
Abstract

Graves' ophthalmopathy (GO) (Thyroid–Associated Ophthalmopathy, Graves' Orbitopathy) may present before the development of thyrotoxicosis, concomitant with the development of thyrotoxicosis, or after the treatment of thyrotoxicosis. In some patients with Graves' disease (GD) the onset or worsening of GO appears to coincide with the development of the euthyroid state or hypothyroidism after treatment of thyrotoxicosis, suggesting the hypothesis that marked decline in thyroid hormones aggravates GO (1). Struma ovarii (SO), a rare disorder, and GD are both causes of autonomous thyroid hormone production. They have been reported in the same patient though GO was not a prominent feature of most of these reports (2 –4). Here we report a distinctly unusual patient with GD and malignant SO who was first treated for thyrotoxicosis due to GD and then treated for SO and whose onset of severe GO occurred after the latter treatment.
A 44-year-old female teacher was seen in July 2006 for hyperthyroidism. She presented with 6 months history of significant weight loss (22 kg), palpitations, sweating, and emotional lability. Physical examination revealed a diffusely enlarged goiter with audible bruit, GO (NOSPECS* class 3: lid retraction, proptosis, chemosis), tachycardia, and proximal myopathy. Investigation confirmed hyperthyroidism: serum-free thyroxine (FT4) 3.65 ng/dL (normal range 0.62–1.7 ng/dL), serum-free triiodothyronine (FT3) 2545 pg/dL (normal range 162–390 pg/dL), and thyrotropin (TSH) <0.005 mU/L (normal range 0.30–4.0 mU/L). Technetium thyroid scan showed diffuse uptake. The thyrotropin receptor antibody (TRAb) measured 36 U/L (normal level <1 U/L). She was diagnosed as having GD and started on carbimazole 10 mg t.i.d. and metoprolol 50 mg b.i.d.
Three months later, she remained hyperthyroid with persistently elevated serum FT4 3.2 ng/dL, FT3 2304 pg/dL, and suppressed TSH. Total thyroidectomy was performed in November 2006. She was prepared for thyroidectomy with 10 days of oral Lugol's iodine. Her surgery was performed by a senior endocrine surgeon and was uneventful. Histology confirmed GD. She was started on thyroxine replacement therapy, initially at a dose of 100 μg daily on weekdays and 150 μg daily on weekends. Two months after surgery, her TSH remained persistently suppressed, and the dose was reduced to 100 μg daily on weekdays and 50 μg daily on weekends. Subsequently, monitoring of thyroid function tests (TFTs) revealed that in May 2007 they remained abnormal (serum FT4 1.6 ng/dL, FT3 424 pg/dL, TSH suppressed) despite further reduction in the dose of thyroxine.
While she complained of intermittent pelvic pain soon after the diagnosis of GD, investigations were delayed until 2 months after thyroid surgery. Ultrasound revealed two cystic lesions within the left ovary. These cysts were persistent on follow-up ultrasonography and felt to be atypical, hence a left salpingo-oophorectomy was performed in May 2007. Histology (Fig. 1) demonstrated SO with malignant features favoring papillary thyroid cancer (follicular variant) but with no metastatic seeding in peritoneal washing or omentum.
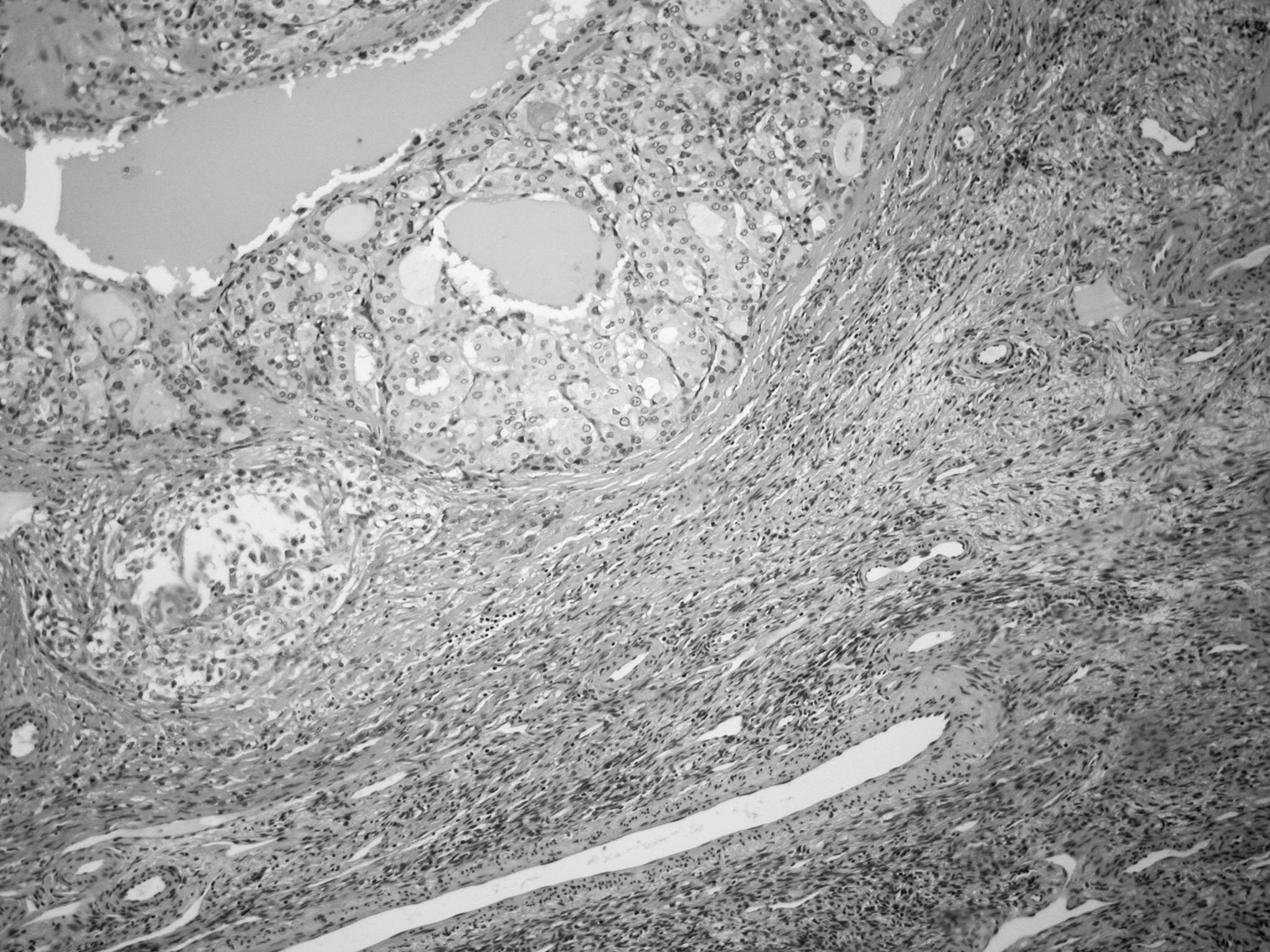
Histology of the left ovary demonstrating papillary thyroid cancer, follicular variant (top left) adjacent to normal ovarian tissue (bottom right).
In July 2007 (8 months after thyroidectomy and 2 months after treatment of SO), she presented with fulminant GO consisting of chemosis, ophthalmoplegia, and left ocular papilloedema (NOSPECS class 6). Orbital computed tomography scan (Fig. 2) demonstrated bilateral marked swelling of the extraocular muscles and left optic nerve compression. Unfortunately TFTs were not obtained at this time but results from a month prior revealed serum FT4 0.9 ng/dL, FT3 182 pg/dL, and with TSH 7 mU/L.

Sagittal and transverse imaging of the orbits: bilateral marked swelling of the extraocular muscles.
She was treated initially with 5 days of intravenous methylprednisolone 500 mg daily and subcutaneous octreotide 50 μg t.i.d., which was followed by maintenance dose of oral prednisolone 40 mg daily. Partial response to the medical treatment was noted, with resolution of papilloedema but incomplete improvement of ocular movement and persistent proptosis. She required bilateral orbital decompression in October 2007.
Three months later (November 2007), following stabilization of her ocular condition, she was treated with radioactive I131 108 mCi. Subsequently, a right salpingo-oophorectomy and hysterectomy was performed (April 2008). Histology excluded any evidence of malignancy. She recovered well but has residual restricted lateral and upward gaze and receiving thyroxine replacement 150 μg daily on weekdays and 100 μg daily on weekends. The latest TFTs were normal (serum TSH 2.2 mU/L and TSH receptor Ab 10 U/L).
Our patient clearly had GD evident by clinical, biochemical, and imaging findings. Incidentally, SO with malignant papillary carcinoma, follicular variant was diagnosed postoperatively. SO is a rare ovarian teratoma that contains more than 50% thyroid tissue. There are less than 500 reported cases in the literature (2). It accounts for <1% of all the ovarian tumors. Approximately 40% of the SO are associated with a cervical goiter, but SO with concurrent GD is extremely rare (3). SO is more prevalent in countries where goiter is endemic (4), and in patients between 40 and 60 years. It is a benign disorder in more than 90% of the cases. Patients are usually asymptomatic with only 8% of the SO presenting with thyrotoxicosis. Thyroid tissue in SO is no different than cervical thyroid tissue. It is difficult to diagnose GD-like changes in SO as the pathognomonic histological features are absent (5).
Interestingly despite having had a thyroidectomy, her TSH was persistently suppressed, requiring a dose reduction of her thyroxine to a level less than that expected for her body weight, from 100 μg daily weekdays/150 μg daily weekends down to 100 μg daily weekdays/50 μg daily weekends. This is equivalent to a dose reduction of 1.3 μg/kg/day down to 0.9 μg/kg/day. Despite these changes, her FT3 appeared to be rising (424 pg/dL, normal range 162–390 pg/dL) at 6 months postoperatively. The next TFTs after left salpingo-oophorectomy were consistent with subclinical hypothyroidism (serum TSH 7 mU/L). The following month, she presented with fulminant and progressive GO (NOSPECS class 3 to class 6).
We presumed that our patient's SO was functional, given the persistent suppressed serum TSH despite total thyroidectomy and the fact that she developed hypothyroidism after removal by left oophorectomy of the SO. While the thyroxine replacement may have been in excess, this is less likely as the requirement dose was much less than predicted in patients after total thyroidectomy. The functionality of SO has been shown in previous studies by detection of triiodothyronine, thyroxine, and thyroglobulin but in the presence of concomitant GD, it is difficult to elucidate. Teale et al. (6) demonstrated the presence of TSH receptors in SO of their patient using immunohistochemical staining. Their data suggest that the TRAb of GD could be stimulating SO growth and function.
To our knowledge this is the first published case of worsening of GO after total thyroidectomy and removal of a SO. The pathogenesis of GO is unclear. GO is widely known to be an autoimmune disorder and the TSH receptor has been suggested to be a source of antigen as it is present in the orbital tissue and thyroid (7). The possibility of TRAb production by SO or stimulation of TRAb production by SO is unknown. Our patient developed fulminant GO after removal of the source of TRAb (thyroidectomy and oophorectomy). The transient mild hypothyroidism after surgery may have contributed to the GO flare, as has been reported previously (8). However, this is only a theory and the degree of hypothyroidism was only mild.
To date there is no consensus on the surgical and postoperative management of malignant SO (papillary thyroid cancer of follicular variant in our patient). Treatment options include total abdominal hysterectomy and oophorectomy and near total thyroidectomy. These measures enable monitoring of thyroglobulin levels for recurrence of disease (9,10). Our patient has received that therapy although in reverse order. Our plans are to follow her prospectively with serial thyroglobulin assays and radioactive iodine imaging and perhaps other forms of imaging if indicated (computed tomography [CT], magnetic resonance imaging [MRI], and positron emission tomography [PET] scans). This case highlights the unique coexistence between malignant SO and GD as well as development of GO flare-up after thyroidectomy and oophorectomy; the cause of which is unknown and not been reported previously.
Footnotes
A preliminary report of this was presented at Endocrine Society of Australia, Clinical Weekend Conference, August 22–24, 2008.
*
In 1969, the American Thyroid Association adopted the formal classification of Ocular Graves' disease, represented by the mnemonic NOSPECS. The disease process passes through 6 stages: (0) No signs or symptoms present; (I) Only symptoms of ocular irritation (dryness, tearing, foreign body sensation); (II) Soft tissue involvement (periorbital edema); (III) Proptosis; (IV) Extraocular muscle involvement (ophthalmoplegia); (V) Corneal involvement (dense punctate epitheliopathy, infiltration, and ulceration); (VI) Sight loss with or without visual field compromise secondary to compressive optic neuropathy. However, because the disease is recognized as variable, the formal classification was revised in 1974 to range from no manifestations to mild, moderate, or severe manifestations.