
Abstract
Background:
Midline ectopic thyroid tissue is a common pathological entity. In contrast, laterally located ectopic thyroid tissue with a normally located thyroid gland is a very rare condition in head and neck surgery.
Summary:
We report the association of laterally located multinodular thyroid tissue and a normally located multinodular goiter. A woman was seen in the otolaryngology clinic with a right submandibular mass. Clinical examination and investigations confirmed the presence of a multinodular goiter in an ectopic thyroid gland.
Conclusion:
Laterally located ectopic thyroid tissue is a very rare condition. Ectopic thyroid tissues can undergo the same pathological changes as a normally located thyroid gland. Ectopic thyroid goiter together with a normally located multinodular goiter is a rare entity, and this is the first to be reported in North America.
Introduction
We present the first patient, or one of the first patients, from North America with laterally placed multinodular thyroid tissue in association with a multinodular goiter in the usual position.
Patient
A 55-year-old woman presented with a history of a painless lateral neck mass on the right. The mass had been gradually increasing in size over 2 years. She had no other symptoms and there was no evidence of thyroid dysfunction. Her medical history was unremarkable. There was no history of exposure to radiation. The patient's mother had a history of Hashimoto thyroiditis. She had a firm, nontender right-sided neck mass in the submandibular area measuring approximately 2 × 3 cm, with no evidence of cervical lymphadenopathy. Bilateral palpable thyroid nodules were identified, without obvious communication with the right-sided neck mass. Flexible nasal endoscopy showed normal hypopharynx, and supraglottic and bilateral mobile vocal cords. The results of laboratory tests including complete blood count, thyroid-stimulating hormone (1.77 mIU/mL; normal range, 0.3–3 mIU/mL), and free thyroxine (11.83 pmol/L; normal range, 7–19 pmol/L) were all within normal limits.
A computed tomography (CT) scan (Fig. 1) revealed a 2.5 × 2.2 cm intensely enhancing rounded mass with small areas of hypoperfusion at the right side of the neck. The mass was located in the right carotid space, anteromedial to the external carotid artery, the right bifurcation, and the distal common carotid artery. The thyroid gland (Fig. 2) showed heterogeneous enhancement and no cervical adenopathy. Magnetic resonance imaging (MRI) was ordered to rule out carotid body tumor and showed (Fig. 3) no vascular flow voids. The lesion appeared to be separated from the adjacent submandibular gland and the carotid sheath. The thyroid gland on MRI showed bilateral dominant solid thyroid nodules at the lower pole of each gland measuring 3.0 × 1.7 × 3.2 cm on the right side and 1.5 × 2.1 × 2.9 cm on the left. The patient was then scheduled for an ultrasound-guided fine needle aspiration of both thyroid nodules and the neck mass. Biopsies of the thyroid masses were returned as consistent with degenerative changes, and both were negative for malignancy. The cytology of the neck mass did not suggest a lesion of thyroid origin, and was interpreted as pleomorphic adenoma.
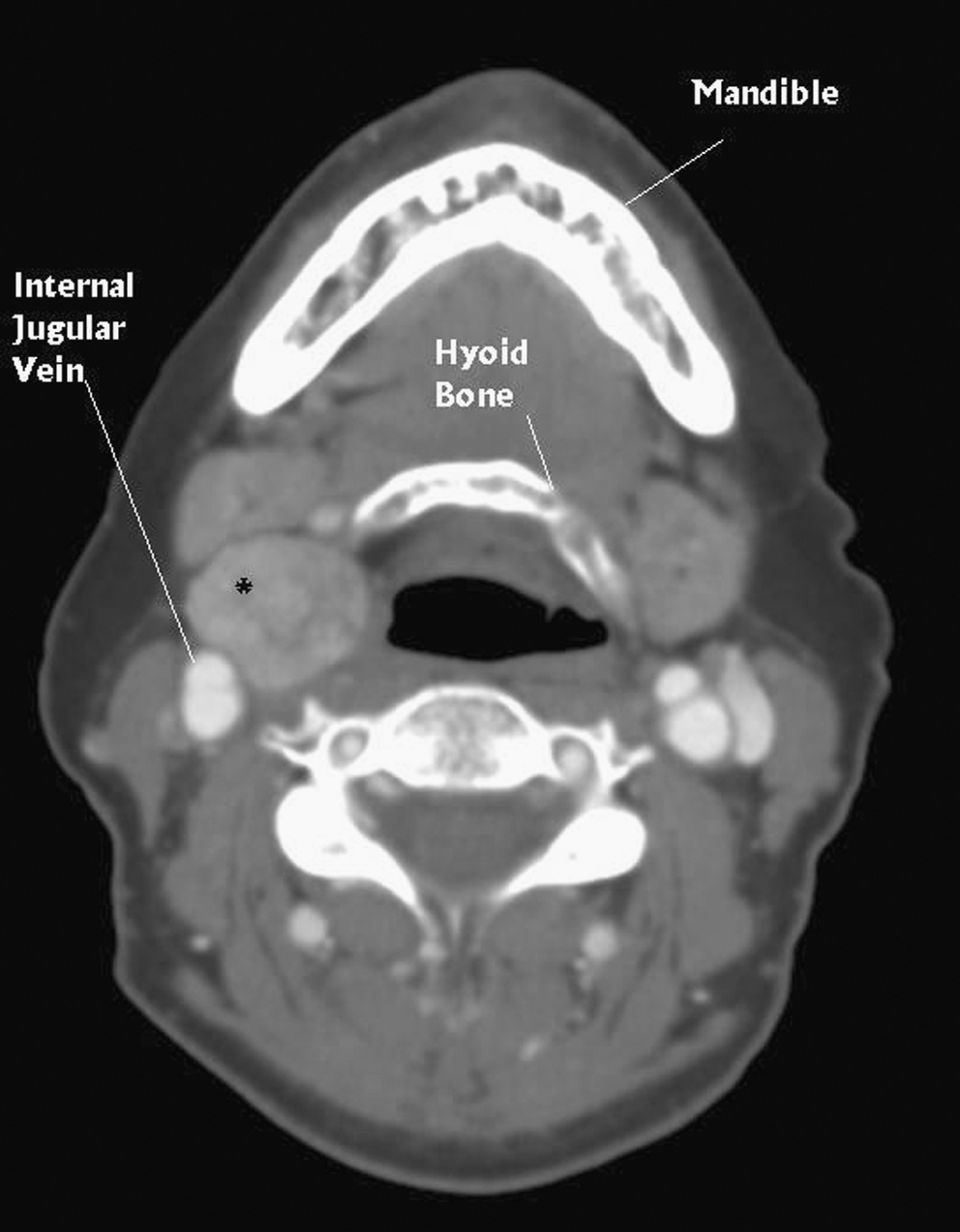
Axial computed tomography scan at the level of the hyoid bone, showing the lesion on the right side (asterisk), deep to the sternocleidomastoid muscle and just lateral to the airway.
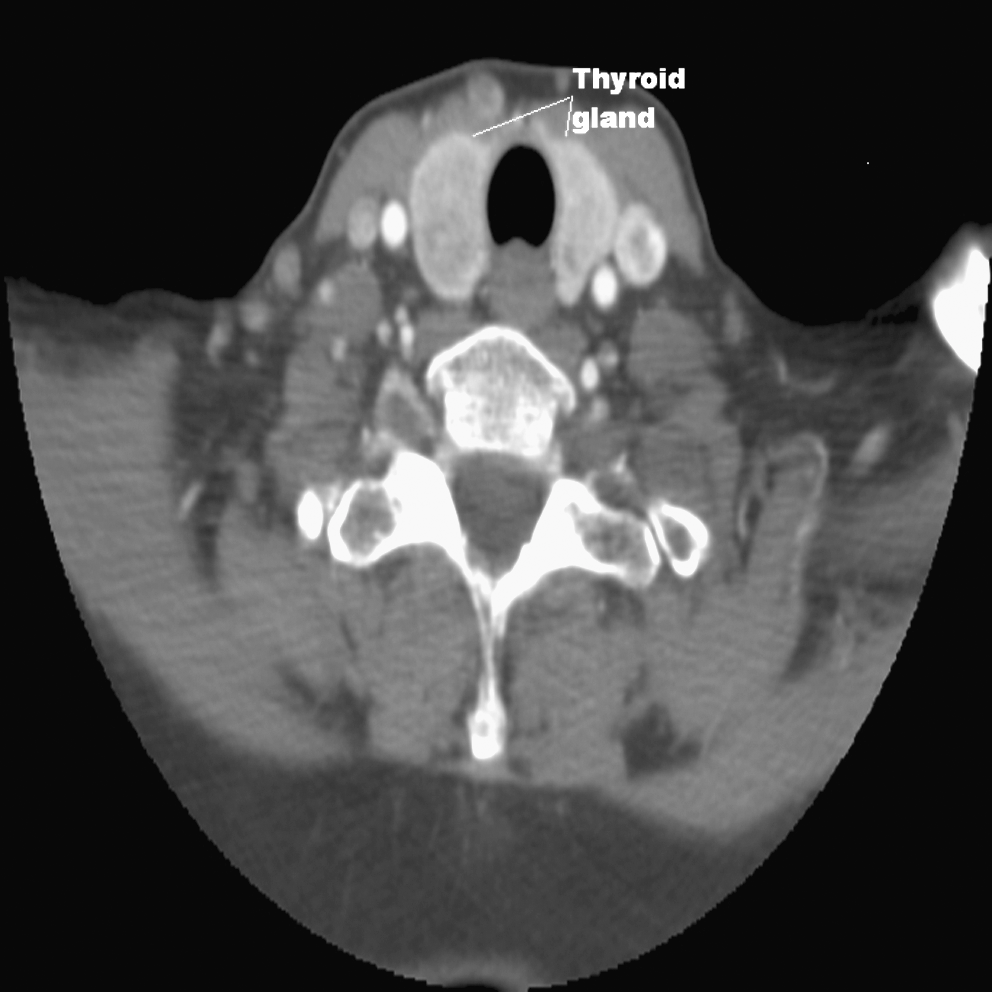
Axial computed tomography scan at the level of the thyroid gland, showing bilateral hypodensity nodules in both lobes of the gland.
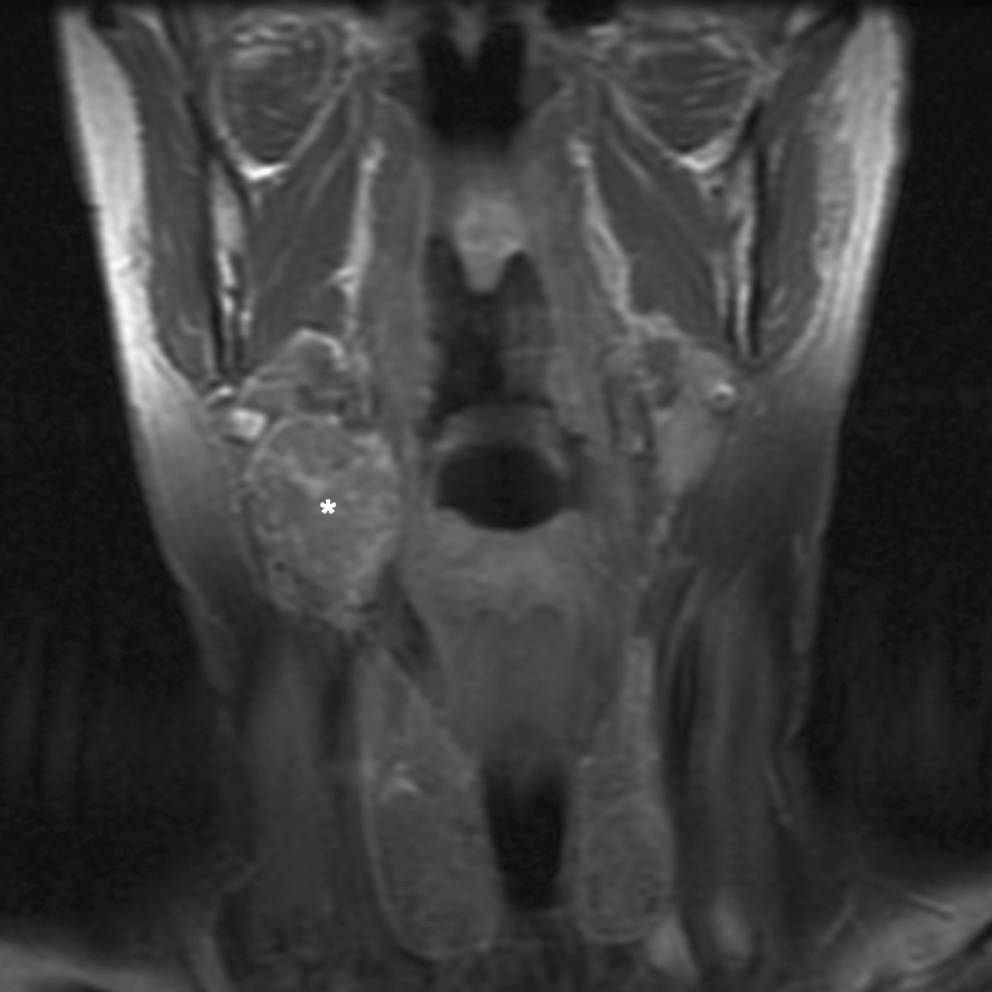
Coronal magnetic resonance image showing the ectopic thyroid mass (asterisk) on the right side and the thyroid gland. There is no obvious connection between the ectopic thyroid mass in the neck and the thyroid gland.
The patient underwent excision of the neck mass. Intraoperatively, no connection to the right superior pole of the thyroid was identified. It measured 3.5 cm in greatest dimension and on cut section contained several nodules that measured up to 1.4 cm in diameter. Microscopically, all the nodules had architectural and cytological features consistent with hyperplastic nodules (Fig. 4). A small quantity of normal thyroid tissue was noted at one edge. There was no evidence of malignancy. The postoperative course was uncomplicated and the patient was discharged home the following day.
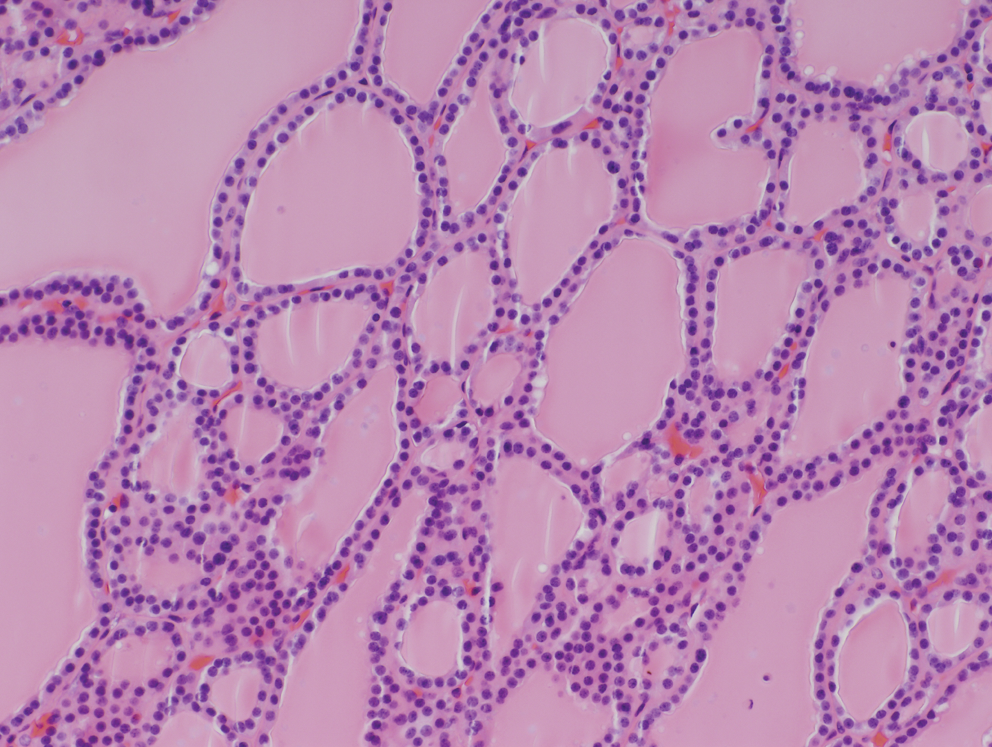
Photomicrograph of a nodule of thyroid tissue showing macrofollicles and small cysts consistent with nodular hyperplasia (hematoxylin and eosin, 40 ×). Color images available online at
Discussion
Abnormality in the development or aberrant migration of the thyroid descent will result in ectopic thyroid tissue. It is usually present in midline along the path of migration from the foramen cecum to the mediastinum. Biallelic mutations in Foxe1 have been shown to result in thyroid ectopy in mice; however, up to now, no mutation in a known gene has been associated with human ectopic thyroid tissue (8).
The first ectopic thyroid tissue was described by Hickman in 1869: it was a lingual thyroid in a 1-day-old girl (9). Helidonis described the first ectopic thyroid tissue in the submandibular region (10). In the past the term “lateral aberrant thyroid” has been used, and some examples were considered to be metastatic thyroid cancer rather than an embryonic rest. To our knowledge, the first report of a submandibular ectopic thyroid tissue presenting with a normally located thyroid was by Sambola-Cabrer et al. in 1996 (11). Since then, sporadic patients have been reported (12 –15). The prevalence of ectopic thyroid tissue is approximately 1 per 100,000–300,000 persons and occurs in 1 in 4000–8000 patients with thyroid disease (16). In 70–100% of cases with ectopic thyroid tissue, no other thyroid tissue is present (4 –7). However, according to autopsy studies, the prevalence of ectopic thyroid tissue varies between 7% and 10% (17). Ectopic thyroid tissue is more common (65–80% of all cases) in women (16).
Clinically, most ectopic thyroid patients are asymptomatic but may have symptoms of dysphagia, dysphonia, dyspnea, cough, and hemoptysis (16). Hypothyroidism has been reported to occur in 33% of patients with ectopic thyroid (2), and rates of hypothyroidism might be expected to be higher in patients with only ectopic tissue. Although the chemical structure of thyroid hormones synthesized in ectopic thyroid is normal, the amount may not be sufficient to meet the physiological demands. In such conditions, the level of thyroid-stimulating hormone increases and results in hypertrophy of the thyroid gland. The development of malignant ectopic thyroid tissue is rare but has been reported (18). About 80% of such tumors are papillary carcinoma (19). If thyroid tissue is found in the lateral cervical chain, a metastatic thyroid malignancy must be excluded. However, several diseases can lead to detached fragments of thyroid tissue in the neck that are not associated with lymph nodes, including nodular goiter and chronic thyroiditis (19).
Ectopic thyroid tissue should be considered in the diagnosis of all median and lateral cervical masses. The neck should be examined for a normally located thyroid gland. The differential diagnosis of submandibular masses includes inflammatory and malignant lymphadenopathy, salivary gland tumor, lipoma, branchial cleft cyst, sebaceous, and dermoid cyst. Cervical ultrasonography, CT, and MRI are excellent methods for evaluating the site and size of the lesion. On CT the ectopic thyroid tissue appears as a high-density mass due to its high iodide content. Thyroid scintigraphy with 123I or Technetium-99m is highly sensitive and specific in detecting normal and ectopic thyroid tissue. It can differentiate tongue and neck ectopic thyroid mass from other causes of neck mass
Ultrasound-guided fine needle aspiration for extrathyroidal neck masses is simple and in experienced hands has an accuracy of >90% (20). Ectopic thyroid tissue should be considered in the evaluation of any neck mass, despite the presence of a normally located thyroid gland. Ectopic thyroid goiter in association with normally located multinodular goiter is very rare. To our knowledge, this is the first patient reported in North America.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.