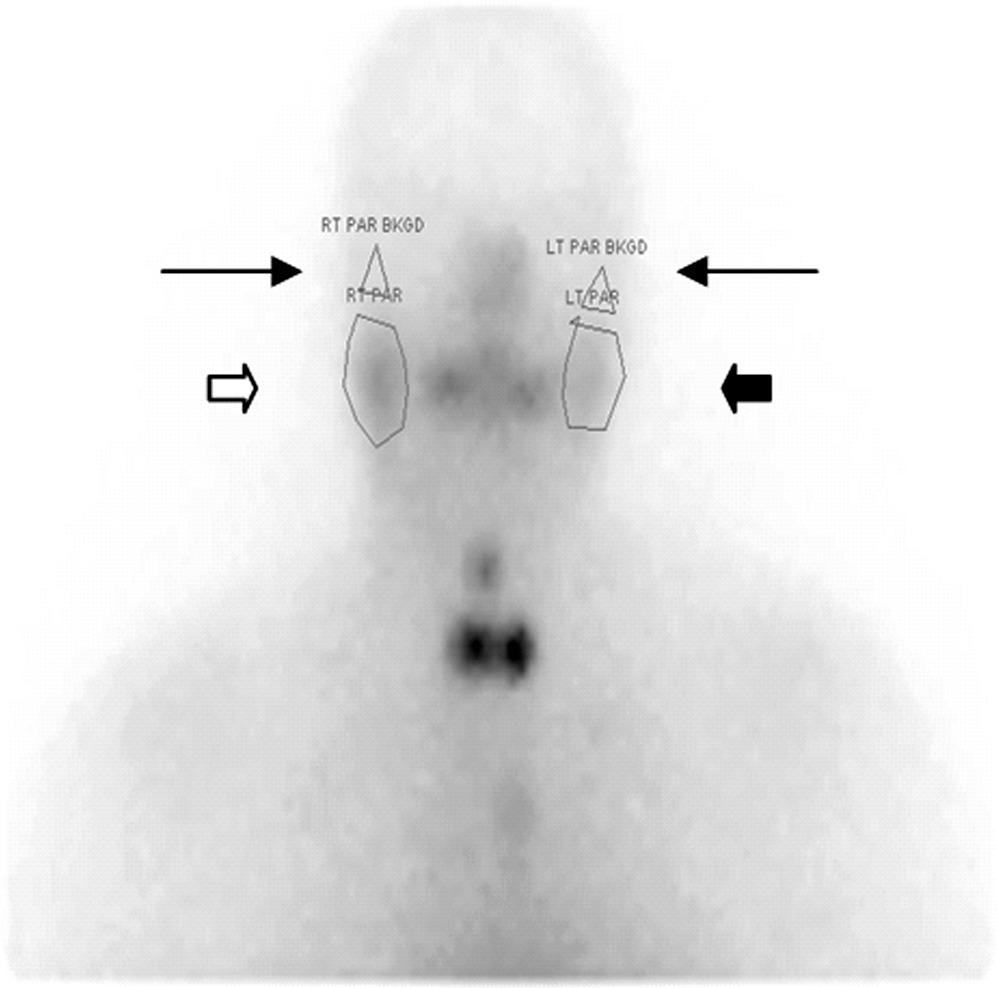
The region of interests over the right (white thick arrow) and left (black thick arrow) parotid glands are shown. The background region of interests for the right and left parotid glands are demonstrated by the thin black arrows.
Results
During the first ∼60 minutes of imaging, good uptake is visually noted in both parotid glands with greater activity in the right relative to the left (see Fig. 2), The peak activity in the right and left parotid glands was 402 and 248 counts/second, respectively. No uptake was present in either submandibular gland on the images. At no time during the total imaging time of ∼2 hours was radioactivity observed in the submandibular glands. Almost immediately (1 minute) after the administration of the lemon juice, the radioactivity within both parotid glands decreased significantly and rapidly. Relative to the peak activity, the right and left parotid gland washout was 87% and 83%, respectively. The time to the nadir of activity in the parotid glands was ∼3 minutes, and re-accumulation of radioiodine began almost immediately thereafter. Over the next ∼50 minutes of imaging, increasing radioactivity was present in both parotid glands, and by 30 and 13 minutes after the nadir the radioactivity in the right and left parotid glands, respectively, essentially equaled the initial activity prior to the administration of the lemon juice. At no time during the 50 minutes of imaging did the uptake in either parotid gland significantly exceed the pre–lemon juice levels of activity. At ∼50 minutes after the lemon juice, a significant reduction of radioactivity was again noted in both parotid glands; however, no additional sialagogues had been administered. On questioning after the study, the patient had no memory of visualizing or thinking of food. The washout relative to the activity just prior to the spontaneous salivation was 70% and 51% in the right and left parotid glands, respectively. The time to the nadir of activity in the parotid glands was ∼4–5 minutes.
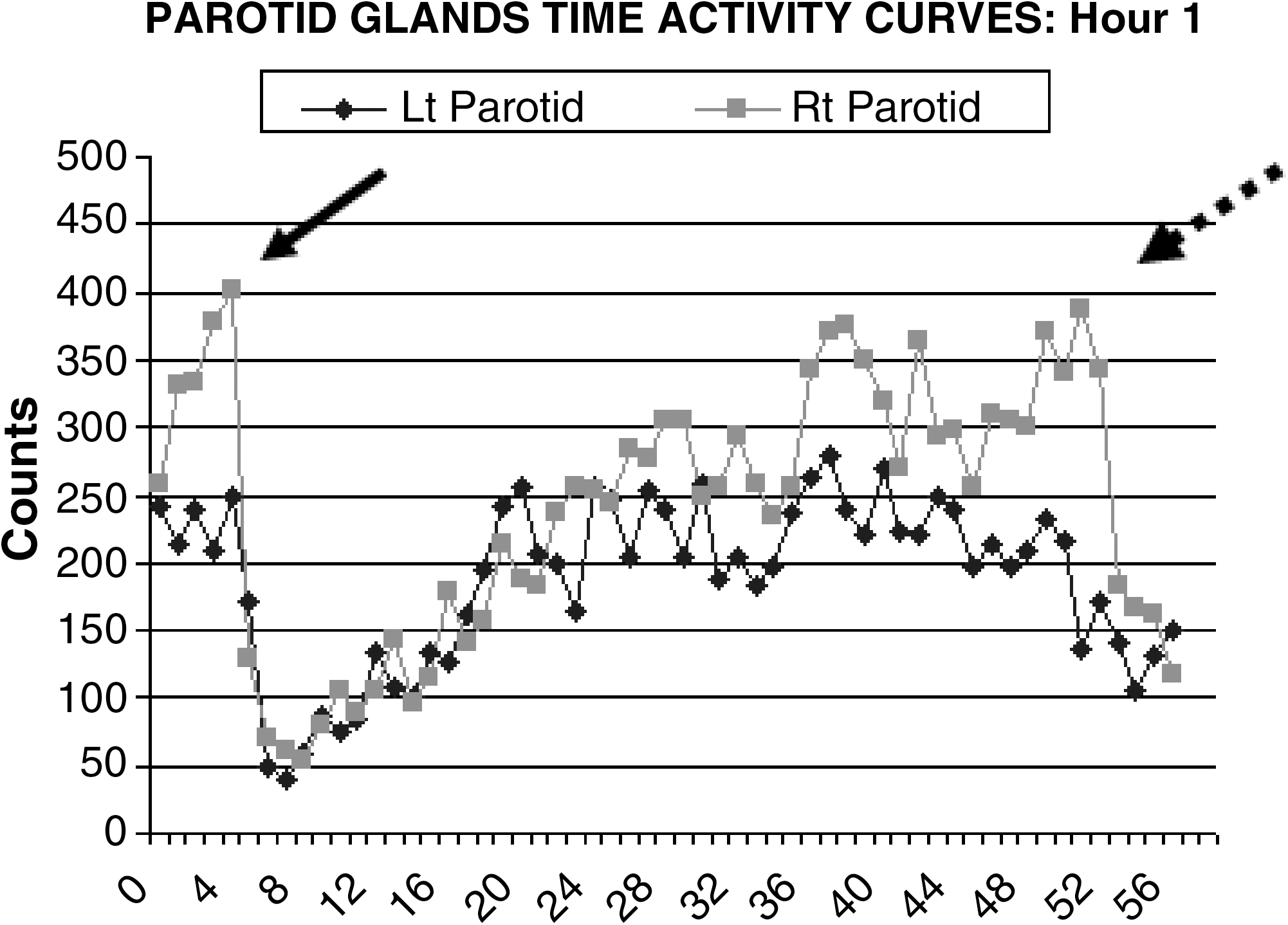
The above graphs represent the time–activity curve for the right parotid (Rt; square data points) and left parotid (Lt; diamond data points) after correction for background beginning 2 hours after the diagnostic prescribed activity of 131I was administered for the whole-body scan and dosimetry. Lemon juice was administered at 5 minutes (solid arrow) after initiation of imaging. No sialagogue was administered at 53 minutes (broken arrow), which indicates spontaneous salivation.
The second set of images were initiated shortly after the first set of images and obtained from ∼70 minutes to ∼130 minutes after initiation of the study (see Fig. 3). Peak activity in the right and left parotid glands was 307 and 292 counts/second, respectively. Shortly after the administration of the lemon juice, the radioactivity within both parotid glands again decreased significantly and rapidly. Relative to the peak activity, the right and left parotid washout was 67% and 61%, respectively. The time to the nadir of activity in the parotid glands was approximately 3–4 minutes, and the beginning of re-accumulation of radioiodine in the parotid glands began almost immediately thereafter. After each of the three subsequent administrations of additional lemon juice every 15 to 20 minutes (see Fig. 2) additional washout of radioiodine was noted. At no time during this period of imaging did the activity in the parotid glands return to the activity prior to the administration of the lemon juice for this second set of images.
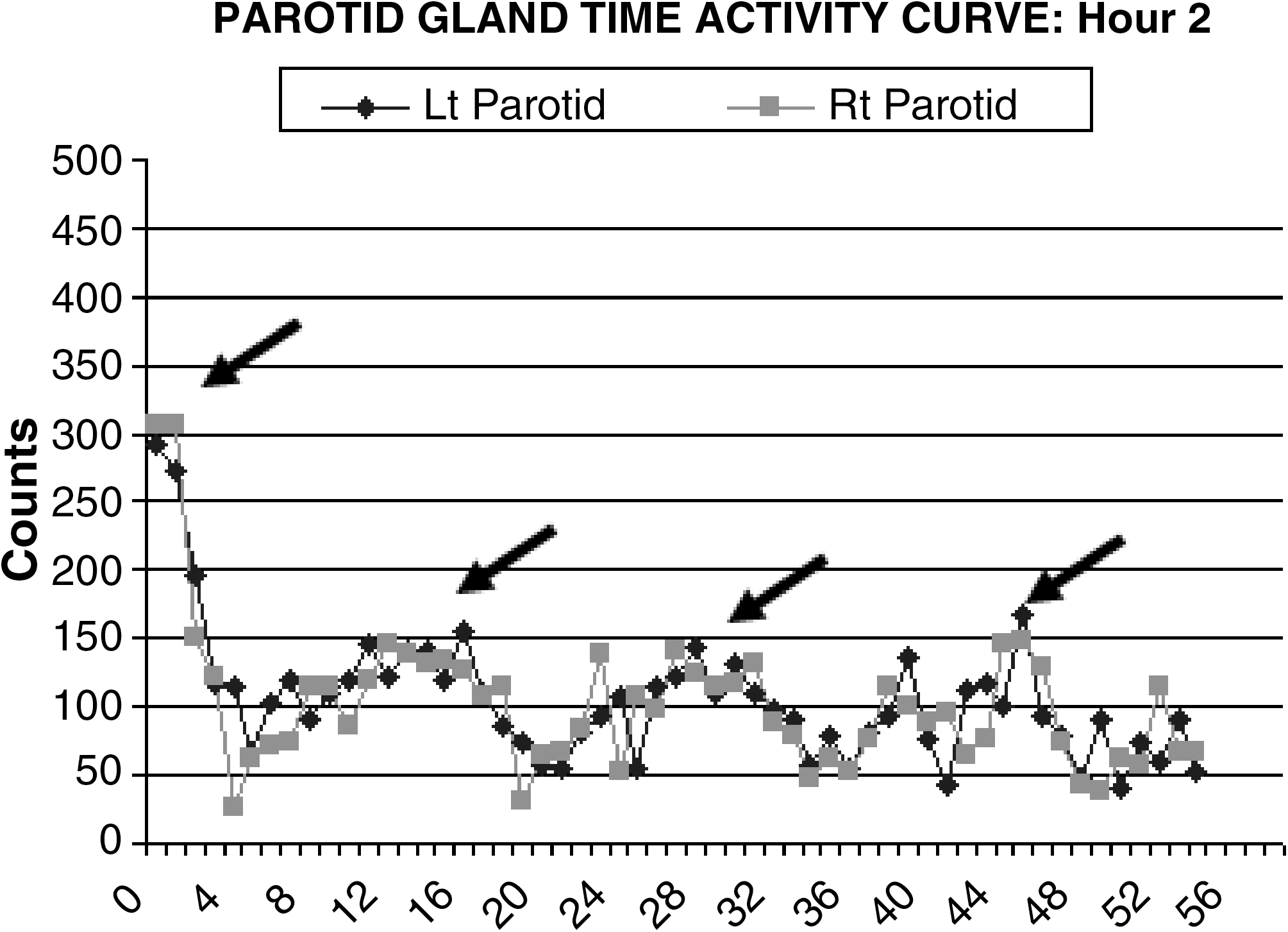
The above graphs represent the time–activity curve for the right parotid (square data points) and left parotid (diamond data points) after correction for background for the second hour of imaging, which was approximately 3 hours after the diagnostic prescribed activity of 131I was administered for the whole-body scan and dosimetry. Lemon juice was administered at the beginning of this period (first arrow) and intermittently during the next hour (subsequent arrows).
In regard to the calculation of radiation dose to the salivary glands, it is impossible to truly calculate such because we do not know the time–activity curve for the radioiodine in the salivary glands had the sialagogues not been administered. However, we calculated an estimate of the relative decrease of the area under the time–activity curve as a result of the lemon juice, and this was based on the assumption that there was no further accumulation of radioiodine up until the spontaneous salivation. Accordingly, the percent reduction in the area under of the curve of the right and left parotid glands for approximately 1 hour after the initial administration of lemon juice was 38% and 30%, respectively. The percent reduction of the area under the curve of the right and left parotid glands for the second hour after administration of lemon juice every 15–20 minutes was 67% and 61%, respectively.
Based on the patient's salivary gland scan and time–activity curves, we recommended to the patient to repeat sialagogues at approximately 30-minute intervals throughout the afternoon and evening and approximately hourly throughout the night and next day. The patient was administered 5.16 GBq (191 mCi) of 131I, and she reported following these instructions. During the next 6 months after the131I treatment, the patient reported no symptoms and had no signs of radiation-induced sialoadenitis.
Discussion
This case study demonstrates four findings.
To our knowledge, this is the first case study that uses the prescribed activity of the radioiodine for the diagnostic WBS to help assess whether or not a patient may have decreased or increased radioiodine (a rebound effect) uptake in the salivary glands in response to sialagogues. Although this patient's radioiodine was 131I, we submit that the performance of a salivary gland scan using the diagnostic dosage of 123I for WBS would be as equally effective as using 131I because the images are performed within hours after the administration of the radioiodine.
Second, this case demonstrates that the administration of lemon juice 2 hours after the administration of a diagnostic activity of 131I does not necessarily result in a rebound effect. Specifically, there was no increased radioiodine uptake in the parotid glands that was significantly higher than the uptake prior to the lemon juice for the period studied. Of course, this does not mean that there could not have been a rebound effect after imaging was stopped. However, if a rebound effect would have occurred later, it is possible that continued administration of sialagogues may have inhibited or even eliminated any subsequent rebound effect as suggested by the second set of images with multiple administrations of lemon juice.
Third, this case study also indicates that at least in one patient the administration of sialagogues reduce the retention of radioiodine for the first 2 hours, thereby reducing the radiation absorbed dose (rad or gray) to the salivary glands. This is distinctly different than increasing the potential radiation absorbed dose resulting from a rebound effect.
Finally, spontaneous salivation was demonstrated. Although salivation secondary to eating or even visualizing or thinking of food is physiologic, the observation of spontaneous salivation in this patient raises concerns regarding the recommendations of Nakada et al. (3). Patients eating and/or spontaneously salivating during the 24 hours after therapy could reduce the proposed value of avoiding sialagogues for the first 24 hours. Nakada et al. (3) did not mention if their patients were NPO for the entire period of the first 24 hours after the therapeutic administration of the radioiodine. Moreover, even if their patients had been kept NPO for 24 hours, could spontaneous salivation as demonstrated by this patient have occurred, thereby reducing the potential value of avoiding sialagogues for the first 24 hours?
Of course, there are several limitations to this report. First, this is only a case study. Second, in the attempt to estimate potential reduction in radiation absorbed dose, we assumed that there was no further increase or decrease in radioiodine activity within the parotid glands after lemon juice was administered. In fact, the radioiodine activity may have continued to increase, and if this was the case, our estimate of the true potential reduction of radiation absorbed dose secondary to the administration of the lemon juice would have been an underestimation.
So, should or shouldn't we use sialagogues during the first 24 hours after radioiodine ablation or treatment? More carefully controlled studies are needed to answer that question, and until then, we believe one should not change one's practice for three reasons. First, Nakada et al. (3) is only one report, and one should be cautious in changing practice based on only one report. Second, based on this case reported herein, at least one patient did not have a rebound effect during the time the patient was imaged. Of course, like one series, one case should not change one's practice. However, this case study does raise the question of whether sialagogues should be administered more frequently than every 2–3 hours during the daytime, which is what Nakada et al. (3) evaluated. Although no sialagogues for 24 hours may be better than sialagogues administered every 2–3 hours, sialagogues administered every half hour to one hour during the day time as well as throughout the night may be better than either withholding sialagogues for 24 hours or administration of sialagogues every 2–3 hours only during the day. Third, we do not believe that withholding sialagogues for 24 hours makes sense intuitively when patients are eating and/or spontaneously salivating. Although one could possible have the patient fast for 24 hours, one cannot control spontaneous salivation. Again, we do not believe for the above reasons that one should change one's practice regarding sialagogues at this time.
In summary, this case study demonstrates 1) an approach without the use of any additional radioiodine to assess whether or not an individual patient will have increased or decreased radioiodine uptake in the salivary glands after administration of sialagogues, 2) a decrease of radioiodine uptake in the salivary glands after lemon juice without a rebound effect, and (3) a potential decrease of radiation absorbed dose of as much as 30% to 67% with the use of sialagogues.
Footnotes
Disclosure Statement
No competing financial interests exist.